
Abstract
Despite high rates of nonmarital childbearing in the United States, little is known about the health of women who have nonmarital births. We use data from the NLSY79 to examine differences in age 40 self-assessed health between women who had a premarital birth and those whose first birth occurred within marriage. We then differentiate women with a premarital first birth according to their subsequent union histories and estimate the effect of marrying or cohabiting versus remaining never-married on midlife self-assessed health. We pay particular attention to the paternity status of a mother’s partner and the stability of marital unions. To partially address selection bias, we employ multivariate propensity score techniques. Results suggest that premarital childbearing is negatively associated with midlife health for white and black women, but not for Hispanic women. We find no evidence that the negative health consequences of nonmarital childbearing are mitigated by either marriage or cohabitation for black women. For other women, only enduring marriage to the child’s biological father is associated with better health than remaining unpartnered.
Nonmarital births have increased in number and as a share of all births over the past few decades (Hamilton, Martin, and Ventura 2009; Ventura and Bachrach 2000), and nonmarital childbearing is strongly associated with social and economic disadvantage (U.S. Census Bureau 2007). Despite an explosion of research on socioeconomic disparities in health in recent years, consequences of nonmarital childbearing for women’s health in the United States have been largely overlooked. Most of what we know comes from European countries (Shouls et al. 1999; Westin and Westerling 2006; Whitehead, Burstrom, and Diderichsen 2000), but these countries’ broader social safety nets and different norms likely buffer negative consequences of nonmarital childbearing (Ozawa 2004; Waldfogel 2001). Using data from the 1979 cohort of the National Longitudinal Survey of Youth (Bureau of Labor Statistics, Department of Labor 2009), we compare midlife self-assessed health of women whose first birth was nonmarital to that of women whose first birth occurred in marriage, giving attention to potential racial/ethnic differences. If nonmarital childbearing is associated with less favorable health at midlife, it is important to identify later life events or transitions that might improve the health of such women. Within the broad array of possible factors, we focus on one with substantial policy relevance: marriage.
Decades of research indicate that, on average, marriage is associated with a range of positive health outcomes (Waite and Gallagher 2000). Findings of marital status differences in health and mortality resonate with cultural beliefs about the importance of marriage and contribute to the view that marriage is a panacea for a range of individual and societal ills. In fact, social science research on marital status differences in health is often cited in support of government policies encouraging disadvantaged single mothers to wed (Nock 2005).
Lacking direct empirical evidence, however, average health advantages conferred by marriage cannot be generalized to particular subgroups. This is especially true for women who have nonmarital births, because they are far from average by any number of metrics (e.g., poverty rates and the probability of marrying). It is unclear whether subsequent marriage offers measurable benefits to the health of women who had a premarital birth, or if, in some cases, marriage might pose health risks. Investigating this question is the second and central aim of our study. Focusing on women who had a nonmarital first birth, we compare midlife health of women who subsequently marry or cohabit with that of their continually never-married counterparts. We distinguish unions with a child’s biological father from those with a new partner, and marriages that dissolve from those that endure. Placing these questions within an ecological framework, we specifically consider whether race/ethnicity moderates these patterns. Finally, we employ multivariate propensity score matching to address differential selection of women into single motherhood and, among women who had a nonmarital birth, selection into particular union statuses.
Nonmarital Childbearing and Women’s Health
Nonmarital childbearing is an increasingly normative pathway to family formation in the United States. In 1979, only 17.1 percent of all births were to unmarried women, but by 2007 that figure had risen to 39.7 percent (Hamilton et al. 2009; Ventura and Bachrach 2000). The rapid increase and sustained prevalence of nonmarital childbearing in the United States highlights the importance of understanding its consequences for adult health and well-being. Furthermore, consequences of nonmarital childbearing for the production of inequality across multiple domains (McLanahan and Percheski 2008) suggest that it may contribute to the formation and maintenance of social disparities in population health, a topic of considerable interest in recent years. Yet we know surprisingly little about the health of single mothers—a large and particularly vulnerable segment of the U.S. population.
There are several reasons to expect that nonmarital childbearing will be associated with poor health among women in the United States. The economic toll of nonmarital childbearing is well-established, and socioeconomic status is, in turn, a fundamental determinant of health (Link and Phelan 1995). Among never-married mothers with minor children, 41 percent live below the poverty line (U.S. Census Bureau 2007), and single mother households accounted for 70 percent of all families receiving Temporary Assistance for Needy Families (TANF) in 2009 (Irving 2010). Economic disadvantages associated with single motherhood persist into later life: women who spend 10 or more years raising dependent children outside of marriage are 55 percent more likely to live in poverty when age 65 to 75 than are women who were married while raising their children (Johnson and Favreault 2004).
Nonmarital childbearing is associated with exposure to numerous other stressors that may further compromise health. Compared with married mothers, single mothers report higher levels of chronic strain and more stressful life events (Avison, Ali, and Walters 2007; Barrett and Turner 2005; Cairney et al. 2003), fewer health-protective psychosocial resources such as social support (Cairney et al. 2003), and higher levels of psychological distress (Avison et al. 2007; Demo and Acock 1996; Hope, Power, and Rodgers 1999; Wang 2004). Stress, social isolation, and psychological distress are, in turn, strongly and negatively associated with physical health (Cornwell and Waite 2009; Mulatu and Schooler 2002).
A growing body of European research finds associations between nonmarital births and mothers’ poor health. In Britain (Benzeval 1998; Shouls et al. 1999; Whitehead et al. 2000), Norway (Elstad 1996), Finland (Martikainen 1995), and Sweden (Westin and Westerling 2006; Whitehead et al. 2000), single mothers have significantly worse health than do partnered mothers. Many of these countries provide lengthy paid maternity leaves, free or highly subsidized childcare up to age 5, and universal access to health care for adults and children (Ozawa 2004; Ray, Gornick, and Schmitt 2008). In the United States, only half of women working in the private sector are eligible for 12 weeks of unpaid maternity leave, and subsidized childcare is provided only to very low-income families (Ozawa 2004; Waldfogel 2001). The relative lack of a social safety net makes it especially likely that nonmarital childbearing has negative health consequences for women in the United States.
Only one prior study directly examines the health of never-married mothers in a nationally representative sample of U.S. adults. Using data from the Health and Retirement Study (HRS) 1931 to 1941 birth cohort, Henretta (2007) finds that women whose first birth was nonmarital had a greater hazard of early death (before age 61 to 71 years) and were more likely to be diagnosed with heart disease and stroke than were women whose first birth occurred within a marriage. As Henretta notes, however, these findings may not be generalizable to more recent cohorts for whom nonmarital births are more common and less stigmatized. We use data from a nationally representative group of women born in the United States between 1957 and 1965 to compare midlife self-assessed health of women whose first birth was nonmarital to that of women whose first birth occurred within marriage. Because mortality is relatively rare for these more recent birth cohorts, we predict midlife self-assessed health—a measure that strongly predicts mortality later in life (Idler and Benjamini 1997).
Our analyses give particular attention to mothers’ racial/ethnic background. Blacks, whites, and Hispanics have starkly varied rates of nonmarital childbearing (Ventura and Bachrach 2000), as well as different ecological and cultural contexts within which they frame their lives and draw support (Heard 2007). Substantial evidence casts doubt on the dominant cultural belief that early childbearing has widespread individual and social costs for low-income black women (Geronimus 2003). As Geronimus (1996) shows, early fertility may be an adaptive strategy for low-income, urban black women vulnerable to weathering, that is, accelerated declines in health that pose substantial challenges to bearing and raising children at older ages. Although prior research has not considered whether similar considerations apply to nonmarital childbearing and its consequences for black women’s physical health, several studies show that black mothers and their offspring are not as negatively affected by nonmarital childbearing as their white counterparts on other dimensions of well-being (Fomby and Cherlin 2007; Furstenberg 2007; Heard 2007). On the other hand, evidence that blacks have more difficulty than whites accessing high-quality health care services (Smedley, Stith, and Nelson 2003) could mean that black women may be especially vulnerable to any long-term negative health consequences of nonmarital childbearing. Although this countervailing evidence does not support strong directional hypotheses, demographic and ecological factors warrant consideration of potential racial/ethnic differences.
In summary, if the strains of single motherhood lead to poor health, the increasing prevalence of nonmarital births in the United States represents a substantial public health threat that has been largely ignored. Growing numbers of women are entering midlife, when health problems begin to emerge, having experienced cumulative strains associated with nonmarital childbearing. This is especially important because of the links between events and transitions across an individual’s life course and across generations (Elder 1988). Specifically, mothers’ poor health can have enduring consequences for their children by increasing children’s risk of behavior problems (Rodrigue and Houck 2001), psychological distress (Romer et al. 2002), and delinquency (Forehand, Biggar, and Kotchick 1998). For these reasons, it is important not only to understand the long-term consequences of single motherhood for health, but also to identify factors that might further improve or worsen the health of women who had a nonmarital birth. Among the range of possible factors, we focus on marriage and union formation, in part because of their implications for family policy in the United States and in light of government efforts to promote marriage among single mothers.
Nonmarital Childbearing, Union History, and Women’s Health
Decades of evidence have established that married individuals have better health and lower rates of mortality than do their unmarried counterparts (Waite and Gallagher 2000). Despite debate over the causal nature of this association and the potential role of selection, there is general consensus that marriage provides many potentially salubrious benefits, including financial resources and access to social security, public pensions, and spousal health insurance (Oppenheimer 2000). Marriage can also function as an institution of social control, encouraging healthy behaviors and providing social integration and emotional support, which are strongly linked to health (Umberson and Montez 2010). Cohabitation appears to offer some but not all of the advantages of marriage; empirical evidence suggests cohabitors have better health than unpartnered individuals but worse health than the married (Wu et al. 2003).
Understanding marriage’s impact on single mothers’ health has substantial relevance for family policy in the United States. The 1996 welfare reform bill, reauthorized in 2006, expanded the role of federal and state governments in promoting marriage, particularly among low-income single mothers. Federal funding has since been used to support hundreds of marriage promotion efforts, including public advertising campaigns that emphasize the importance of marriage and programs that provide relationship skills training. The average benefits of marriage in the general population are commonly referenced in support of government efforts to promote marriage among single mothers (Nock 2005), but it is a tall order to expect that marriage can counteract the cumulative strains of nonmarital childbearing and their eventual negative impact on health later in the life course. Social research can play an important role in guiding social policy across myriad domains, but it is critical that the empirical evidence relate specifically to the subpopulations most directly affected by such initiatives. In this case, the paucity of research on never-married mothers means we do not know whether marriage protects their health or if it might, in some cases, pose health risks. Even if women who had a nonmarital birth do not receive the same health benefits from marriage as do other women, a more fundamental question is whether marriage enhances their health at all compared to remaining unpartnered. Focusing on women who had a nonmarital birth, our second central aim is to compare the midlife health of women who subsequently marry or cohabit with women who remain continually unpartnered.
There are several reasons to expect that the benefits of marriage may not accrue to women who had a nonmarital birth. First, these women experience more conflict and receive less companionship in marriage than do women who enter marriage without children (Timmer and Orbuch 2001), and they are more likely than other married women to anticipate potential divorce (Williams, Sassler, and Nicholson 2008). Strained marriages undermine health and well-being—in some cases, more so than remaining unmarried or divorcing (Hawkins and Booth 2005; Williams 2003). Women with nonmarital births are also less likely to receive economic benefits from marriage, despite being in greater need of them. Compared with childless women, single mothers tend to marry men with lower levels of income and education (Lichter, Graefe, and Brown 2003). These women may also have children from several fathers, increasing the risk of union dissolution (Carlson and Furstenberg 2006; Lichter and Qian 2008) and concomitant financial strains. For these reasons, we distinguish single mothers who subsequently marry and then divorce from those who remain married until age 40.
Despite the high prevalence of cohabitation among single mothers (Lichter and Qian 2008), evidence of its effects on their health and well-being is lacking. We hypothesize that women who had a nonmarital birth will have a lower than average likelihood of sharing any health benefits of cohabitation, because they are more likely than childless women to form cohabiting unions with men who already have children (Goldscheider and Sassler 2006). Growing evidence indicates that cohabiting father figures earn substantially less than do married biological fathers (Hofferth and Anderson 2003; Lichter and Qian 2008). Given the additional challenges of integrating new father figures and step- or half-siblings into children’s lives (Cherlin 1978), cohabiting unions may offer few positive, and perhaps some negative, consequences for the health and well-being of single mothers. Exiting cohabiting unions is also associated with increased psychological distress, and single mothers are more likely to end their cohabiting relationships than are other women (Williams et al. 2008).
Nonmarital Childbearing, Union History, and Women’s Health: Existing Evidence
Only one prior study considers how subsequent unions affect the health of women who have had a nonmarital birth compared with remaining unpartnered. Analyzing data from the National Survey of Families and Households, Williams and colleagues (2008) find that entering marriage was not associated with improved self-assessed health across the five- to eight-year study period for mothers, even when a marriage endured. Entrance into cohabiting unions was also not associated with improved health. However, due to sample limitations, this study combined divorced mothers and women who experienced nonmarital births into a single category and was unable to consider spouses’ paternity status. We address this issue in the present study by focusing on women who had a nonmarital first birth and by distinguishing such mothers not only by whether they subsequently marry or cohabit, but also by whether they do so with the biological father of their first child or with a different partner.
Our study builds upon extant research in several additional ways. First, we focus specifically on potential racial/ethnic variations in the health consequences of subsequent union experiences of single mothers. Black women are far more likely than white or Hispanic women to bear children outside of marital unions (Hummer and Hamilton 2010), and they are less likely to marry following a nonmarital birth (Graefe and Lichter 2002). Some evidence suggests that many low-income, black single mothers face considerable barriers to marriage, including a shortage of economically attractive men (Lichter and Graefe 2007) and gender distrust (Anderson 1992; Edin and Kefalas 2005; Edin and Reed 2004) that arises in part from multi-partner fertility and the threat this represents to new partners (Mincy 2002). The likely impact of these barriers on the health consequences of marriage among black single mothers is, however, difficult to predict. In one view, black single mothers who overcome challenges to wed may have particularly strong relationships and supportive partners, suggesting they may be especially likely to benefit from marriage. However, the likelihood that a healthy marriage selection effect exists among black single mothers is undermined by evidence that black mothers’ marriages are more likely than their Hispanic and white counterparts’ marriages to end in divorce (Graefe and Lichter 2002). Overall, we expect that because black single mothers, on average, face greater barriers to healthy enduring marriages than do their white and Hispanic counterparts, marriage will provide them with fewer health benefits.
Second, prior research takes a short-term view of the potential benefits and costs of subsequent marriage for single mothers’ health, typically investigating outcomes within five years of union entry. Placing this question within a life course framework draws attention to the importance of considering more enduring consequences of single mothers’ union histories. Spurred in part by the growing availability of longitudinal data, recent studies across a range of disciplines demonstrate that negative social conditions experienced early in life can be associated with a diverse array of poor health outcomes many years later (Hayward and Gorman 2004; Kuh and Ben-Shlomo 1997; Palloni 2007). Similarly, integration of a life course perspective with the study of social stress has produced mounting evidence that transitions and strains experienced at one life course stage have cumulative effects on health that can result in the emergence of chronic illness decades later (Pearlin et al. 2005). This lag occurs, in part, because many chronic illnesses have long latency periods (Lynch and Smith 2005) and because stressful life events produce chronic secondary strains that, by definition, accumulate over time (Pearlin et al. 2005).
A short-term perspective in which health outcomes are measured contemporaneously with influential life course transitions may therefore grossly underestimate true long-term associations between the two. Furthermore, from policy and public health perspectives, it is especially important to identify events and conditions with enduring consequences for health, compared to those with short-lived effects. We focus on estimating the association of single mothers’ subsequent union transitions with their health in midlife, a time when health problems are beginning to emerge and when chronic strains associated with union transitions (or the lack thereof) have likely accumulated over time. A third contribution of this study, which we will address in greater detail, is our use of multivariate propensity score matching to partially address selection bias.
Selection into Nonmarital Childbearing and Marriage
Studies examining the average association of marriage with health generally indicate that differential selection into marriage accounts for some but not most of the association (Waite and Gallagher 2000). However, health-based selection into nonmarital childbearing and marriage may be more prominent among women who had a nonmarital birth than in the average population because nonmarital births are most prevalent among the less advantaged, and marriage is less common among single mothers (Goldscheider and Sassler 2006; Lichter et al. 2003; Lichter and Qian 2008). Our data allow us to control for a range of background characteristics predictive of entry into nonmarital parenting and of single mothers’ subsequent union pathways. We also employ multivariate propensity score matching in two ways to partially address bias due to selection. First, we determine whether significant observed associations of nonmarital parenting with midlife health exist when women who had a nonmarital first birth are matched with women who have a similar estimated propensity of having a nonmarital first birth. Second, among women who had a nonmarital first birth, we determine whether significant observed associations of union histories with midlife health persist when women who enter unions are matched with women who have a similar predicted propensity of sharing that union history.
Data and Measures
Data
The 1979 National Longitudinal Survey of Youth (NLSY79) (Bureau of Labor Statistics, U.S. Department of Labor 2009) data are uniquely suited to investigating long-term consequences of nonmarital childbearing and subsequent family transitions. The NLSY79 is an ongoing survey of a nationally representative sample of 12,686 young men and women ages 14 to 22 years in 1979. The study originally included oversamples of black, Hispanic, military, and poor white respondents. Although the military and economically disadvantaged white oversamples were dropped prior to 1991, the remaining respondents were interviewed annually through 1994 and biennially since. By 2008, data on detailed union histories had been continuously collected over a 29-year period, and measures of health and well-being ascertained at age 40, a time when health problems begin to emerge. As of 2006, all NLSY79 mothers were over age 40.
For our first set of analyses (reported in Table 3), a total of 3,986 women had given birth prior to age 40, and 3,471 (89.3 percent) of them completed the age 40 health assessment. We further limit this sample to the 3,896 women whose first birth took place prior to age 36 and who therefore had sufficient time to enter a union prior to reaching age 40. Of this subsample, 3,391 (89.1 percent) completed the self-assessed health measure. Our second primary analyses (reported in Table 5) focus on the 1,275 women who had a nonmarital first birth prior to age 36 (this includes 246 white, 799 black, and 230 Hispanic women). Of these 1,275 women, 1,150 (90.2 percent) completed the age 40 health module. The amount of data missing is greatest for the measure of self-reported health (reported earlier), followed by maternal years of education (6.2 percent), poverty status (6.0 percent), AFQT score (5.0 percent), and health limitations (3.1 percent). To maintain maximum sample size, we estimated all regression models using multiple imputed data created from the imputation chained equations (ICE) program for Stata (Royston 2006). 1 Propensity score matching was implemented using the psmatch2 program created for Stata by Leuven and Sianesi (2003). We calculated bootstrapped standard errors for all matching estimations.
Measures
Self-assessed health
We measure self-assessed health at age 40 with a single question: In general, would you say your health is excellent, very good, good, fair, or poor? We coded responses from 1 to 5 with higher values indicating better health. Self-assessed health is highly predictive of subsequent morbidity and mortality (Idler and Benjamini 1997) and is widely recognized as a valid and reliable indicator of health status in the general population (Ferraro and Farmer 1999).
Single motherhood status
We define a single mother as a woman who had a first birth while never-married and lived with that child in her household.
Marital and cohabitation history
Six dummy variables distinguish the following marital and cohabitation histories by age 40 for women who had a nonmarital first birth at age 35 or younger: (1) entered a single enduring marriage with the first child’s biological father (n = 203), (2) entered a single enduring marriage with a new partner (n = 168), (3) entered and exited a marriage with the first child’s biological father (n = 129), (4) entered and exited a marriage with a new partner (n = 123), (5) never married but cohabited with the biological father (n = 104), and (6) never married but cohabited with a new partner (n = 43). The reference category consists of continually never-married and unpartnered women (n = 187).
Control variables
Control variables include race/ethnicity (non-Hispanic black, Hispanic and non-Hispanic non-black [i.e., white]), U.S. nativity (1 = foreign born), age at first birth, cohabitation status at first birth (1 = cohabiting), cognitive ability (1980 AFQT score, which ranges from 1 to 99), poverty status at baseline (1 = in poverty, based on whether family income was below the federal poverty income guidelines for the particular family size in 1978), mother’s family composition at age 14 (1 = lived with both biological parents), her own mother’s years of education as a proxy for socioeconomic status of her family of origin, and the existence of health conditions in 1979 that limit a respondent’s ability to work for pay (1 = yes). Because nonmarital childbearing and health differ for Hispanics depending on their nativity status, we also control for the interaction of Hispanic X U.S. nativity.
Although the number of biological children a woman has by age 40 and her marital status at age 40 likely influence health, they are consequences rather than causes of nonmarital fertility and subsequent union history. Controlling for these potential mechanisms would underestimate the true total effect of single motherhood or subsequent union history on midlife health; we therefore exclude them from the models presented. Supplementary analyses, however, reveal that their inclusion does not change the overall pattern of findings, suggesting their role as potential mediators is negligible.
Analysis
Our analyses address two basic questions: (1) Does nonmarital parenthood undermine health and well-being? (2) Among women who had a nonmarital first birth, is subsequent marriage or cohabitation associated with better health at midlife than remaining never married? We first employ ordinary least squares (OLS) and ordered probit regression to address these questions. 2
Selection into nonmarital childbearing and subsequently forming unions is a nonrandom process. To identify the effect of nonmarital childbearing and later union transitions on mothers’ health, we must minimize the potential bias due to nonrandom selection. We do this by conditioning on pre-treatment observable characteristics (Rosenbaum and Rubin 1983) derived from the literature on nonmarital childbearing and union formation following nonmarital births. Propensity score matching (PSM) then allows us to match women in our sample based on the predicted probability they had a nonmarital birth or experienced a particular union history (i.e., the propensity score) as a non-parametric feature of these pre-treatment (or predetermined) observed characteristics (Dehejia and Wahba 2002). PSM models thus estimate the average effect of having a nonmarital birth (or, in later models, union history) among women similarly likely to engage in such behaviors. In the second stage of each part of our analysis, we determine whether significant associations identified in the first-stage OLS models are robust to a propensity score matching specification. As Morgan and Harding (2006) argue, the use of matching techniques provides a sizable advance over merely conceding that selection bias may be present in some form and speculating on the sign of the bias.
We use one-to-one nearest neighbor matching with replacement (Morgan and Harding 2006; Rosenbaum and Rubin 1983). Nearest neighbor matching (with and without replacement) and other approaches (e.g., interval matching and kernel matching) are closely related. To date, there are no standardized guidelines for choosing a matching procedure (Gangl 2010; Morgan and Winship 2007), although research shows that nearest neighbor matching estimates produce lower standard errors, compared with caliper matching, and are preferred when there is a large overlap in propensity scores between treatment and control groups (Black and Smith 2004; Dehejia and Wahba 2002). We use matched observations from the treatment and control groups to compute differences in health at age 40; we then compute the average difference across all matches. Where necessary, we trim the sample to ensure common support (i.e., the range of propensity scores is the same for treatment and control groups). We use bootstrapped standard errors (n = 50) to ensure the most robust outcomes for our PSM results.
Descriptives
Table 1 shows descriptive statistics (means and standard deviations or percentages) for all variables by race/ethnicity and marital status at first birth. We assess bivariate differences between women with a nonmarital first birth and women with a marital first birth within race/ethnicity with independent sample t-tests or chi-square tests. Consistent with our hypothesis, women who had a nonmarital first birth have lower levels of self-assessed health at age 40 than do their same race/ ethnicity counterparts who had a marital first birth. Several background differences are also evident, some of which vary by race/ethnicity. Women with a nonmarital first birth were younger than married mothers at their first birth, their mothers had lower levels of education, they were less likely to have lived with both parents at age 14, they were much more likely to be living in poverty at baseline, and they had lower cognitive ability scores. White women with a nonmarital first birth were more likely to report a health limitation at baseline than were their counterparts with a marital first birth. Among black women, those with a nonmarital first birth were less likely to be foreign born than were those with a marital first birth.
Descriptive Statistics by Marital Status at First Birth and Race/Ethnicity among Women Whose First Birth Occurred Prior to Age 36 (imputed data)
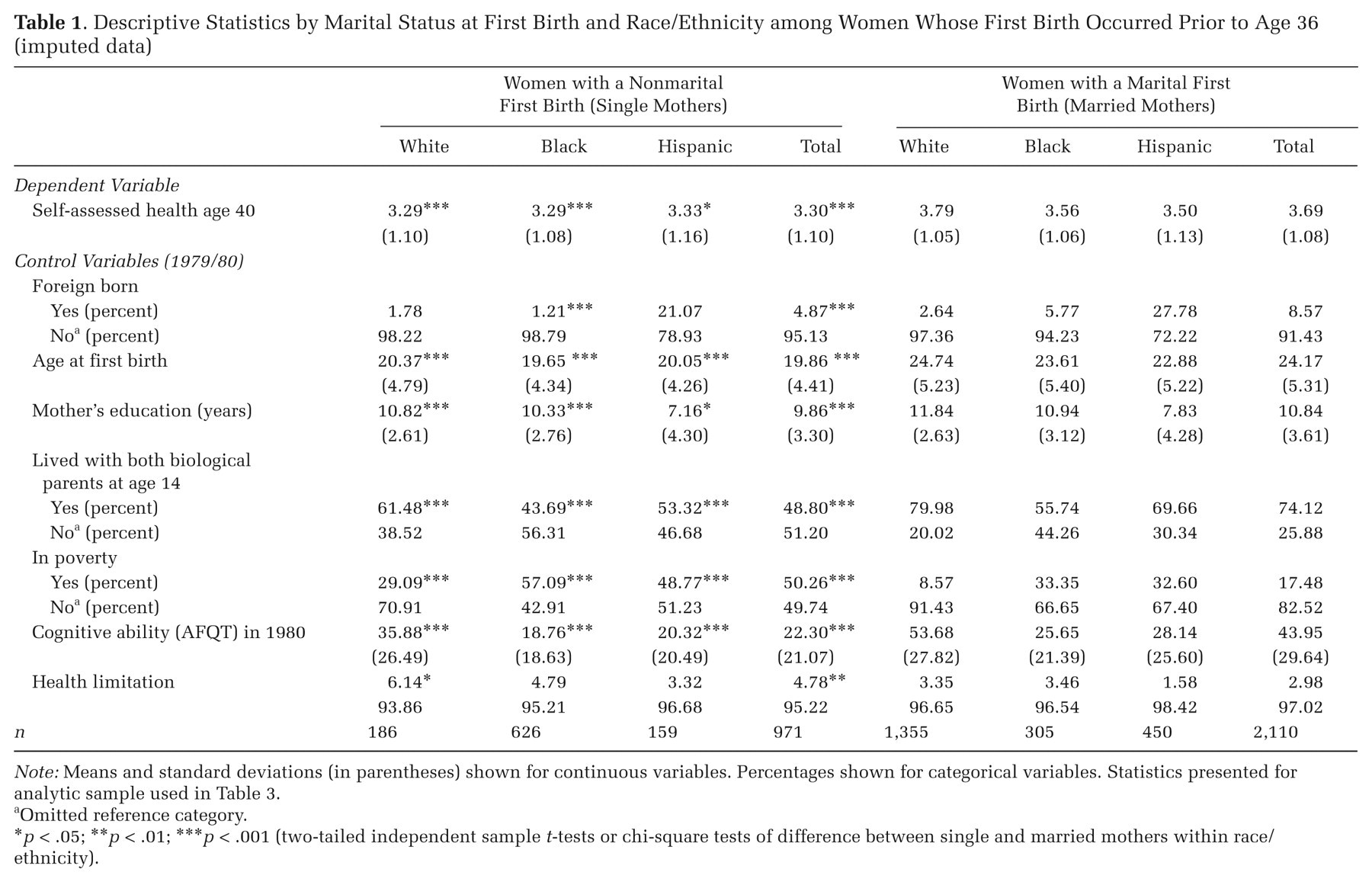
Note: Means and standard deviations (in parentheses) shown for continuous variables. Percentages shown for categorical variables. Statistics presented for analytic sample used in Table 3.
Omitted reference category.
p < .05; **p < .01; *** p < .001 (two-tailed independent sample t-tests or chi-square tests of difference between single and married mothers within race/ethnicity).
Table 2 shows the distribution of women who had a nonmarital first birth prior to age 36 according to their subsequent union history and their cohabitation status at birth by race/ethnicity. Among women with a nonmarital first birth, black women are the most likely to be in the “never married, never cohabited” group, followed by Hispanic and then white mothers. Hispanics are more likely than whites and blacks to cohabit with the child’s biological father without marrying, and Hispanics and whites are more likely than blacks to enter an enduring marriage with the biological father. White single mothers are more likely than their black and Hispanic counterparts to marry and subsequently divorce the biological father and are more likely than black mothers to marry and divorce a new partner. Overall, black women’s relatively low probability of marriage and high probability of remaining unpartnered substantially distinguishes them from Hispanic and white women.
Distribution of Post-birth Union Histories and Cohabitation Status at Birth by Race/Ethnicity and Poverty Status among Women with a Nonmarital First Birth at Age 35 or Younger (imputed data)
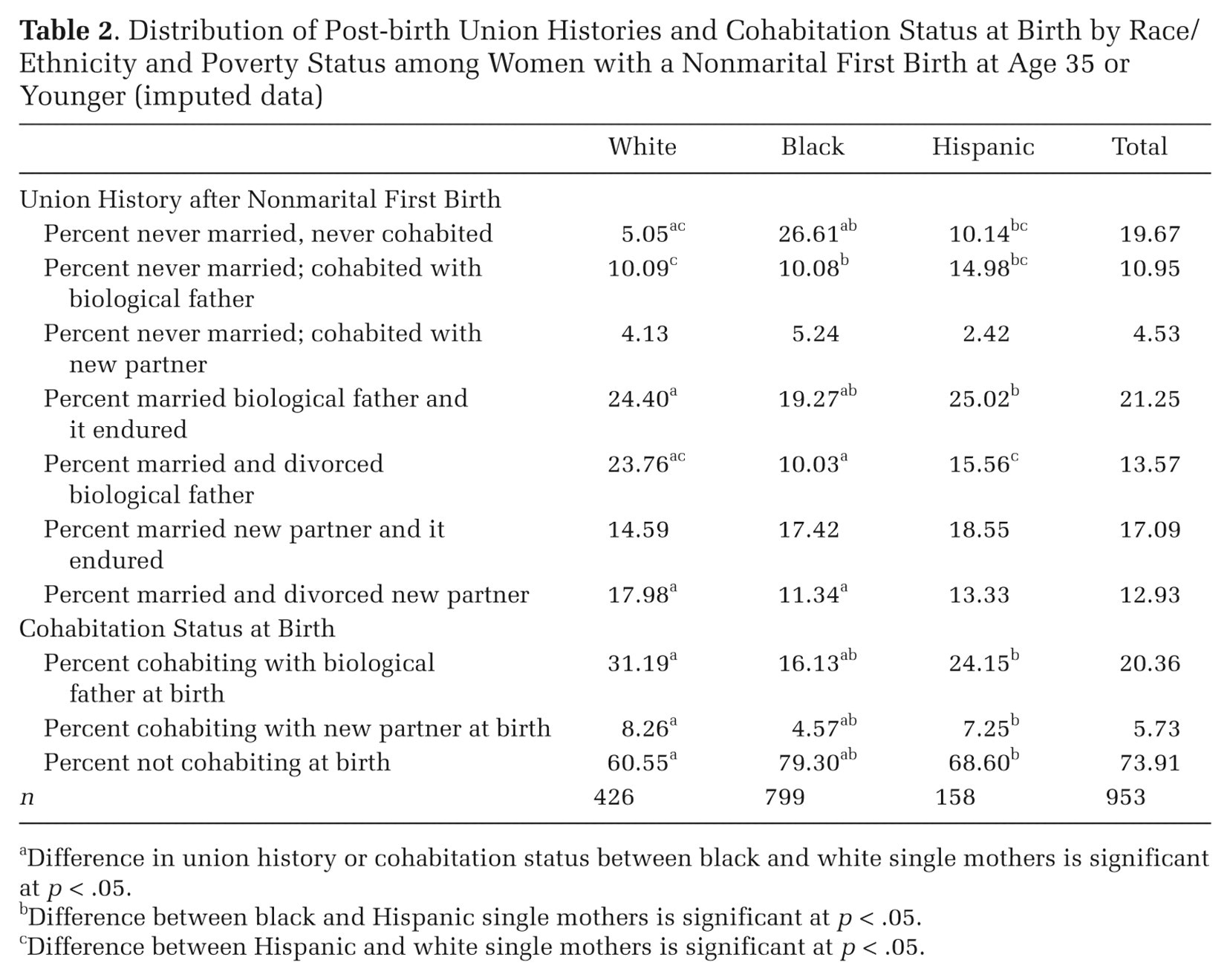
Difference in union history or cohabitation status between black and white single mothers is significant at p < .05.
Difference between black and Hispanic single mothers is significant at p < .05.
Difference between Hispanic and white single mothers is significant at p < .05.
We also examined bivariate associations of union history with age 40 self-assessed health by race/ethnicity for the same sample of women as in Table 2. Results are available in Table S1 of the online supplement (http://asr.sagepub.com/supplemental). At the bivariate level, neither marriage nor cohabitation is positively associated with the health of white and Hispanic women who had a nonmarital birth. However, black single mothers who subsequently enter an enduring marriage with the child’s biological father have better midlife self-assessed health than do black women who remain unpartnered.
Results
Midlife Health of Women with a Nonmarital First Birth
Table 3 presents results from OLS regression models comparing health at age 40 of women who had a nonmarital first birth to that of their counterparts who had a marital first birth prior to age 36. As Model 1 shows, even when controlling for a range of background characteristics (including highly significant predictors such as AFQT score, mother’s education level, and health limitations at baseline), women who had a nonmarital first birth report lower levels of self-assessed health at age 40 than do women who had a marital first birth.
OLS Regression Coefficients Estimating the Effect of a Nonmarital First Birth on Age 40 Self-Assessed Health: Women Who Had a First Birth at Age 35 or Younger (imputed data)
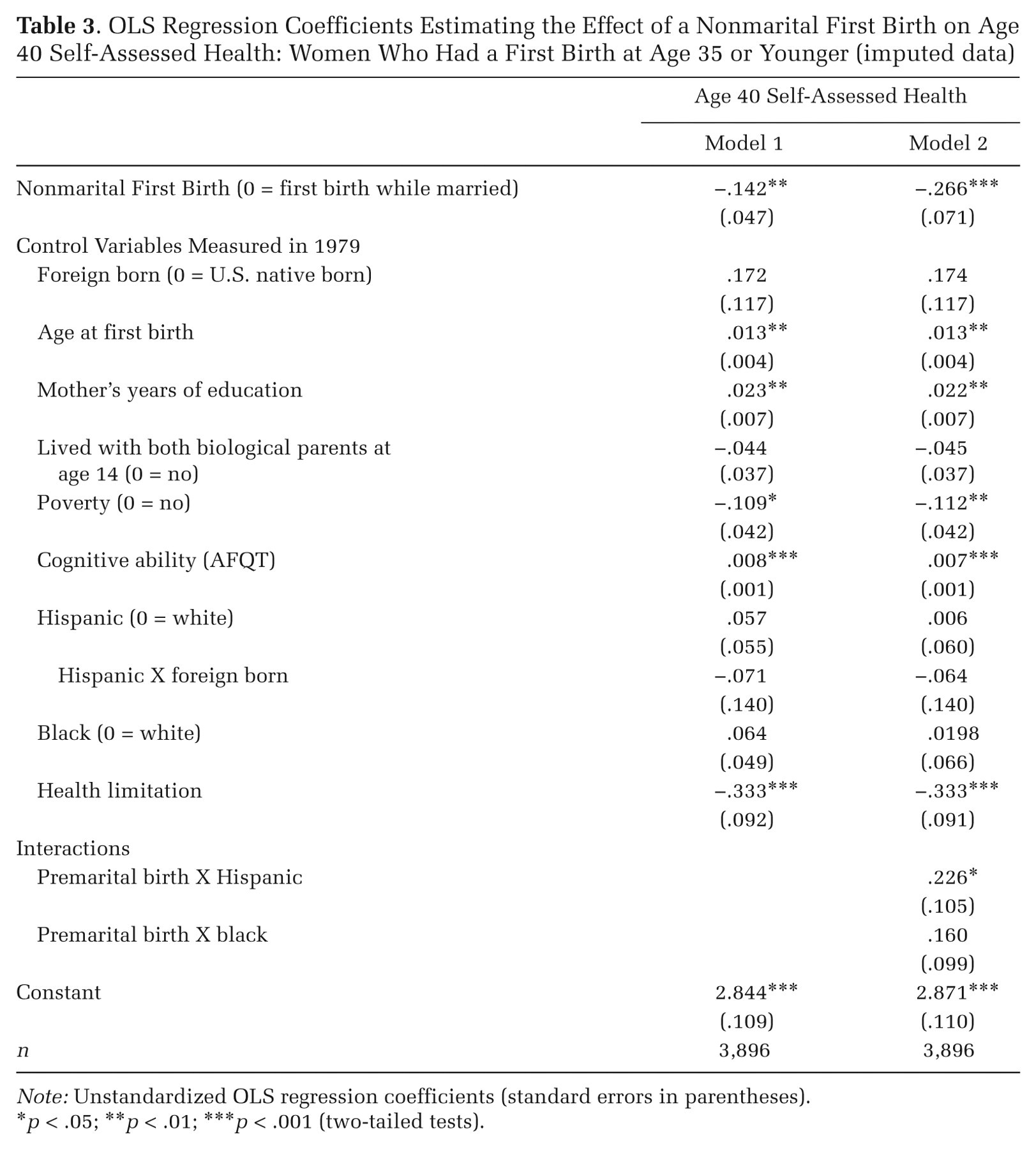
Note: Unstandardized OLS regression coefficients (standard errors in parentheses).
p < .05; **p < .01; *** p < .001 (two-tailed tests).
In Model 2, we enter interaction terms to test for racial/ethnic differences in the estimated effect of nonmarital childbearing on midlife health. The health disadvantage associated with having a nonmarital birth does not differ for white and black women, but it is smaller for Hispanic women. Supplementary analysis indicates that the estimated effect of nonmarital parenthood on midlife health is negative for white and black women but not distinguishable from zero for Hispanic women. Nonmarital parenting appears to have few long-term negative consequences for Hispanic women’s health, as their midlife health is similar to that of their counterparts who had a marital first birth (.226 − .266 = −.04).
We next employ multivariate propensity score matching to determine whether the significant associations presented in Table 3 are robust to an approach that better accounts for the differential selection of women into premarital parenthood. This analysis estimates the likelihood of experiencing a nonmarital first birth for the total sample of women who became mothers. We do this by conditioning on characteristics observable prior to conception that are associated with entrance into nonmarital childbearing (Rosenbaum and Rubin 1983). 3 Covariates used to estimate the propensity for nonmarital birth include mother’s family structure at age 14, health limitations and cognitive abilities, poverty status at baseline, self-efficacy, gender role orientations, and expectations for future education, family, and fertility as ascertained in 1979. These measures are described in detail in Table S2 in the online supplement and marked with the symbol †. Significant predictors of nonmarital first births for the total sample include baseline measures of mothers’ AFQT scores, health limitations, family structure at age 14, nativity, race, poverty status, and educational expectations.
Table 4 presents coefficients obtained from the OLS models and the average treatment effects for the treated, estimated from the PSM models. Results in the first panel (total sample) reveal little difference in the estimated effect of nonmarital first births on self-reported health at age 40 across the two sets of analyses; both coefficients are statistically significant. Because our OLS analysis indicates that having a nonmarital birth is associated with poorer health for white and black women, but not for Hispanic women, we estimate a separate propensity score matching model limited to black and white women (second panel of Table 4). As expected, the average treatment effect for the treated (ATT) is significant and greater for the black and white subsample than for the total sample, which includes Hispanic women. In summary, the PSM increases confidence in our OLS results by showing that among black and white women with similar propensities to have nonmarital first births, women who actually have one report substantially worse midlife health than do women whose first birth occurred in marriage. We find no evidence of negative health consequences of nonmarital childbearing for Hispanic women.
Comparison of OLS and Propensity Score Matching Results Estimating the Effect of a Nonmarital Birth on Age 40 Self-Assessed Health (imputed data)
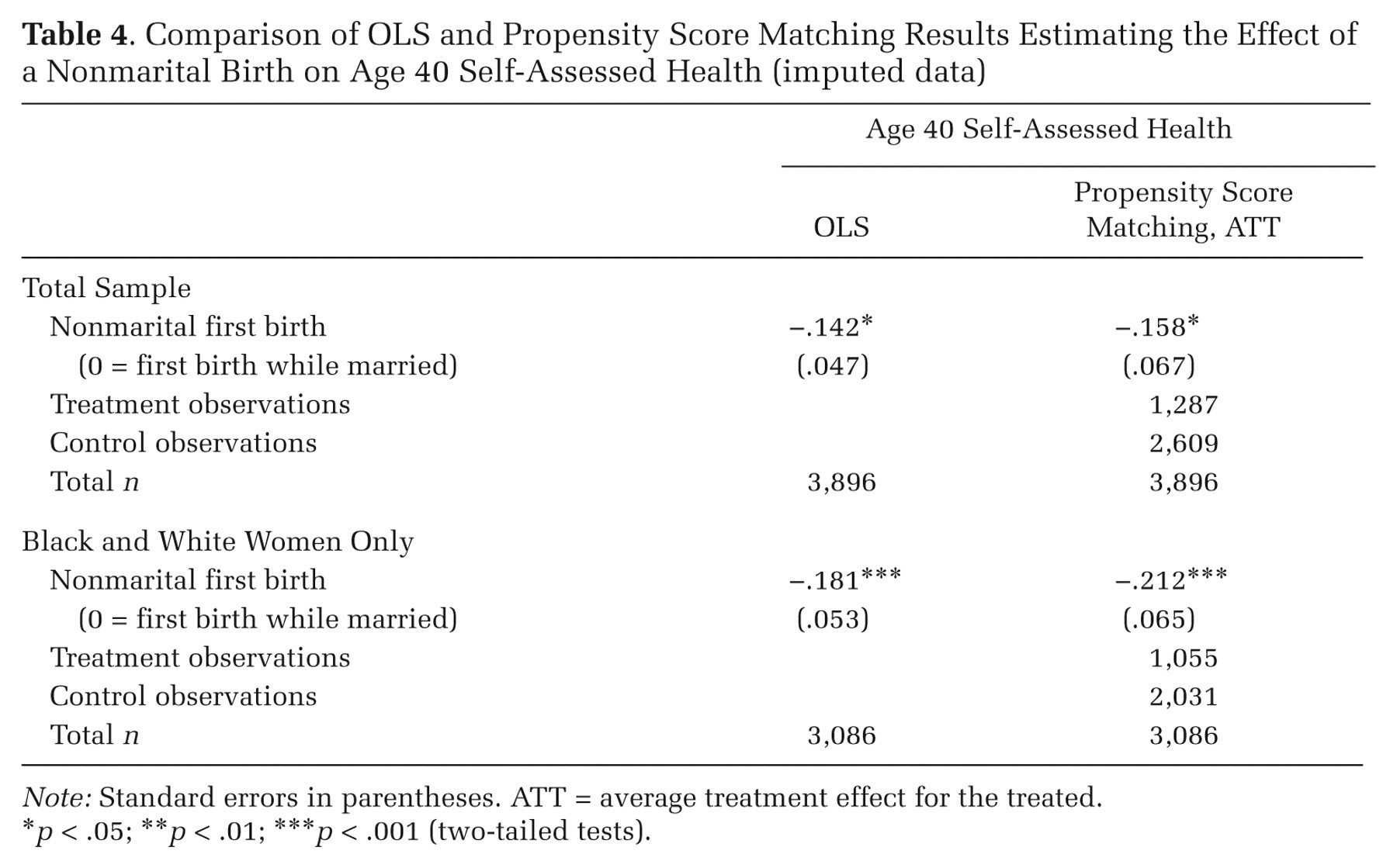
Note: Standard errors in parentheses. ATT = average treatment effect for the treated.
p < .05; **p < .01; *** p < .001 (two-tailed tests).
Nonmarital Childbearing, Subsequent Union History, and Health at Midlife
In the second part of the analysis, we limit the sample to women who had a nonmarital first birth before age 36. We use OLS regression to examine whether women who later marry or cohabit have better midlife health than women who remain unpartnered through age 40, giving attention to their partners’ paternity status and the stability of the union (supplementary ordered probit analyses are available from the authors upon request). Table 5 shows results for the total sample (all racial/ethnic groups combined) and the black subsample. Sample sizes do not allow us to estimate separate models for white and Hispanic women.
OLS Regression Coefficients Estimating the Association of Union History with Age 40 Self-Assessed Health: Women Who Had a Nonmarital Birth at Age 35 or Younger (imputed data)
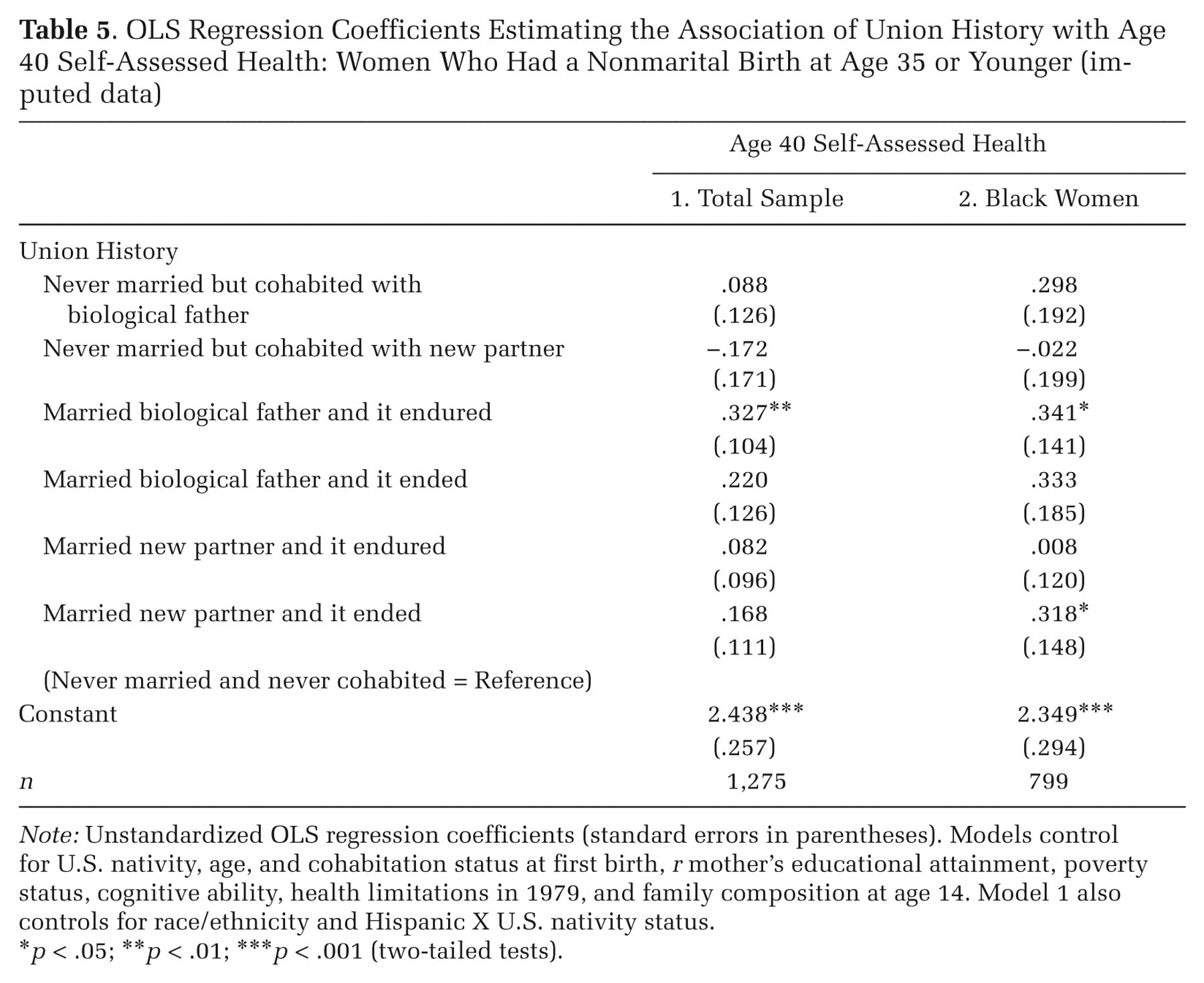
Note: Unstandardized OLS regression coefficients (standard errors in parentheses). Models control for U.S. nativity, age, and cohabitation status at first birth, r mother’s educational attainment, poverty status, cognitive ability, health limitations in 1979, and family composition at age 14. Model 1 also controls for race/ethnicity and Hispanic X U.S. nativity status.
p < .05; **p < .01; *** p < .001 (two-tailed tests).
With a few notable exceptions, results suggest that most subsequent union experiences neither offer health benefits nor pose health risks in midlife to women who had a nonmarital birth. In some cases, however, marriage to the first child’s biological father appears to benefit women’s health. For the total sample and the black subsample, single mothers who subsequently marry their first child’s biological father report better midlife health than do women who remain unpartnered, but this difference reaches significance only for women whose marriage to the biological father endures. In addition, black single mothers who subsequently marry and then divorce a new partner report better midlife health than do their continually unpartnered counterparts. For single mothers with all other union experiences, their midlife health does not significantly differ from that of women who remain unpartnered.
We also considered that cohabitation might offer differential benefits to health compared with some types of marital unions. In supplementary analyses (available from the authors upon request), we varied the reference category to compare mothers who subsequently cohabited without marrying to mothers who entered each type of marital union. Results suggest that marrying a new partner offers no greater health benefits than does cohabiting with either the child’s biological father or with a new partner. Marriage to the biological father (whether it endures or not) is not significantly associated with better health than is cohabiting with him. However, single mothers who subsequently enter an enduring marriage with the child’s biological father have better midlife health than do mothers who cohabit with a new partner. For the black subsample, there are no significant differences in health for single mothers who subsequently cohabit versus those who enter a marital union, either with the child’s biological father or with a new partner.
Finally, because marriage promotion policies commonly target low-income single mothers, we estimated supplementary models that include an interaction term for baseline poverty status X union history. We find no significant differences by poverty status in the estimated effect of subsequent union history on the health of women who had a nonmarital birth, either in the total sample or the black subsample.
We next use PSM to determine whether the significant associations of union history with single mothers’ midlife health, shown in Table 5, are robust to a consideration of differential selection into marriage with a child’s biological father among women with a nonmarital birth. We first estimate the likelihood of marriage to the child’s biological father (relative to remaining never married and not cohabiting). We refine the measure to include only marriages that endure up to age 40 for the total sample of mothers whose first birth was nonmarital. We also undertake a separate analysis of black women who had a nonmarital first birth, examining marriages to the child’s biological father that endured and marriages to other men that dissolved. The covariates used to predict entrance into marital unions are marked with Ω in Table S2 in the online supplement. For the total sample, significant predictors of entering an enduring marriage with the child’s biological father are a respondent’s AFQT score, mother’s age at the child’s birth, whether a mother was foreign born, and if she was cohabiting (with the biological father or another man) at the time of the child’s birth. For the analysis limited to black women with a nonmarital first birth, the variables significantly associated with an enduring marriage to the child’s biological father include woman’s age at the child’s birth and whether she was cohabiting at the time the child was born; only age at first birth is significantly associated with the likelihood of subsequently entering a marriage with a new partner that results in divorce.
Table 6 presents comparisons of the coefficients obtained from OLS models shown in Table 5 and the average treatment effects from the PSM models. In the total sample, the PSM model predicts that age 40 self-assessed health of single mothers who later enter an enduring marriage with the child’s biological father is significantly better than what it would have been if these women had remained unmarried and unpartnered. This underscores our OLS results. However, when we limit the analysis to black women, we find that the better health of mothers who remain wedded to a child’s biological father compared with mothers who remain unpartnered is no longer statistically significant. Similarly, whereas the coefficient for black women who marry a new partner and experience the dissolution of that marriage is significant in the OLS model, it no longer reaches conventional levels of significance in the PSM analysis. In summary, the PSM results indicate health benefits of subsequently entering an enduring marriage with a child’s biological father for white and Hispanic mothers but not for black single mothers.
Comparison of OLS and Propensity Score Matching Results Estimating the Effect of Union Transitions with Age 40 Self-Assessed Health among Women Who Had a Nonmarital First Birth (imputed data)
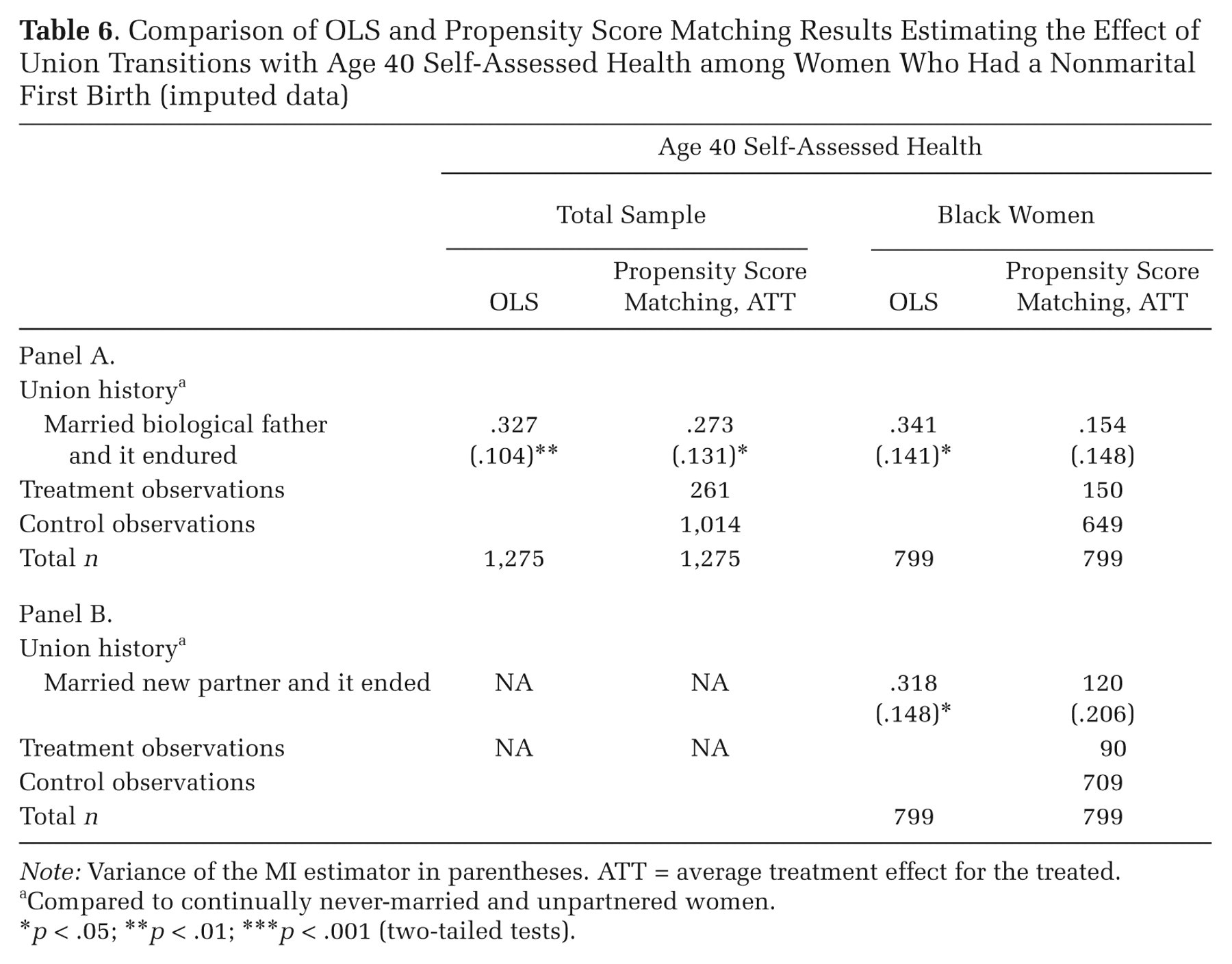
Note: Variance of the MI estimator in parentheses. ATT = average treatment effect for the treated.
Compared to continually never-married and unpartnered women.
p < .05; **p < .01; *** p < .001 (two-tailed tests).
Discussion
The growing prevalence of nonmarital childbearing coupled with the aging of the population draw attention to the importance of understanding the midlife health of women who have had a nonmarital birth, and of identifying the role of subsequent marriage in shaping these health outcomes. We used panel data from the 1979 to 2006 NLSY79 to assess differences in midlife self-assessed health between women who had a nonmarital first birth and women whose first birth occurred in marriage. We tracked the subsequent union histories of women who had a nonmarital first birth to estimate the effect of marrying or cohabiting versus remaining never-married on self-assessed health, giving particular attention to the paternity status of a mother’s partner as well as the stability of a marriage.
Our empirical results lead to two central conclusions. First, on average, having a nonmarital first birth in the United States is negatively associated with white and black women’s health at midlife, and this is not due solely to negative selection into nonmarital childbearing. Substantial evidence shows that single mothers experience high levels of stress, psychological distress, and social isolation (Avison et al. 2007; Barrett and Turner 2005; Cairney et al. 2003; Hope et al. 1999; Wang 2004). However, ours is the first U.S. study to document long-term negative health consequences of nonmarital childbearing among a recent cohort of women who are just entering midlife and for whom the cumulative strains of single motherhood should be most evident. These findings underscore the importance of the life course perspective in highlighting potential cumulative effects, and hence enduring consequences, of occurrences earlier in life that may have ramifications in later years.
Although we find that nonmarital births equally undermine the health of black and white women, single motherhood appears to have no negative long-term consequences for the health of Hispanic women. This may reflect the fact that, compared with other racial/ethnic groups, Hispanic women’s nonmarital births are more likely to occur in long-term cohabiting unions that resemble marriage (Oropesa and Landale 2004; Wildsmith and Raley 2006). Hispanic single mothers may also be embedded in larger and more close-knit family networks, which can provide emotional and instrumental support resources that are protective of health and facilitate coping with the strains of single parenthood (Osborne, Manning, and Smock 2007). Relevant to our findings for Hispanics is Geronimus’s (2003) warning that dominant cultural scripts that stigmatize early or nonmarital births among minority groups ignore the cultural, structural, and ecological contexts that sometimes make alternative fertility patterns adaptive or at least benign.
Second, for most women, negative long-term health consequences of having a nonmarital first birth are unlikely to be mitigated by subsequently entering a cohabiting or marital union. Across all racial/ethnic groups, single mothers who marry or cohabit with a new partner, cohabit with the child’s biological father, or marry and divorce the biological father report no better health at age 40 than do women who remain unpartnered. These results are consistent with research showing few short-term health benefits of marriage or cohabitation for women who enter unions with children (Williams et al. 2008) or after having a nonmarital birth (Meadows, McLanahan, and Brooks-Gunn 2008). We extend this literature by examining longer term consequences and by distinguishing women by the nature of their husbands’ relationship to their children, and whether these unions endure.
In the full sample, we do find evidence of health benefits for women who enter and remain in a marriage with their child’s biological father. These benefits weaken but remain significant after adjusting for differential selection into such a marriage. Our findings are consistent with Williams and colleagues’ (2008) observation that the short-term mental health benefits of marriage for single mothers are limited to women whose marriages endure. The present study clarifies this pattern by showing that any long-term physical health benefits of subsequent union formation are limited to enduring marriages with the first child’s biological father and, as we discuss below, are further limited by race/ethnicity. Blended and step-families face a unique set of stressors related to family boundary ambiguity (in which family members do not perceive a step-parent to be a full member of the family) (Brown and Manning 2009) and a lack of cultural norms and supports to guide interaction (Cherlin 1978). Moreover, fathers are less involved in parenting nonbiological than biological children (Hofferth and Anderson 2003). Given gendered roles in interpersonal relationships, mothers who marry a new partner likely assume much of the responsibility for forging interpersonal bonds and resolving conflicts between members of the blended family (Nielson 1999). Stress associated with this process may undermine any health benefits that marriage would otherwise offer to such women.
For black single mothers, once differential selection is taken into account, even an enduring union with a child’s biological father appears to offer no health benefits. This is consistent with our hypothesis that the challenges faced by black single mothers in forming healthy lasting relationships may lead them to receive few health benefits from marriage. The constrained marriage markets of black single mothers likely play an important role (Harknett and McLanahan 2004; Wilson 1987). Black single mothers are more likely to marry men who are also unwed fathers (Lichter and Graefe 2007), have few economic resources (Graefe and Lichter 2008), lack a high school diploma (Lichter et al. 2003), or who have been incarcerated or have substance abuse problems (Lopoo and Carlson 2008). In summary, marriage market constraints that stem largely from inequality and economic disadvantage likely result in black single mothers receiving fewer of the resources—economic resources and emotional support—through which marriage’s health advantages are conferred (Waite and Gallagher 2000).
Our observation that even marriage to the child’s biological father offers no health benefits for black women is important for several reasons. Black women have far higher rates of nonmarital fertility than do white women (72/1,000 versus 32/1,000, respectively) (Ventura 2009) and black single mothers are more likely to be economically disadvantaged. Black single mothers are, therefore, disproportionately affected by government marriage promotion programs for low-income populations. To the extent that our results can be generalized to more recent cohorts of single mothers, a point to which we turn next, they suggest that even when marriage promotion strategies lead to enduring unions, these programs are unlikely to have any success in protecting the health of the targeted population.
Our analyses have several limitations. First, the relatively small numbers of white and Hispanic women who had a nonmarital birth prevent us from identifying the possibly distinct health consequences of union history for women in these two groups. We do not know if our observation that marriage to a child’s biological father is associated with better health is limited to white or Hispanic women. Because our first set of analyses indicates no negative consequences of nonmarital childbearing for Hispanic women’s health, long-term health benefits of subsequent marriage to a child’s biological father may in fact be limited to white women. A related issue is our inability, due to small sample sizes, to disaggregate our analyses by time since a union transition. Unions (especially marriages) that occur shortly after a nonmarital birth may be more effective than later unions in improving health. Unfortunately, more direct empirical investigation of these questions requires data that, to our knowledge, are not currently available.
Second, despite our observation that marriage to the child’s biological father, compared with remaining unpartnered, is associated with better midlife health for the combined group of white and Hispanic women, we cannot conclude that this is a causal relationship. Our propensity score models enable us to limit our comparisons to women who have a similar propensity to enter such a union based on observable characteristics, and the NLSY79 data allow us to employ a wider range of background characteristics than are typically used. Nevertheless, it is possible that unobserved characteristics associated with health differentially select white and Hispanic single mothers into marriage with their children’s biological father. A lack of comparable measures of baseline and midlife health prohibit using fixed-effects models; we hope future data collection efforts will enable this.
Third, we urge caution in generalizing these results to more recent cohorts of women for whom nonmarital childbearing is more common. It is possible that long-term negative health consequences of nonmarital childbearing will wane among cohorts for whom the experience has become more normative. On the other hand, if the normative status of nonmarital childbearing mitigates its negative health consequences, black women’s health should be less strongly affected than white women’s and we find no evidence of this. Moreover, the 1996 welfare reform legislation sharply curtailed the social safety net available to low-income single mothers and could result in more negative outcomes in future years.
A related consideration is the large shift in the age distribution of nonmarital fertility in the past 30 years (Hamilton et al. 2009). Due to this shift, our sample contains a greater proportion of teenage single mothers than exist in more recent cohorts. Recent research that disentangles the extent to which adverse outcomes of teen motherhood are attributable to the teen birth, itself, versus many teen mothers’ disadvantaged backgrounds suggests that consequences of adolescent childbearing are not always as negative as have been portrayed in the media or by politicians (Furstenberg 2007). However, teen mothers do have lower high school graduation rates and postsecondary educational achievements than their older counterparts (Hoffman 2008). This shift in the age distribution may result in fewer negative health consequences of single motherhood in future years.
In spite of these caveats, our study may have relevance for the debate about the consequences of government efforts to promote marriage among low-income single mothers. On the positive side, our results suggest no long-term negative effects of marriage on the health of women who have a nonmarital first birth, even among women whose marriages subsequently dissolve. Taken together with prior research, marriage promotion efforts are unlikely to have immediate or long-term negative effects for single mothers’ self-assessed health.
Nevertheless, our results also suggest that nonmarital childbearing itself undermines midlife health for black and white (although not Hispanic) women, and even enduring marriages are unlikely to mitigate this outcome for black women. Although we find no evidence in ancillary analyses (available from the authors upon request) that the health benefits of subsequent marriage to a child’s biological father differ depending on single mothers’ poverty status at baseline, it is clear that black single mothers are more likely than their white counterparts to be economically disadvantaged and, hence, they are disproportionately targeted by marriage promotion efforts. In other words, the group most likely to be affected by marriage promotion efforts—black single mothers—is least likely to benefit from them, at least in terms of self-assessed health at midlife. More generally, our findings imply a cautionary tale about succumbing to a tyranny of averages and highlight the importance of ensuring, to the extent possible, that policy is informed by research on the targeted subpopulations. In this case, the empirical evidence does not support axiomatic assumptions about the universal benefits of marriage.
Our approach and findings also underscore the importance of using a life course perspective to understand the long-term consequences of stressful life events and conditions on health and well-being decades later (Pearlin et al. 2005). As the U.S. population ages, a growing number of women will enter midlife and older age—a time when health problems begin to emerge—having experienced the cumulative strains associated with single motherhood. Marriage promotion efforts, even efforts that focus on creating healthy lasting unions, are unlikely sufficient to address this growing public health problem for black women. For other women, these efforts may be effective only to the extent that they result in healthy, lasting unions to the child’s biological father. More research is needed on the mechanisms through which single motherhood undermines the health of U.S. women and on the way these processes unfold over the life course and, possibly, across generations. Chronic financial strain likely plays an important role. Some evidence suggests that marriage only minimally alleviates the poverty and economic strain that accompany nonmarital childbearing (Sigle-Rushton and McLanahan 2002); this may partly explain why marriage appears to offer few benefits to single mothers’ long-term health.
Footnotes
Acknowledgements
We gratefully acknowledge the generous support and encouragement of the Initiative in Population Research at The Ohio State University. We also thank Stephen L. Morgan, Sam Field, and Patrick M. Krueger for helpful discussions on methodological issues, although any errors or omissions remain our own.
This research was supported by Grant Number R01HD054866 from the National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health.
1.
Results are substantively identical when non-imputed variables for the dependent outcome are used. We therefore present results for the fully imputed sample so as to maximize the sample size.
2.
Because we obtain similar results with both techniques, we present the OLS results for ease of interpretation. Results of the ordered probit analyses are available from the authors upon request.
3.
An abundance of research documents that the highest rates of nonmarital childbearing are found among women in their teens and twenties (Hamilton et al. 2009), that minority women have higher rates of nonmarital childbearing than do non-Hispanic whites and the foreign born (Hamilton et al. 2009; Hoffman 2008; Lichter et al. 2003; Lichter and Qian 2004; McLanahan 2009; Wildsmith and Raley 2006), and that factors shaping youths’ social class position (e.g., maternal educational attainment and family structure while growing up) are strongly associated with premarital birth (Pearson, Muller, and Frisco 2006; Wu and Martinson 1993). Other studies find strong associations between gender role orientation and educational and family expectations on the likelihood of union formation (Clarkberg, Stolzenberg, and Waite 1995; ![]() ). Many of these variables are also associated with entrance into coresidential unions (both cohabitation and marriage).
). Many of these variables are also associated with entrance into coresidential unions (both cohabitation and marriage).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.