
Abstract

The recently published Psychodynamic Diagnostic Manual (PDM; PDM Task Force 2006) proposes a diagnostic system with three axes: an S-axis with phenomenological descriptions of symptom patterns; a P-axis with different personality types underlain by the anaclitic and introjective personality dimensions; and an M-axis with descriptions of different profiles of mental functioning. This poster focuses on the interconnected-ness of the P- and the S-axis. More specifically, the hypothesis is tested that the anaclitic interpersonal dimension is associated with hysterical symptom patterns (somatoform disorders and phobias on the S-axis) and that the introjective interpersonal dimension is associated with obsessive-compulsive symptom patterns (see Figure 1, based on the PDM, pp. 544–545). Recently, Desmet et al. (2008) correlated scores on the Inventory of Interpersonal Problems (IIP-64; Horowitz et al. 2000) with clinical ratings on the anaclitic and introjective personality styles, and specified an anaclitic and an introjective IIP profile. The anaclitic profile was marked by high scores on the nonassertive, overly accommodating, and self-sacrificing IIP scales; the introjective profile by high scores on the vindictive and cold IIP scales. Yet when the authors then tested whether these IIP profiles were associated with the predicted symptom patterns, their findings did not confirm the hypotheses.
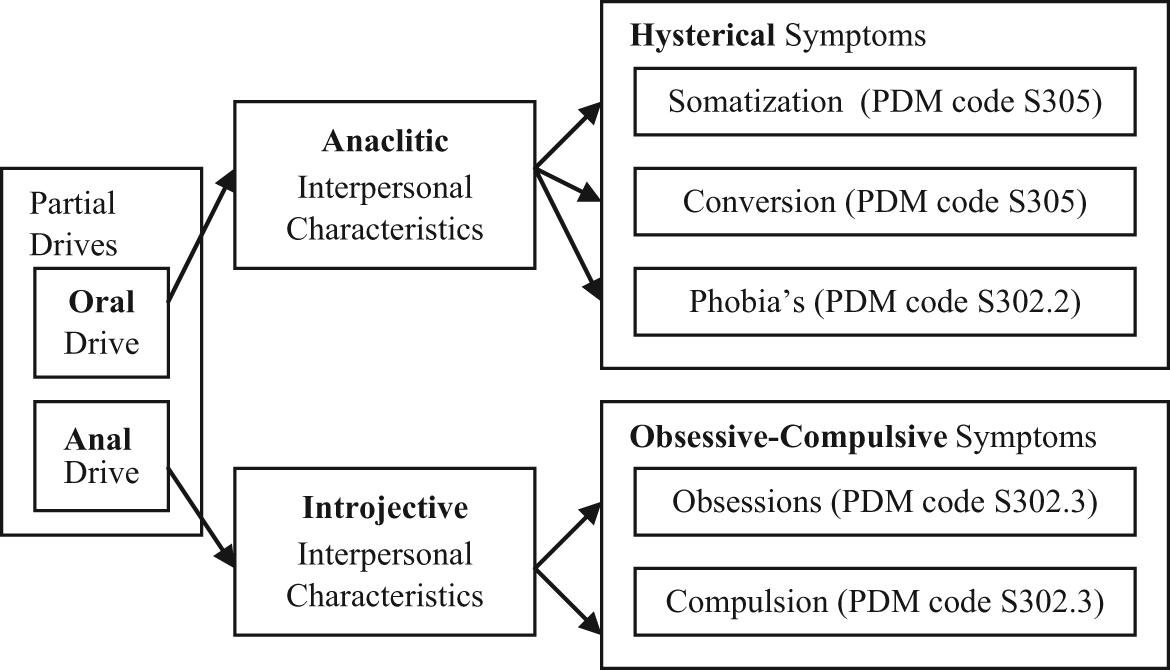
Theoretical associations between partial drives, interpersonal orientations, and neurotic symptoms (operationalizations in parentheses)
This study presents an alternative test of these hypotheses. In the earlier study, Desmet and colleagues used the Symptom Check List (SCL-90-R; Derogatis 1992) to measure hysterical and obsessional symptom patterns. But because psychometric research has shown this questionnaire to be inadequate in distinguishing different types of symptoms (Vassend and Skrondal 1999), the present study assesses patients’ symptom patterns thus: first we used structured diagnostic interviews to select small groups of patients with either a purely hysterical or a purely obsessive-compulsive symptom pattern; we then tested whether or not the theoretically predicted interpersonal profiles were observed in the two groups.
Method
Participants and procedure. Westen’s Clinical Diagnostic Interview (CDI) and the SCID-I (appropriate since the PDM’s S-axis matches axis I of DSM-IV) were used to screen at intake the symptom patterns of outpatients of a private psychotherapy practice. The first four patients (2 women, 2 men) with purely hysterical symptom patterns and the first four patients (2 women, 2 men) with purely obsessive-compulsive symptom patterns were selected.
Materials. The IIP-64 is a 64-item self-report questionnaire designed to assess interpersonal problems using 0 to 4 Likert scales. Eight subscales are correlated as a circumplex: domineering, vindictive, cold, socially inhibited, nonassertive, overly accommodating, self-sacrificing, and intrusive.
Results
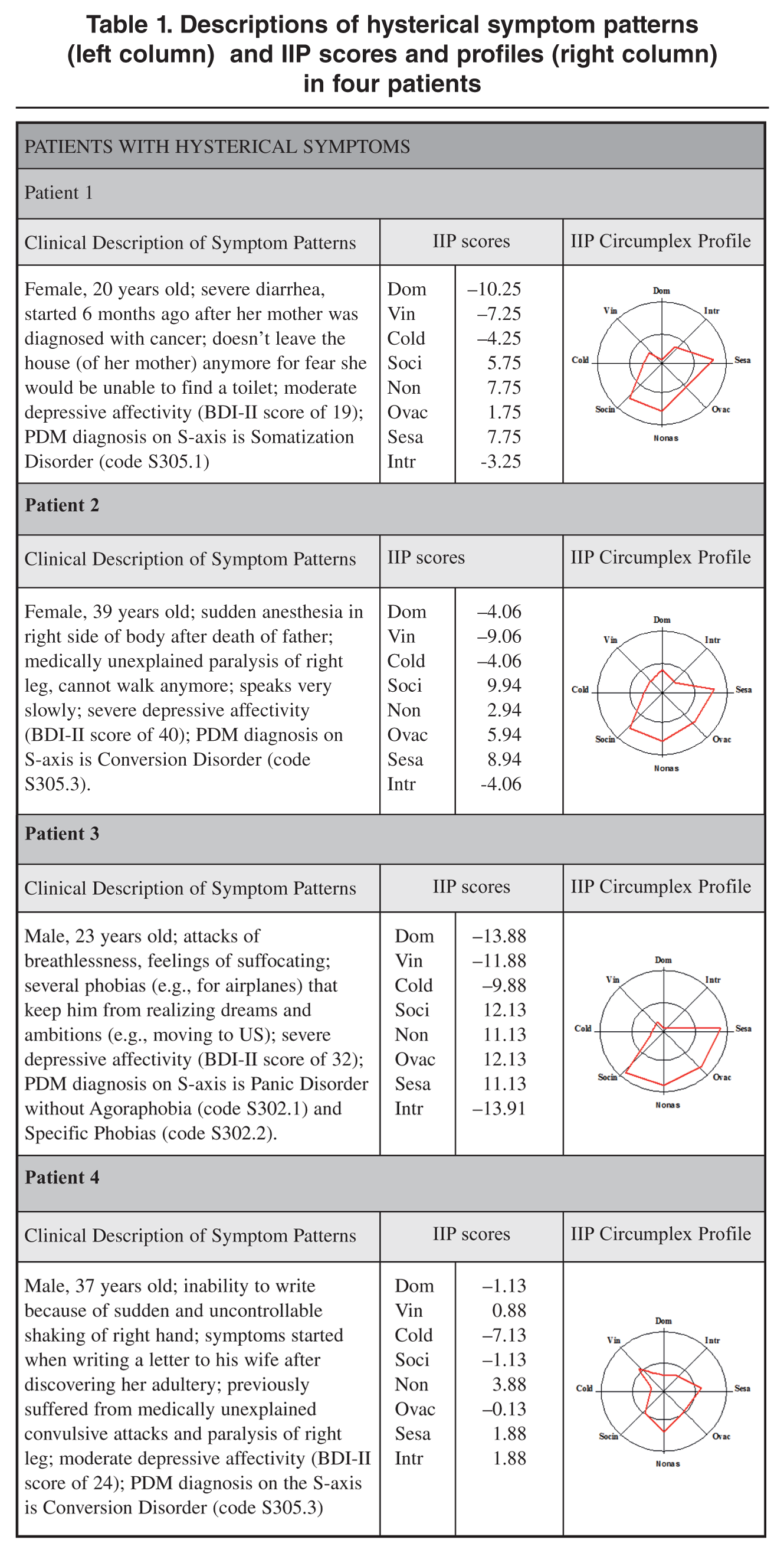
Descriptions of hysterical symptom patterns (left column) and IIP scores and profiles (right column) in four patients
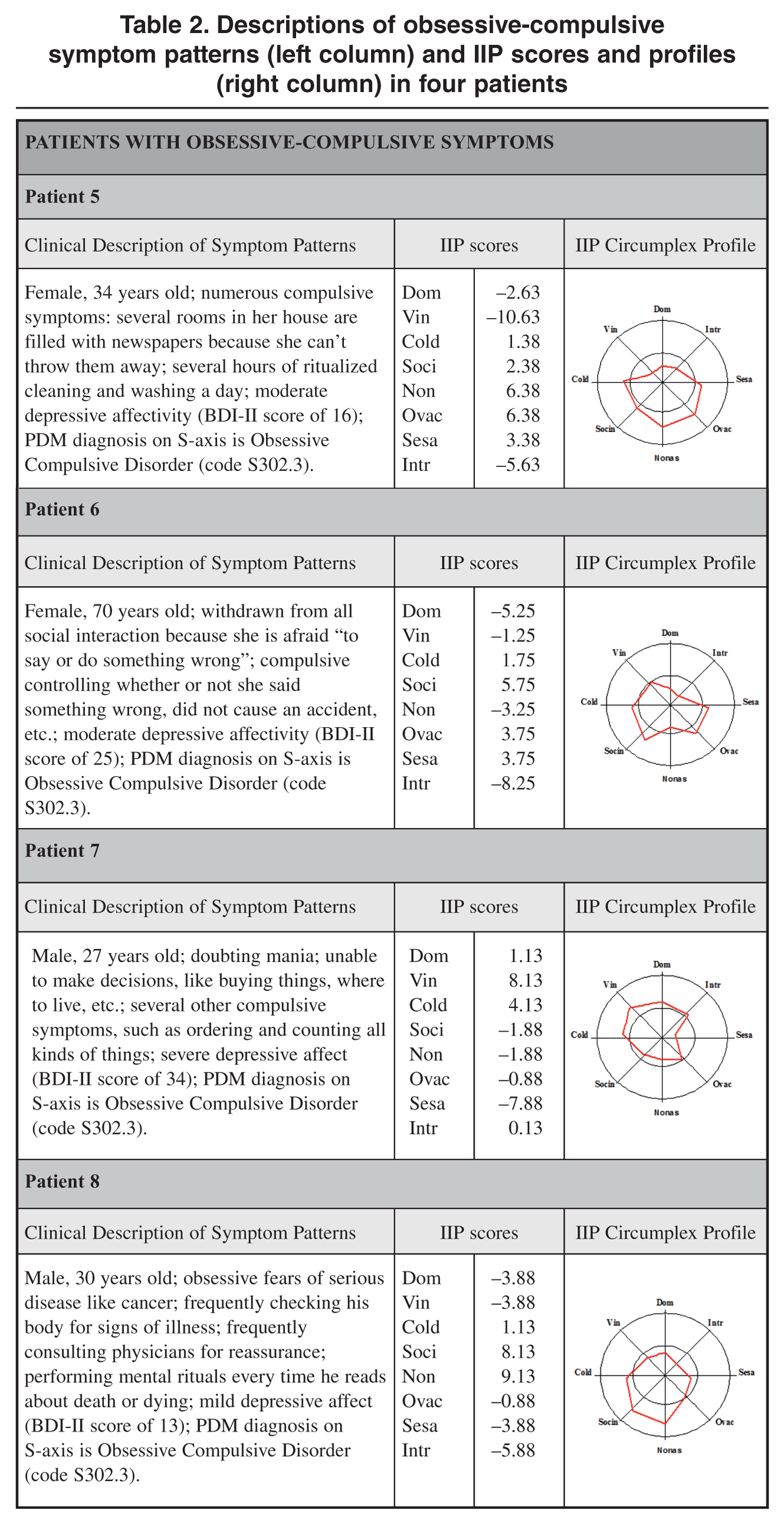
Descriptions of obsessive-compulsive symptom patterns (left column) and IIP scores and profiles (right column) in four patients
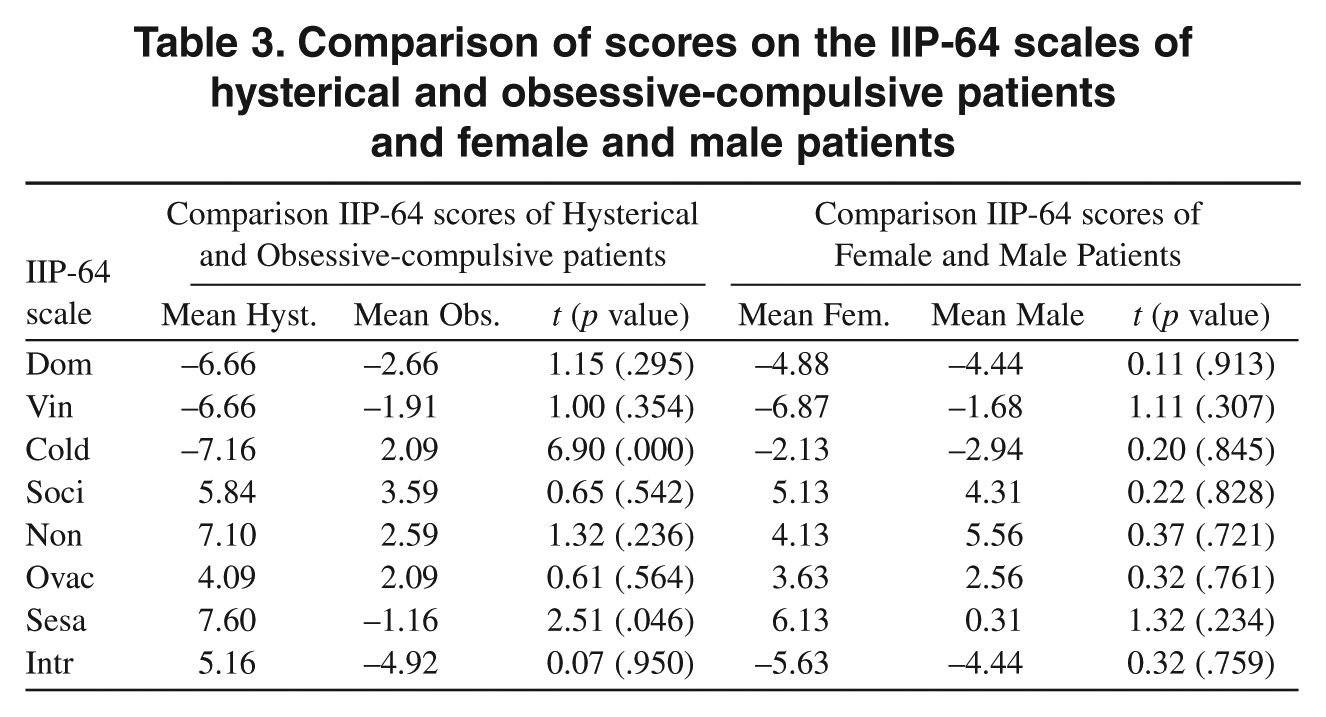
In line with our hypotheses, Table 3 shows that patients with hysterical symptom patterns scored higher on the nonassertive, overly accommodating, and self-sacrificing IIP scales; patients with obsessional symptom patterns scored higher on the vindictive and cold IIP scales. However, the difference between hysterical and obsessive-compulsive patients reached significance only on the self-sacrificing and the cold scales. No differences were found between the IIP scores of men and women.
Comparison of scores on the IIP-64 scales of hysterical and obsessive-compulsive patients and female and male patients
Conclusion
Our results confirm the hypothesized associations between the anaclitic and introjective interpersonal dimensions (P-axis) and hysterical and obsessive-compulsive symptom patterns (S-axis), respectively, put forward in the PDM. At the methodological level, this study confirms the validity of the IIP-64 as a measure of anaclitic and introjective interpersonal dimensions and the necessity of extensive clinical interviewing over and above the use of self-report questionnaires to map the symptom patterns of patients. Shortcomings of the present study are associated with the more clinical approach of selecting patients with pure symptom patterns, which almost inevitably entails smaller samples. For this reason, future research should try to replicate our findings in larger samples before firm conclusions are drawn.