
Abstract
This article explores conditions under which global norms change. I use a case study in which the original interpretation of an international agreement on intellectual property rights was modified to address demands for improved access to affordable AIDS drugs. Conventional theories that focus on international negotiations cannot fully account for the events in this case. Drawing on the theory of recursivity and insights from the literature on diffusion, I suggest that shifts in global norms occur through reactive diffusion of policies across states. Experiences accumulated in this ongoing process of reinvention eventually lead to a new, globally accepted reinterpretation of the original obligation.
Most theories on the creation of global norms and international laws do not discuss the conditions under which these norms and laws may change once in place. Yet experience suggests that norms, laws, and the interpretation given to specific provisions do transform over time. What conditions and processes allow for policy transformations? In this article, I explore this question by looking at the case of intellectual property protection. In 1994, an international agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), signed under the auspices of the World Trade Organization (WTO), obliged all member states to pass laws to improve the protection of patents.
The TRIPS agreement contained provisions describing a number of permissible exceptions, or flexibilities, in the protection of intellectual property rights, but the U.S. government was initially able to enforce a narrow interpretation of those provisions. In the years since, however, many states passed intellectual property laws with explicit references to the controversial exceptions. These exceptions include (1) compulsory licensing in which, without the patent holder’s consent, the government makes direct use of the patent or grants a license to a third-party manufacturer to commercialize a patented invention; (2) parallel importation in which a government buys a patented drug from a legitimate third party; and (3) exceptions from patentability when a product fails to meet the legal conditions to be granted a patent or have a patent renewed (Musungu and Oh 2006). At the international level, two texts delineated the new scope of countries’ rights: the Doha Declaration on the TRIPS Agreement and Public Health adopted in November 2001 (the Doha Declaration) 1 and the Decision on the Implementation of Paragraph 6 of the Doha Declaration on the TRIPS Agreement and Public Health adopted on August 30, 2003 (the August 30 Decision). 2
Expanding TRIPS flexibilities played an important role in the struggle for improved access to AIDS drugs. In the mid-1990s, when scientists first found a combination of antiretroviral drugs (ARVs) effective for the treatment of HIV, brand-name drug companies charged more than $10,000 per patient per year, which HIV/AIDS patients in poor countries could not possibly afford. At the time, pharmaceutical companies did not offer poor countries discounted prices for AIDS drugs and wealthy nations refused to finance the expensive drugs because they did not consider treatment a realistic possibility for poor countries. Partly thanks to the TRIPS exceptions that allowed developing countries to locally produce or import generic versions of patented drugs under certain conditions, the situation today is strikingly different. First-line AIDS drugs in poor countries, most of them generic, can cost as little as $67 per patient per year (Médecins Sans Frontières 2010), 3 and rich countries often fund their purchase. At the end of 2009, approximately 5 million people in low- and middle-income countries, or around 52 percent of people with HIV/AIDS who needed treatment, were receiving antiretroviral drug therapy (World Health Organization 2010). 4
This article describes the processes leading to the global acceptance of TRIPS flexibilities. Conventional theories on global lawmaking focus on negotiations at the international level and they do not capture processes occurring at the national level that, I argue, often determine which position will prevail in negotiations. Halliday and Carruthers’s (2007, 2009) theory of recursivity convincingly addresses this issue by looking at the iterative cycles between global norm making and national lawmaking. When analyzing conditions for national divergence, however, the theory focuses on local processes and overlooks a more significant factor that allows national lawmaking to have a recursive effect at the international level, namely, the reactive diffusion of policies across countries. I suggest that in the course of implementing global obligations, states often deviate from formal interpretations. Some states’ divergences influence other states’ choices, which build on but may further deviate from previous divergences. Experiences accumulated in this ongoing process of reinvention eventually create, and may be formally recognized as, a new globally accepted reinterpretation of the original law.
Making and Remaking of Global Norms: Current Views
As international declarations, agreements, and laws have become central to management of the global economy, they have reignited scholarly interest. Existing theories, however, cannot adequately explain the evolution of intellectual property protection of AIDS drugs.
Conventional approaches to international relations often focus on formal negotiations among states. Outcomes of these negotiations are expected to reflect the military, economic, or symbolic power of participating states (Baldwin 1993; Gruber 2000; Mearsheimer 1994). International laws and norms may transform once in place, either when dominant states are interested in changing the existing rules or when participating states’ relative bargaining leverage changes. Following this conventional logic, most scholars who study the intellectual property protection of AIDS drugs look at states’ relative bargaining leverage to explain TRIPS and the Doha Declaration. According to this view, the U.S. government pushed TRIPS on other countries. In Doha, the U.S. government was not able to protect its pharmaceutical companies’ economic interests and preserve the original interpretation of TRIPS due to the successful collective resistance of developing countries (Shadlen 2004) aided by transnational AIDS activists (Drahos 2002; Klug 2005; Sell 2003).
Negotiations are clearly influenced by participating states’ material and symbolic powers. But an analysis of states’ relative influence in the course of negotiations fails to capture the conditions that led to the Doha Declaration and the August 30 Decision. By the time negotiations were held in Doha in November 2001, many developing countries had codified and implemented flexibilities that were later protected by the Doha Declaration (Musungu and Oh 2006) and the U.S. government had already withdrawn many of its initial objections. This suggests that the heart of the story lies with developments that preceded the Doha Declaration. Specifically, states’ reliance on flexibilities before their formal acceptance at Doha suggests that national processes may be fundamental to these international developments.
Most scholars concerned with the effect of national developments on the international level study how domestic politics affect member states’ negotiating positions (Putnam 1988). In contrast, sociological theories examine processes following, rather than preceding, successful negotiations. World polity theorists have shown that countries often adopt international norms only ceremoniously and local processes and institutions still determine national policies (Meyer and Rowan 1977). More recently, Halliday and Carruthers (2007, 2009) have argued that such divergences at the local level also shape and may transform the original international model.
According to Halliday and Carruthers (2007, 2009), legal globalization is caused by three sets of recursive cycles, where in each cycle a given law or norm can be continuously transformed. The first cycle describes the process of loose coupling, where local processes—recursive cycles of lawmaking and law implementation—may cause national laws to diverge from the external model. The second set describes iterative cycles of norm making at the global level. The third set is at the intersection of the other two, where global norms constrain national lawmaking but divergences that emerge when implementing global norms at the national level influence later developments at the international level. The third cycle implies that analyzing divergence in local responses to international laws is necessary for understanding norm remaking at the international level. 5
Recursivity theory offers an original contribution to the question of changing global norms by showing that countries’ divergent implementation of original obligations has the paradoxical effect of potentially transforming these obligations. Halliday and Carruthers’s analysis, however, assumes that states respond to international obligations and potentially reshape them independently of each other. In their case studies of insolvency law, the circumstances they identify to explain South Korea’s, Indonesia’s, and China’s deviations from international obligations are entirely local (Halliday and Carruthers 2009). They do not consider the effect of other countries’ responses to pressure to adopt new insolvency laws. As a result, it is not entirely clear how recursive cycles at the national level could affect existing international norms.
As convincingly argued in the extensive literature on diffusion, however, local divergences are unlikely to occur independently. Two arguments on diffusion, regarding learning and reinvention, are particularly useful. First, states learn from each other. The literature on diffusion, including specialized studies on the global diffusion of public policies, shows that the spread of policies reflects not only countries following international laws or norms, but also countries being influenced by other countries’ policy choices, often through learning or emulation (Henisz, Zelner, and Guillén 2005; Simmons, Dobbin, and Garrett 2006; Wejnert 2002; Weyland 2005). Even when policies originate at the international level, dissemination often occurs laterally, because states are influenced by international events as well as by other states. The implications, which studies do not always note, are significant: lateral dissemination of international obligations means that if one country diverges from the original interpretation, this divergence will influence other countries’ policy adoptions.
The second insight is that the process of diffusion involves reinvention (Glick and Hays 1991; Hays 1996; Rogers 1983). The literature on global diffusion normally describes diffusion as a static process, so policies that spread from one country to another are “treated as an unchanging object” (Strang 2010:10). When these scholars describe divergence in implementation, they expect local divergence not to affect the content of what is being diffused. In contrast, scholars looking at policy diffusion in U.S. states show that states do not blindly follow early innovators. Rather, states modify the core innovation during the diffusion process (Glick and Hays 1991; Rogers 1983), which allows for a continuous process of reinvention. This process also affects early adopters, who may “amend their laws to fit within the range created by the recent ones” (Glick and Hays 1991:847). Regarding implementation of global obligations, this implies that countries not only learn from others about possible deviations, but countries can also deviate from the divergences they encounter.
Reactive Diffusion and Accumulated Experiences
This article argues that transformation in global norms, such as norms regarding the intellectual property protection of AIDS drugs, often depends on cross-national influence and collective accumulation of experiences. This argument emphasizes the recursive interchange between local divergences and global obligations, but it also stresses that the national divergences recycled to the international level are not developed independently of each other but emerge from cross-national diffusion, whereby a country’s response is influenced by other countries’ responses to the same pressures. Moreover, this cross-national diffusion is reactive: although a country may be influenced by another country’s policy innovation, a state is also likely to diverge from the innovation, often through broadening the range of flexibilities already used by others (layering) and utilizing new types of flexibilities (branching off). This accumulation of experiences—of countries successfully implementing policies that diverge from the original obligation—enables local divergences as they travel across states to be recycled back to the international level, leading to a formal change in global norms.
Diffusion of policy innovation
National divergences do not stay at the domestic level. When one country deviates from the international template, it introduces the choice of alternative policies to other countries. Hence, when a state chooses its response to a global norm or law, it is likely influenced by local circumstances, as emphasized by recursivity theory, and also by divergences that emerged in other states. Brazil’s policies on intellectual property, for example, were informed not only by TRIPS but also by South Africa’s and Thailand’s divergences from TRIPS. 6
Reinvention through reactive diffusion
The process of cross-national diffusion is reactive rather than static. 7 In the process of learning and emulation, an innovation by one state is diffused to but also modified by another state; subsequent adopters may choose among these innovations or modify the policy again to create another model. As a result, the original model continually transforms. In implementing TRIPS, countries were influenced by other legal interpretations that highlighted permissible flexibilities. Countries such as Brazil and Thailand, however, did not simply copy strategies adopted by others. They developed their own divergent interpretations of the new legal possibilities that built on, but deviated from, other countries’ earlier reinventions.
This ongoing change is due to “diffusion entrepreneurs,” namely, actors who provided information on how policies were modified elsewhere and how those modifications could be further altered (Braithwaite and Drahos 2000:585). In the diffusion of TRIPS, four types of diffusion entrepreneurs are central: domestic and transnational activists who transplanted strategies and responses from one place to another; 8 state officials who shared their experiences with other governments; officials of international organizations who used international platforms “to bring people together so they do what the international organization cannot do itself”; 9 and commercial enterprises, mostly generic drug manufacturers, who could profit from diffusion of TRIPS flexibilities.
Accumulated experiences
In cases where states diverge from an international model and this divergence leads to additional policy reinventions through reactive diffusion, the recursive cycle from the national back to the international—leading to revisiting of the original model—can be explained by states’ accumulated experiences. In the process of reactive diffusion, countries experiment with divergent interpretations of an international model, seek versions of policies more in line with their needs or preferences, and, most importantly, discover whether they can preserve these policies in the face of external opposition. These experiences lead to formal renegotiations at the international level and can determine their outcomes. In the case of TRIPS, by the time of the Doha negotiations, due to experiences in South Africa, Brazil, and many other countries, the right to use flexibilities was no longer considered controversial. The Doha Declaration was a defining moment in the history of TRIPS because it formalized at the international level what was already legitimately practiced in many states, not because it allowed for flexibilities.
To summarize, local divergences of an international model are not isolated events, in which each state acts independently. Instead, often with the help of diffusion entrepreneurs, divergences occur through reactive sequences in which policies are modified in the process of diffusion from one state to another. Accumulation of successful experiences enables states that support modification of global norms to impose such change at the international level.
Studying Reactive Diffusion: Data and Methods
To trace diffusion of TRIPS flexibilities across countries and over time, I draw on evidence I obtained from newspaper reports, interviews, and official documents. I collected and read all articles on intellectual property rights and AIDS drugs from the main English-speaking newspapers in the United States, the United Kingdom, South Africa, Thailand, and India. I took the following steps to allow for systematic analysis of the information in newspaper reports. First, using an online database, ProQuest, I created an original dataset that includes all reports from major U.S. newspapers (i.e., Boston Globe, Christian Science Monitor, New York Times, Wall Street Journal, and Washington Post) from January 1, 1994, to December 31, 2010, and that contain “acquired immune deficiency syndrome (AIDS)” and either “intellectual property,” “patents,” or “generic drugs.” This dataset includes 424 articles. Second, I imported the dataset to research software, NVivo; it allowed me to search the original dataset for the number of articles in which a country was mentioned (sources) and for the number of times a country was mentioned in any given article (references). I used this data to identify the countries most actively involved in debates over access to AIDS drugs and the period in which they were active. Third, using NVivo, I searched the original dataset for the frequency with which two countries were mentioned in the same article. I used this data to identify likely routes of diffusion from one country to another.
In addition to analysis of newspaper reports, I conducted 22 interviews, most of them during 2008 and 2009, in Switzerland, South Africa, the United States, and India. I interviewed government officials in the United States and South Africa; AIDS activists from Médecins Sans Frontières (MSF), Consumer Project on Technology (CPTech), Treatment Action Campaign (TAC), and the International Centre for Trade and Sustainable Development (ICTSD); representatives of brand-name and generic pharmaceutical companies; representatives of the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA); and officials of the World Health Organization (WHO), the Joint United Nations Programme on HIV/AIDS (UNAIDS), the World Bank, and the Global Fund to Fight AIDS, Tuberculosis, and Malaria. I selected respondents for their personal involvement in the events analyzed in this study and I made sure they represented all interested parties and diverse geographic regions. I identified actors through newspaper articles and official reports (see below). In most cases, the individuals I contacted agreed to have a meeting and some also introduced me to others. In the two cases in which the person I contacted was not available, I was able to interview other individuals in the same organization. All interviews, with the exception of one follow-up interview over the phone, were conducted in person and were normally one to two hours in length. I conducted interviews in English, and most were recorded and later transcribed. Interviews were semi-structured and questions focused on events in which respondents were personally involved. Respondent information was instrumental in identifying the most important events influencing the use of TRIPS flexibilities and obtaining detailed accounts of those events. These accounts helped me identify the process of reactive diffusion by revealing how governments’ actions were often informed by other governments’ decisions and how these actions often consciously deviated from the claimed inspiration.
I supplemented newspaper articles and interviews with official reports and documents prepared or commissioned by government agencies and international organizations, including the WHO, UNAIDS, the World Bank, the Global Fund, and, in the United States, the General Accounting Office and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). Other useful reports were prepared by nongovernmental organizations, including MSF, Oxfam, and South Centre. Most documents were available online, with the exception of some reports prepared by the WHO Director-General’s Office and minutes of the annual meetings of WHO member states. I obtained these materials from the WHO library in Geneva. Altogether, I obtained 57 relevant documents as well as minutes of all WHO meetings between 1996 and 2009 when delegates discussed the issue of intellectual property protection and recounted their experiences with TRIPS flexibilities. These documents were helpful in providing reliable data on epidemiological patterns, technical legal issues, and negotiations over TRIPS flexibilities in numerous countries and at the international level.
Newspaper reports, interviews, and documents provided information on implementation of TRIPS in various countries and on struggles that preceded or ensued from that implementation. The NVivo dataset of articles on intellectual property rights and AIDS drugs was especially useful for tracing the route of diffusion across places and over time. By counting the number of sources for each of the 135 countries identified by the World Bank as low- or middle-income, I could identify the countries most involved in the emerging struggle in any given year (see Table 1). 10 Because the number of times a country is mentioned in an article is a reliable indicator of the country’s centrality to the article, Table 1 depicts the number of references, rather than the number of sources, per year for each of the 15 most frequently mentioned countries. The frequency with which a country is mentioned is likely influenced by newspapers’ tendency to report on large countries and on countries particularly affected by AIDS. Nonetheless, this survey allows me to identify (1) countries that were most likely involved in the debate over intellectual property rights and access to AIDS drugs, (2) the relative significance of each country to the story, and (3) the timing of different countries’ engagement. Countries most often mentioned—South Africa, Brazil, India, China, and Thailand—are likely the ones with a significant role in the process of diffusion (on China, see below). The period in which countries were mentioned, in turn, allows me to follow the debate as it traveled from one place to another over time.
Number of Times per Year a Country Was Mentioned in Newspaper Articles on the Topic of Intellectual Property and AIDS, 1994 to 2011
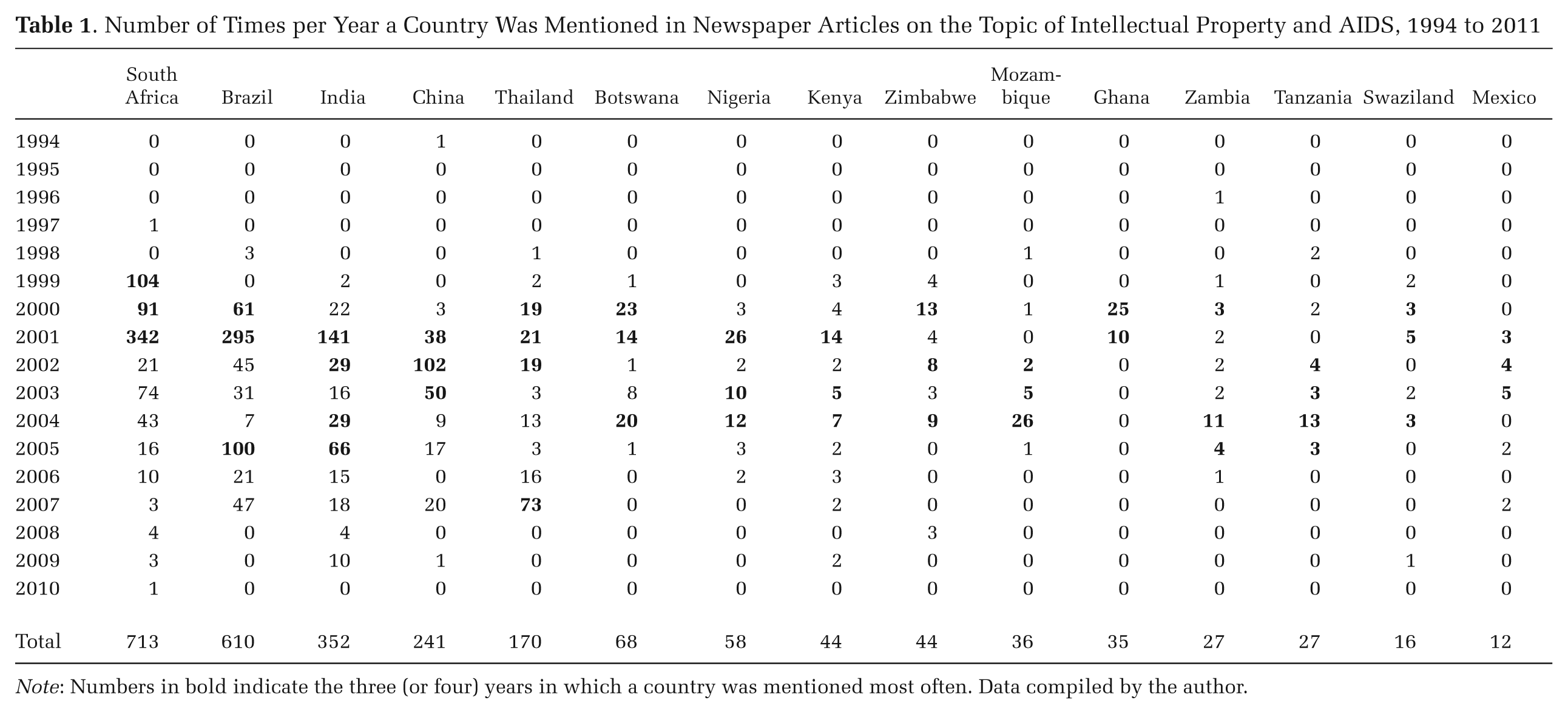
Note: Numbers in bold indicate the three (or four) years in which a country was mentioned most often. Data compiled by the author.
Once I established the list of potentially involved countries, the second challenge was to establish the possibility of diffusion among these countries. Table 2, which indicates how often two countries were mentioned in the same article, reveals the presence of links between some paired countries but not others. 11 Newspaper articles often mentioned more than one country in the same article, both to describe similar developments and to show cross-national influences. Patterns revealed in Table 2 suggest two possible pathways of diffusion: across countries in the same geographic region (e.g., Mexico and Argentina; Ethiopia, Nigeria, and Kenya) or, more commonly, from a small number of influential countries—namely, South Africa, India, and Brazil—to others. For example, the title of one newspaper article announced “India May Follow Brazil Patent Law” (Kamath 2001), and another article quoted a Chinese official saying, “We would like to do as Brazil and India have done,” when announcing a plan to invoke compulsory licensing (Chang 2002). The very infrequent cross-referencing of China with other countries, shown in Table 2, confirms that China has not played an important role in the diffusion process. As for Thailand, Table 2 suggests that its influence on other countries is likely mediated through its influence on diffusion entrepreneurs such as India and Brazil. One Wall Street Journal (2007) editorial illustrates this pathway: “Thailand’s decision [to invoke compulsory licensing for a drug for heart disease] is already reverberating worldwide. Brazil . . . is paying attention.”
Of the Two Countries Being Compared, the Percentage of Articles on the Topic of Intellectual Property and AIDS that Mention the Country Less Frequently Cited
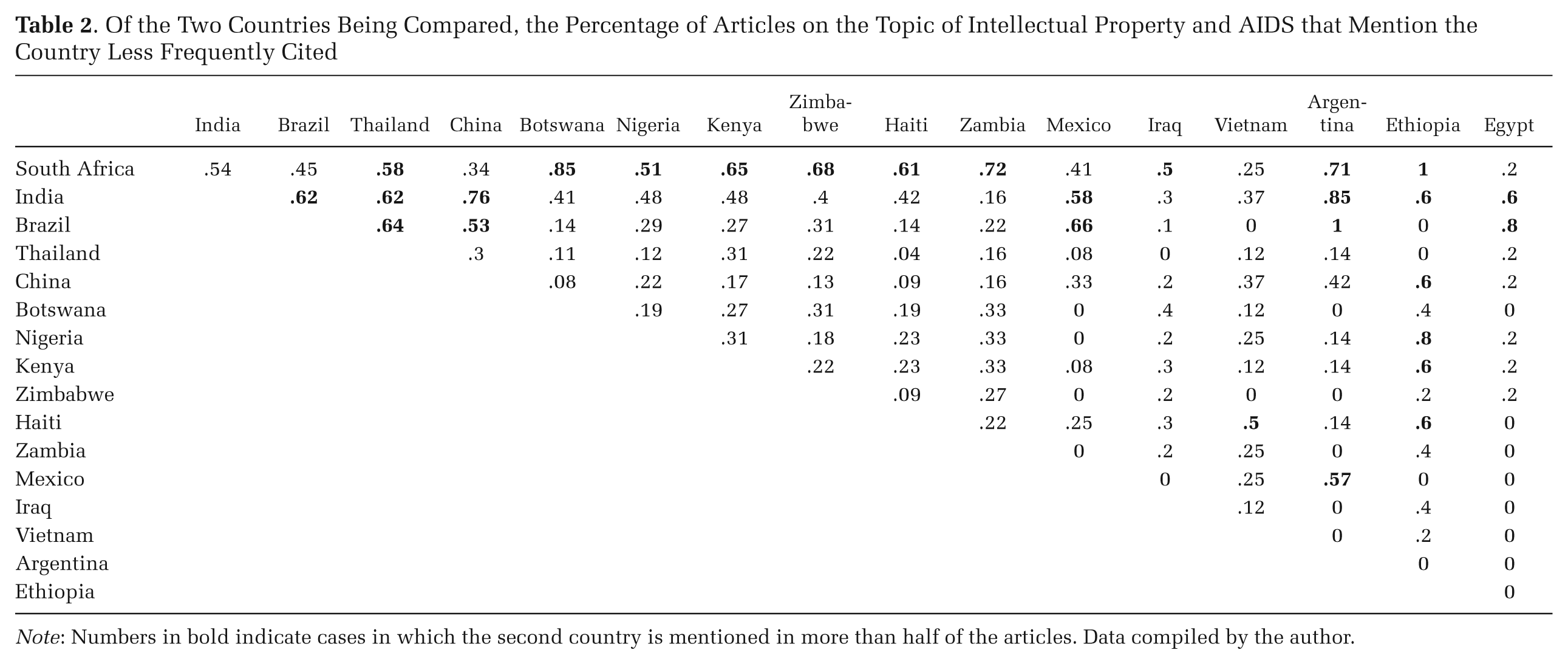
Note: Numbers in bold indicate cases in which the second country is mentioned in more than half of the articles. Data compiled by the author.
To summarize, a systematic survey of newspaper articles suggests that a large number of countries were involved in the debate over affordable access to AIDS drugs and points to the likely existence of lateral links between innovators and other middle- and low-income countries. The remainder of this article shows that these lateral links led to reinvention through reactive diffusion and how, in the process of diffusion, a new global norm emerged.
From Trips to Doha and Beyond
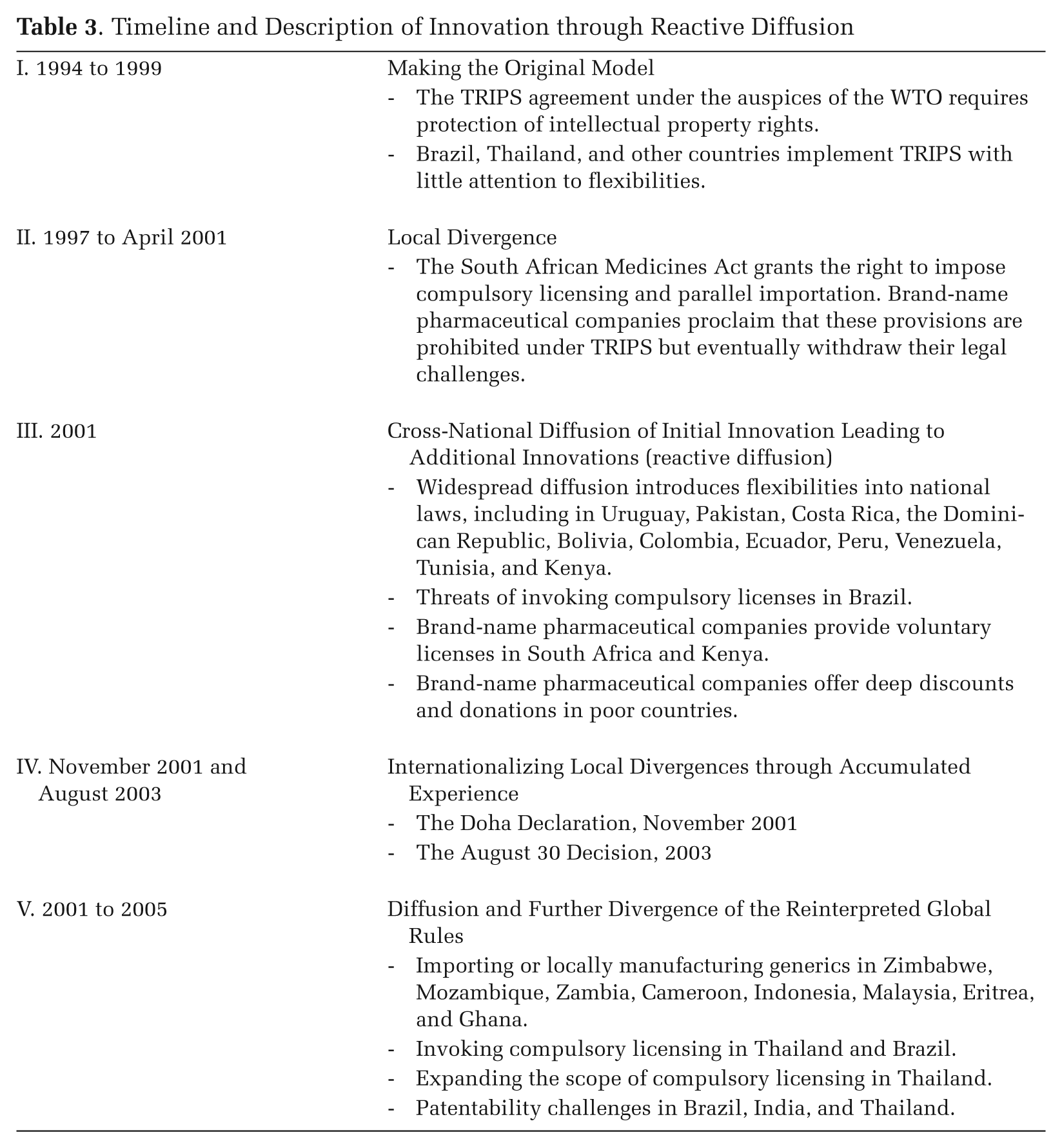
In the face of common challenges, governments often learn from each other. In confronting AIDS, governments were often explicit in referring to others’ experiences as a source for information and legitimacy. To promote distribution of free condoms in India, for example, a senior Congress Party leader “pointed out how the government of Thailand undertook vigorous condom distribution programs and succeeded in controlling the spread of the deadly virus” (Times of India 2005). Governments also learned from others about TRIPS flexibilities. Countries combined this learning with local experimentation, leading to branching off and layering of previous policy innovations and, eventually, to a global normative shift regarding the intellectual property protection of AIDS drugs (see Table 3).
Timeline and Description of Innovation through Reactive Diffusion
Making the Original Model: Formulation and Initial Spread of TRIPS
When the first HIV drug, zidovudine (AZT), was approved by the U.S. government in 1987, some middle-income countries took advantage of their pharmaceutical manufacturing capability to produce generic versions of the drug, mostly for local use. In Brazil, for example, the patent law of 1971 did not provide patent protection to pharmaceuticals and the Constitution of 1988 established the right of access to basic medicines. The state-owned laboratory Farmanguinhos began manufacturing AZT in 1991 (Souza 2007). In Thailand, the 1990 Social Security Law committed the government to providing basic health care for its citizens and the state-owned Government Pharmaceutical Organization (GPO) began producing AZT in 1992 (Ford et al. 2007). India’s Patent Act of 1970 allowed patents to be granted for chemical processes, but not for the product itself, which allowed manufacturers to bypass patents by slightly manipulating the production process. Cipla, a private Indian company, introduced a generic version of AZT in 1994, offering it for sale in India and foreign markets (Lancet 2004).
TRIPS, signed by WTO member states in 1994, put into question the future legality of local manufacturing of generic drugs, just two years before the prohibitively expensive ARVs were introduced. This international agreement to strengthen global protection of intellectual property required, by the end of a transition period, patent protection for any invention in any field of technology. Key requirements included patent protection for a minimum of 20 years and protection for a product and its chemical production process.
Developing countries were granted a 10-year transition period until 2005 to implement TRIPS. Although many of these countries initially opposed TRIPS (Sell 2003), some implemented the agreement earlier than required. The Brazilian government, which was under pressure to improve economic relations with the United States, passed the Industrial Property Law in May 1996 (Ford et al. 2007). This law provided a number of strong patent protections, but these protections did not apply to products that had been commercialized anywhere in the world before May 1997. As a result, 10 AIDS drugs remained unpatented and could legally be copied. The same year, Brazil also passed a law requiring the government to provide free AIDS medication. By 2001, Farmanguinhos produced eight of the twelve AIDS medications then available in Brazil (Souza 2007). In Thailand, under threat from the U.S. government that it would limit textile imports, the government passed a restrictive new patent law in 1992 (Ford et al. 2007). In 1999, again in response to U.S. threats, the Thai government took additional measures restricting the use of compulsory licenses and parallel importing (Wilson et al. 1999).
Initially, member states accepted a narrow interpretation of the exceptions allowed under TRIPS. Local divergences found in Brazil, Thailand, or elsewhere (Musungu and Oh 2006) attracted little attention even when, as in the case of Brazil, some provisions were challenged at the WTO (see below). The policy innovation offered by South Africa, however, had a very different fate.
Local Divergence: South Africa’s Reinterpretation of TRIPS
In South Africa, local conditions raised concerns regarding implementation of the TRIPS agreement. The Health Minister in South Africa’s first democratic government, Nkosazana Dlamini-Zuma, understood that a rigid implementation of TRIPS would have especially harmful consequences in a country confronting a devastating AIDS crisis and facing challenges associated with reversing its apartheid system. South Africa’s position on TRIPS was also informed by its new constitution, which established health care as a right, and by the existence of domestic pharmaceutical manufacturing capabilities.
In addition to local conditions, South Africa’s response to TRIPS was shaped by a WHO report, Globalization and Access to Drugs: Implications of the WTO/TRIPS Agreement (WHO 1997). The report, prepared by the WHO’s Action Programme on Essential Drugs, insisted that TRIPS, if interpreted correctly, could achieve an appropriate balance between intellectual property protection and developing countries’ health needs. According to the reading of Articles 30 and 31 of TRIPS offered in the report, the agreement “expressly provide[d] two means of obtaining exceptions and limiting the exclusive rights conferred by the patent on its owner,” namely, compulsory licensing and parallel imports (WHO 1997:33). The WHO’s report was the first to provide a legal interpretation of TRIPS that allowed developing countries to consider exceptions to intellectual property protection not as acts of subversion, but as loyal implementation of its provisions. 12 In November 1997, Dlamini-Zuma won parliamentary passage of the Medicines and Related Substances Control Amendment Act (Medicines Act). Clause 15(c) of the Act granted the government the right to impose compulsory licensing and parallel importation to allow the supply of more affordable medicines. 13
The U.S. government and the brand-name pharmaceutical sector vigorously criticized the WHO report, but their criticism was mild compared to the campaign they launched against the South African government for following the WHO’s interpretation. Indeed, what likely made the South African case particularly influential was not its explicit divergence from the international norm, but that the government prevailed over the very strong opposition the Medicines Act triggered. Provoked by the explicit challenge to their patents and concerned that the South African example would disseminate to other countries, 14 brand-name pharmaceutical manufacturers closed their South African factories, cancelled investments and expansion plans, and ran scare ads suggesting that babies could be hurt by counterfeit generic drugs (McNeil 1998). In February 1998, 40 multinational drug companies, together with the Pharmaceutical Manufacturers Association of South Africa, filed a lawsuit against the government alleging that compulsory licensing and parallel importing were prohibited under TRIPS (Heywood 2001).
The Clinton administration supported the pharmaceutical sector by imposing economic sanctions on the South African government and delivering diplomatic threats (Bond 2003). But an activists’ network that included the New York AIDS activist group ACT UP and Ralph Nader’s CPTech heavily criticized these actions. When it became clear the issue could negatively affect gay and black voters’ support of Vice President Al Gore’s candidacy for the presidential election, Gore negotiated a deal with the South African government that allowed the United States to withdraw its objections (Ayres 1999).
AIDS activism also played a decisive role in South Africa. The night before a court hearing in March 2001, Treatment Action Campaign (TAC) and the South African trade union COSATU staged an all-night vigil and protest outside the court building and the U.S. embassy. A transnational network of activists organized demonstrations in 30 other cities worldwide. At the courthouse the following day, activists won an important victory when Judge Bernard Ngoepe allowed testimonies from HIV/AIDS patients (Heywood 2001). By the time the case resumed six weeks later, the transnational activist network had swayed public opinion in developed countries and gained the support of unlikely allies, including the European Union, the Dutch government, the World Bank, and even WTO officials (Sell and Prakash 2004). Soon after, in the “hope to extricate themselves from a public-relations nightmare” (Block 2001), drug companies withdrew the case. After five years, South Africa’s interpretation of TRIPS had prevailed.
In South Africa, divergence from a narrow interpretation of TRIPS was only one step in a much longer struggle for drug treatment (Friedman and Mottiar 2005). But South Africans were not the only ones affected by the Medicines Act, as the legal developments in their country—although heavily informed by unique conditions—spread beyond the local level. As we saw, the struggle over the Medicines Act led some governments and international organizations to modify their positions. In the United States, President Clinton issued an executive order that prohibited pressuring any sub-Saharan African country into forgoing strategies to increase access to AIDS drugs (Sell and Prakash 2004). The Clinton administration intended these concessions to serve as an exception, but diffusion of South Africa’s policy innovation to other developing countries would make such exceptions the rule.
Diffusion of Initial Innovation Leading to Additional Innovations
The policy innovation introduced by South Africa is consistent with an expectation of divergence. But studies on recursivity tell us little about how policy innovation in one locality affects policies in other sites. In the case of South Africa, two surprising things occurred. First, the South African experience influenced policy diffusion in other countries, as governments learned not only from the original TRIPS interpretation but also from South Africa’s experience of challenging that interpretation. Second, new policy innovations were introduced in the process of that diffusion.
The South African challenge to TRIPS was a historical turning point. Years later, when officials of the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA) assessed strategies used by the pharmaceutical sector to protect its patents, they readily confirmed the “major, major mistake” of “suing Nelson Mandela.” These IFPMA officials articulated a common perception when they referred to the South African “huge faux-pas” as the watershed in a process that gradually but dramatically weakened pharmaceutical companies’ normative and legal position. 15 As soon as it became clear that the South African government would likely prevail, officials in other developing countries, with the support of health activists, began to focus on TRIPS flexibilities as the central strategy to improve access to AIDS drugs. 16 They saw the South African legal challenge as a test case, and with the failure of that challenge, they considered it unlikely that drug companies would campaign against other developing countries or that Western governments would publicly support such campaigns (Mutume 2001). Following South Africa, the campaign for access to affordable AIDS drugs moved to Kenya, where the Parliament passed a law allowing exemptions to international patent law (Itano 2001), and other nations similarly experimented with TRIPS flexibilities to lower prices of AIDS drugs. Illustrating the reactive nature of diffusion, countries also modified what they learned from the South African experience.
Many countries passed new intellectual property laws to comply with TRIPS, and many of the laws included explicit references to permissible flexibilities, including compulsory licensing, government use, parallel imports, and patent exceptions (Musungu and Oh 2006). Figure 1 depicts the aggregate number of flexibilities explicitly permitted and the aggregate number of flexibilities not mentioned or excluded in intellectual property laws passed in various countries from 1997 to 2005. Although they validate the expected variation across countries (Deere 2008), the results also make clear the widespread diffusion of flexibilities between 1999 and 2001. Of the 23 countries that passed intellectual property laws during that time, only one country did not allow for some form of compulsory licensing or government use, and many countries allowed for parallel imports or patent exceptions. Uruguay, Pakistan, Costa Rica, the Dominican Republic, Bolivia, Colombia, Ecuador, Peru, Venezuela, Tunisia, and Kenya were particularly expansive in their legislation of flexibilities.
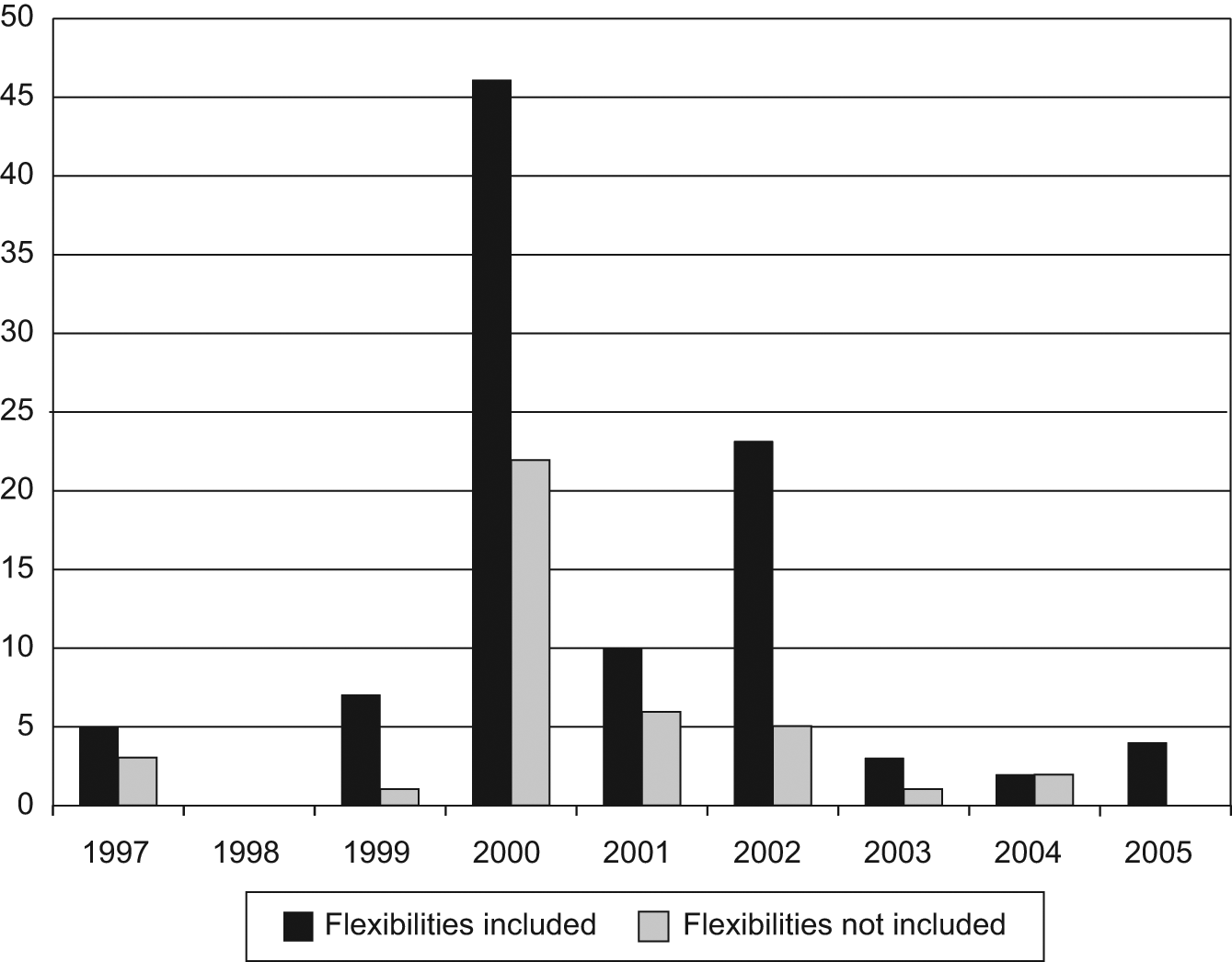
Number of Flexibilities Permitted in National Laws, 1997 to 2005
The move from legislation to implementation was slower and involved even greater divergence from others’ experiences, as evidenced by the cases of Thailand and Brazil. While new patent laws in both countries allowed for some flexibilities, the Thai and Brazilian governments did not initially use these public-health safeguards because they wanted to avoid U.S. retaliation. When the Thai government refused a GPO request for a compulsory license to produce didanosine (ddI), an official explained that, “Thailand hasn’t moved to exercise its compulsory licensing rights under TRIPS . . . as Thai officials nonetheless fear trade reprisals” (cited in Oxfam 2001:6). Brazil experienced the threat of trade reprisals first-hand; in January 2001, at the WTO, the U.S. government challenged Article 68 of the Brazilian Industrial Property Act that authorized the government to invoke compulsory licensing for goods that were not manufactured locally within three years of receiving patent protection.
The South African government’s success in defending the Medicines Act suggested to these governments that they, too, could take advantage of TRIPS flexibilities. The Brazilian government saw the changed circumstances when in June 2001, the U.S. government agreed to a compromise with Brazil rather than pursuing the WTO case. Commentators agreed that the U.S. retreat was triggered by developments in South Africa, which turned its case against Brazil into a political embarrassment (Sell and Prakash 2004). Subsequently, the Brazilian government became more confrontational in utilizing TRIPS flexibilities. As we saw, Brazil was locally manufacturing most of the AIDS drugs it offered, but it was importing two brand-name drugs, efavirenz (licensed by Merck) and nelfinavir (Roche), which accounted for a disproportionate 36 percent of Brazil’s expenditure on AIDS medications. When Merck and Roche failed to offer acceptable discounts on these drugs, the Brazilian Health Minister, José Serra, announced he would issue compulsory licenses if the pharmaceutical companies did not lower their prices (Souza 2007). After uneasy negotiations, Merck agreed to cut the prices of efavirenz by 59 percent and another drug, indinavir, by 64.8 percent, and Roche agreed to drop the price of nelfinavir by 40 percent (Jordan 2001a).
While Brazil learned from the South African example, other countries were learning from Brazil. The U.S. decision to drop the WTO case, for example, was “interpreted by . . . the Indian industry as the opportunity to model India’s patent law along that of Brazil” (Kamath 2001). Brazilian officials proactively pushed to make their strategies a source of imitation. José Serra, for example, announced that tactics Brazil had used to receive price concessions from Merck and Roche could be employed by other developing countries (Donnelly 2001). Realizing that a country’s bargaining leverage depended on its manufacturing capabilities, UN reports called on least developed countries to “follow Brazil’s example” of local manufacturing (Mutume 2001: 14), and the Brazilian government invited health officials from several African and Caribbean countries to visit Farmanguinhos and promised support to set up their own local production (Jordan 2001b). In August 2002, leaders from several Portuguese-speaking countries signed on to a program to share in Brazil’s know-how (Downie 2002).
Some countries sought ways to reduce prices of patented drugs, but in other countries local generic manufacturers pressed drug companies to voluntarily license their key AIDS drugs. In South Africa, soon after termination of the court case, Aspen Pharmacare received assurances from Bristol-Myers and others that they would not sue if Aspen manufactured and sold their AIDS drugs. 17 South African activists initiated legal challenges against Glaxo-SmithKline and Boehringer Ingelheim, and in out-of-court agreements the companies agreed to grant voluntary licenses for production of their AIDS drugs (Nelson 2003). In Kenya, the government was able to obtain voluntary licensing agreements (Musungu and Oh 2006).
Countries without manufacturing capabilities also benefitted from the pharmaceutical debacle in South Africa, because in an attempt to bolster their image and demonstrate that intellectual property was not an obstacle to gaining access to affordable drugs, pharmaceutical companies began to offer their drugs at deeply discounted prices (Petersen 2001). In March 2001, for example, Merck announced discounts of 90 percent for two of its AIDS drugs in sub-Saharan Africa. The real decline in prices occurred, however, when manufacturers of generic drugs offered AIDS drugs at much lower prices.
During the South African conflict—partly in an attempt to undermine pharmaceutical companies’ moral standing by showing how cheap it was to produce AIDS drugs—activists began talks with generic manufacturers. 18 Following these discussions, Dr. Yusuf K. Hamied, the Chairman of Cipla, a generic pharmaceutical manufacturing company in India, announced his company would sell a combination of three AIDS drugs for the shockingly low price of $600 per patient per year. According to Hamied, this price would still allow him to make a profit (Specter 2001). Because India did not have to fully implement TRIPS until 2005, Indian manufacturers could legally produce generic drugs and Cipla’s entrepreneurship was soon imitated by other Indian manufactures. The price for AIDS drugs soon dropped to $295 per patient per year. Soon, Nigeria, Cameroon, Algeria, Kenya, and Botswana announced plans to import drugs from India. Countries that were still “too scared of the [U.S.] government to buy generics” also benefitted, as brand-name pharmaceutical companies responded to the generic threat by substantially dropping the price of their drugs (Boseley 2003). In June 2001, for example, GlaxoSmithKline announced price reductions of about 80 percent for three AIDS drugs in 63 countries, and Pfizer offered fluconazole for free in the least developed countries. Largely as a result of this competition between brand-name and generic drugs, the price of AIDS drugs radically dropped. Figure 2 shows the reduction in prices quoted by brand-name and generic manufacturers for developing countries of one type of a fixed-dose combination.
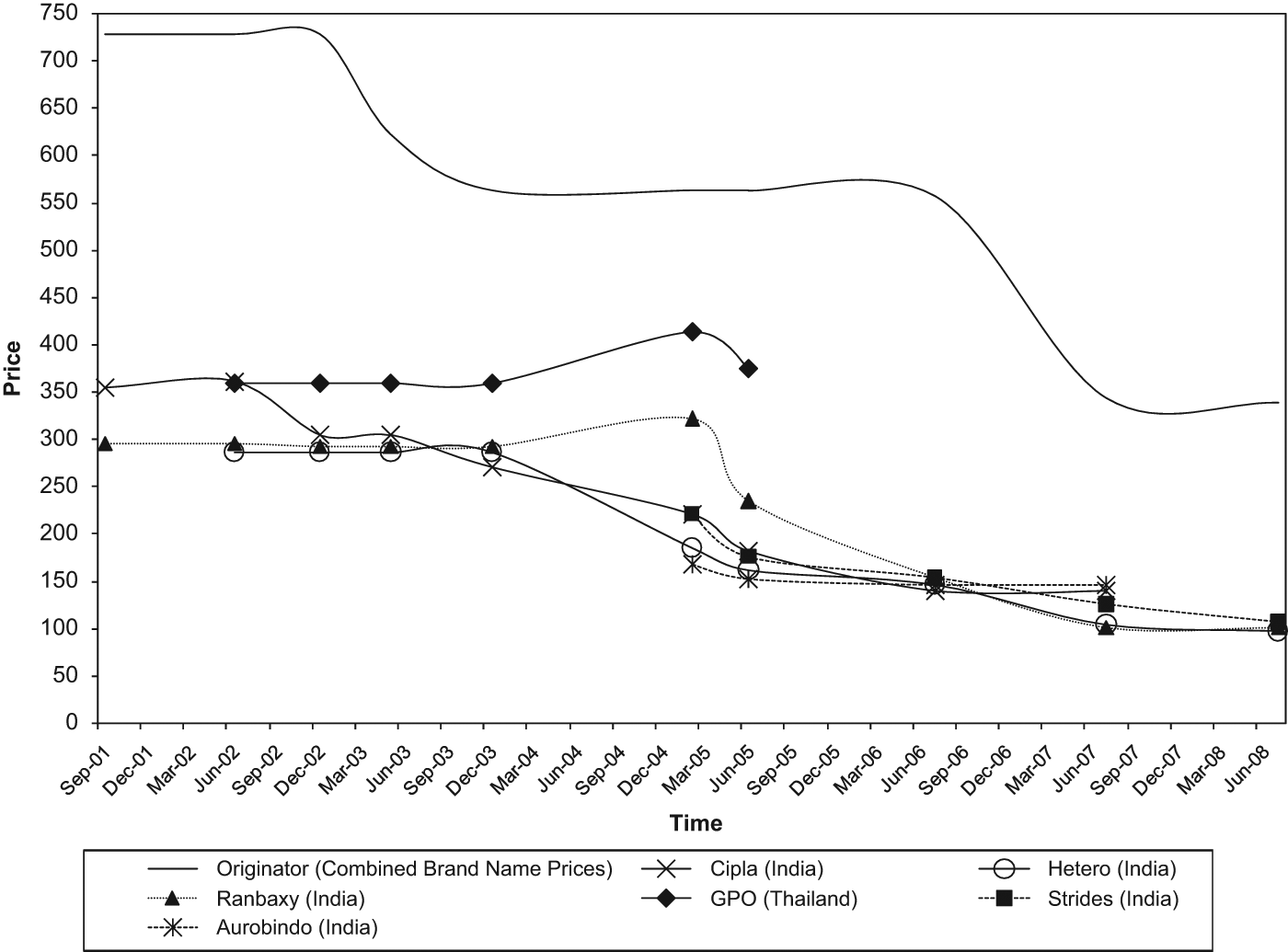
Prices Quoted for a Fixed-Dose Combination of 3TC/d4T/NVP, 2001 to 2008
In short, South Africa’s Medicines Act convinced other states that they, too, could find ways to push down the price of AIDS drugs. While learning from others’ experiences, countries also found variations better suited to their local circumstances. Through a process of reactive diffusion, the suitability of TRIPS flexibilities and their legitimate scope was tried in different fashions in different places, creating accumulated experiences that, by late 2001, led to reframing of the original global norm.
Internationalizing Accumulated Experiences
The South African debacle made brand-name pharmaceutical companies less likely to challenge generic manufacturing of their drugs, but developing countries were still worried that the United States and other governments supporting these companies would use TRIPS to challenge their actions. At the Fourth WTO Ministerial Conference in November 2001, a coalition of more than 50 developing countries led by Brazil, South Africa, India, Kenya, and Zimbabwe declared they would not agree to a new round of trade negotiations without a statement that would clarify their rights to issue compulsory licenses and to authorize parallel importation (Shadlen 2004).
Scholars analyzing the negotiations rightly note that developing countries enjoyed a powerful moral argument and a stable coalition that was greatly strengthened by the support of AIDS activists, and they identify a number of contingent conditions that further weakened the opposition of the United States and other rich countries (Klug 2005; Sell 2003). But this focus on countries’ bargaining leverage overlooks the essential fact that the outcome was mostly predetermined by the successful diffusion of flexibilities in many countries. As we saw, by the end of 2001, many developing countries were already acting according to their preferred interpretations of the TRIPS flexibilities, the pharmaceutical sector had lost the normative battle, and the U.S. government confirmed it would not challenge sub-Saharan African countries and compromised in the WTO case it had launched against Brazil. International declarations at the WHO and the UN Sub-Commission on Human Rights helped disseminate a global position and consolidate it at the international level (Schwartländer, Grubb, and Perriëns 2006). Hence, the debate had largely already been won in the process of reactive diffusion: countries knew what types of exceptions would not be blocked by the pharmaceutical sector or Western governments. The outcome at Doha was a major symbolic victory. But rather than collective action at the international level, it was the accumulation of policy innovations at the national level that forced other countries to accept the legitimacy of TRIPS flexibilities.
Hence, the scope of permissible flexibilities negotiated in Doha had largely been determined through the accumulated experiences of countries that had passed laws and implemented them. Although not without debate, WTO member states agreed on a document, the Doha Declaration, that dramatically stated, “We agree that the TRIPS Agreement does not and should not prevent members from taking measures to protect public health. . . . We reaffirm the right of WTO members to use, to the full, the provisions in the TRIPS Agreement, which provide flexibility [for protecting public health and promoting access to medicines for all].” The Doha Declaration also extended the period for least developed countries to comply with TRIPS provisions on pharmaceuticals to 2016.
The Doha Declaration confirmed members’ rights to grant compulsory licenses for local manufacturing, but it left unresolved—possibly because of lack of domestic precedents—the conditions under which countries without pharmaceutical manufacturing capabilities would be allowed to import generic versions of patented drugs. Following two years of difficult negotiations, the United States, the European Union, Brazil, India, South Africa, and Kenya reached a compromise, which was accepted by the WTO General Council on August 30, 2003. As demanded by developing countries, the agreement covered all diseases, not just HIV/AIDS, tuberculosis, and malaria, and it applied to all countries, not just the “truly disadvantaged” (Bridges 2003). However, the August 30 Decision included so many requirements and conditions that activists warned it contained “enough bureaucratic red tape to discourage poor nations from importing the drugs” (Becker 2003).
Despite their perceived shortcomings, developing countries and AIDS activists considered the Doha Declaration and the August 30 Decision significant milestones in their struggle for affordable drugs. These texts were the outcome of developing countries’ accumulated experiences through imitation and reinvention, but they also contributed, as we will see, to subsequent diffusion of TRIPS flexibilities in developing and developed countries. Even the United States changed its position. On the one hand, the United States continued to impose constraining intellectual property rules on other countries through bilateral free trade agreements (Rossi 2006; Sell 2007) or when advising states how to operate their patent offices (Deere 2008; Drahos 2008). On the other hand, it no longer explicitly denied developing countries’ right to create access to affordable drugs, including by using flexibilities. In addition, the United States, like other wealthy countries, dramatically increased its level of foreign aid devoted to purchasing AIDS drugs (see Figure 3). Crucially, both the Global Fund to Fight AIDS, Tuberculosis, and Malaria, which was established in 2002, and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), which was launched in 2003, funded AIDS drugs, including generic versions of patented drugs. 19 By 2008, PEPFAR spent 57 percent of its procurement budget for ARVs on generic drugs (PEPFAR 2008). This tension shows that although the U.S. government may not have been an enthusiastic adherent of the new global norms, it was forced to revise its strategies to mostly abide by them. The ambiguous position of the United States, in turn, suggests that global norms may exist and be effective even when the most powerful state is a reluctant follower.
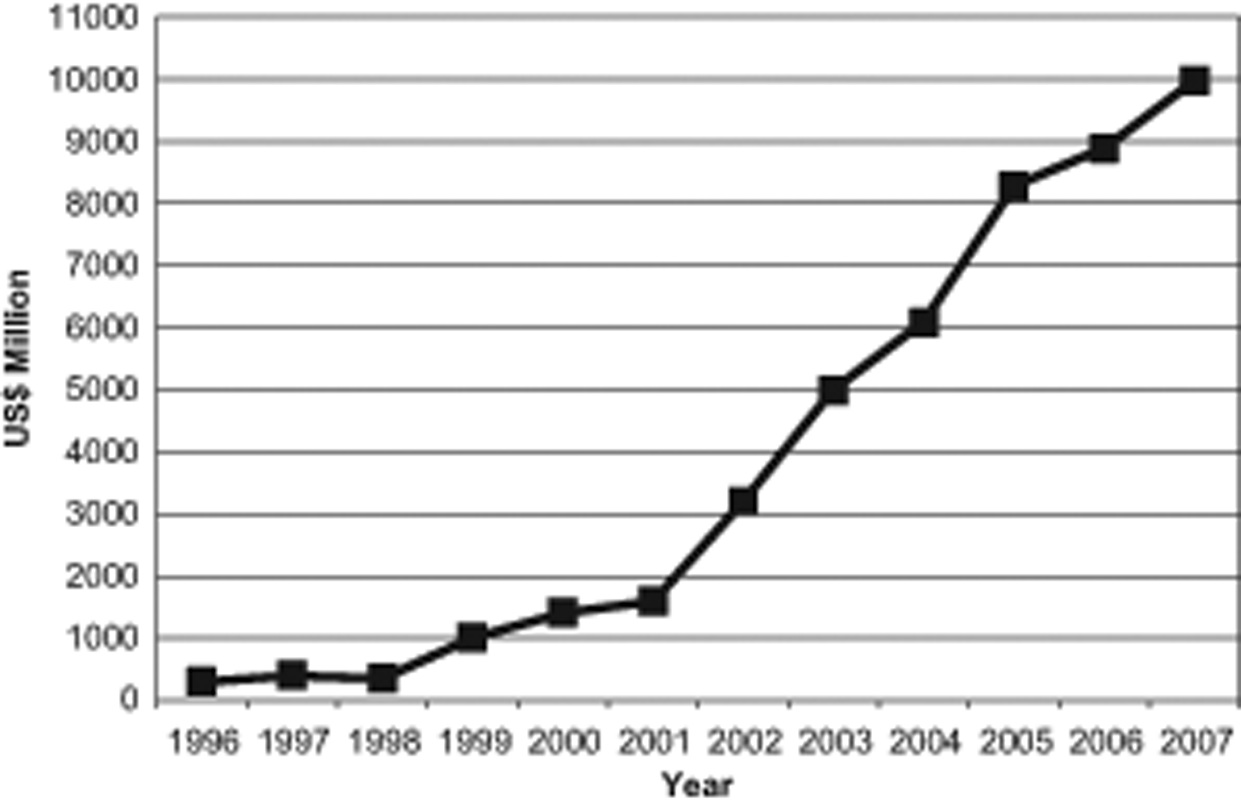
Estimated Total Annual Resources Available for AIDS, 1996 to 2007
Diffusion and Further Divergence of the Reinterpreted Global Rules
Following Doha, more poor countries took advantage of their right to use TRIPS flexibilities, but they still maintained local variations. By 2006, a WHO report found that “virtually all developing countries . . . provided for the grant of compulsory licenses. . . . The grounds upon which such licenses could be granted, however, varies considerably” (Musungu and Oh 2006:xvii). The review also found “an almost equal number of patent laws that incorporated specific provisions for parallel importation and those that did not” (Musungu and Oh 2006:48). Countries also utilized these laws. After adoption of the Doha Declaration, Zimbabwe was the first country to utilize its government use provisions to import, and then locally produce, generic ARVs. Mozambique, Zambia, Cameroon, and Indonesia issued compulsory licenses to local manufacturers. Malaysia, Eritrea, and Ghana relied on the August 30 Decision to issue compulsory licenses for the importation of generic HIV/AIDS medicines, mostly from India. 20
But countries did not merely implement existing rights. Through reactive diffusion, the scope of rights granted under the Doha Declaration continued to evolve and spread, with Thailand, Brazil, and India taking the lead. Thailand’s wide-scale provision of locally manufactured ARVs in 2003 was informed by a study visit to Brazil (Ford et al. 2007). In contrast to Brazil, however, Thailand chose to go beyond merely threatening the use of compulsory licensing. In October 2006, a month after Thailand’s armed forces overthrew Prime Minister Thaksin Shinawatra, the minister of public health announced a compulsory license for efavirenz. In another case, in January 2007, Thailand provocatively issued a compulsory license for Kaletra, a second-line treatment for AIDS. In a third case, further widening the spectrum of public-health issues considered severe enough to warrant overriding patents, Thailand invoked compulsory licensing for Plavix, a drug for heart disease (Bridges 2006). In this way, Thailand built on earlier successful challenges to broaden the scope of flexibilities. A Wall Street Journal (2007) editorial warned that other countries were likely to follow Thailand’s example. Indeed, with its threats of compulsory licensing losing their credibility, in May 2007 Brazil invoked compulsory licensing for efavirenz (Souza 2007).
A fourth flexibility for improving access to drugs was to challenge their patentability. In Brazil, a presidential decree issued in 1999 and converted into law in 2001 required prior consent from the Ministry of Health for any pharmaceutical patent application approved by the National Institute for Industrial Property. Between 2001 and July 2008, the Ministry rejected almost 30 percent of applications approved; in more than 40 percent of applications the Ministry did approve, the applicant first had to reduce the breadth of the patent’s claims (Shadlen 2009). In other countries, including Thailand, activists went to court to challenge patents’ legitimacy (Oxfam 2001).
The issue of patentability emerged with full force when India prepared to implement a third amendment to its Patent Act in 2005. The bill’s content was bitterly contested by generic drug manufacturers, who sought to maintain their right to export generic drugs, and advocates who argued that stronger patent protections would trigger investment and innovation in the country (Bellman 2005). The generic manufacturers’ position was strongly supported by international actors concerned with the impact of a stringent patent law in India on access to AIDS drugs elsewhere. Much was at stake because more than half the AIDS patients in the developing world relied on India’s generic drug industry (McNeil 2005). Indian lawmakers received letters from heads of Latin American and African countries, and from UNAIDS, the WHO, and many others, urging them not to adopt restrictions that were not required under the TRIPS Agreement (Subramanian 2005).
The Patent Act that eventually passed offered a narrower scope of flexibilities than what these international actors hoped for (Bridges 2005). But the Act did restrict the scope of patentability, explicitly stating that incremental innovations could not be patented without the applicant demonstrating that the modification yielded increased efficacy (Shadlen forthcoming). AIDS activists in India soon used the patentability provision to challenge various patent applications, including GlaxoSmithKline’s patent application for Combivir and Gilead Sciences’ patent application for Viread (tenofovir). When Novartis appealed a ruling denying a patent application by contending that the Patent Act was in breach of India’s obligation under TRIPS, the High Court ruled against the company (Bridges 2007). Brazil followed India’s example and in 2008 rejected Gilead’s patent request for Viread on grounds that it lacked technological inventiveness (Reuters 2008). The Indian newspaper Economic Times proudly reported that the patentability provision “is emerging as a global trendsetter” with many countries in the Asia-Pacific region, including the Philippines, Maldives, Pakistan, Sri Lanka, Vietnam, Indonesia, Malaysia, and Bangladesh, considering adopting the wording of the Indian law (Prasad 2007; see also Shadlen forthcoming).
In short, after Doha, governments of low- and middle-income countries continued to broaden the scope of TRIPS flexibilities by building on each other’s experiences. Through reactive diffusion, but also because of counter-strategies by Western governments and brand-name pharmaceutical companies, policies regarding access to AIDS drugs will no doubt continue to evolve, disseminate, and be challenged.
Discussion
Global norms regarding the appropriate balance between intellectual property protection and access to affordable AIDS drugs have gone through a number of significant transformations (see Table 3). Initially, low- and middle-income countries implemented TRIPS with minimal attention to the flexibilities permitted in the Agreement. However, after brand-name pharmaceutical companies failed to block a South African law that relied on TRIPS flexibilities, other countries adopted policies that built on South Africa’s interpretation of TRIPS but also deviated from it, offering their own policy innovations. To formalize their success, developing countries demanded that local variations be confirmed as legitimate by other WTO member states. The Doha Declaration and August 30 Decision were successfully disseminated in a large number of developing countries but again with local divergences.
This chain of events suggests that the new global norm regarding the acceptable balance between intellectual property rights and access to affordable AIDS drugs emerged out of a process in which alternative interpretations were first tested as local divergences. When successful, these divergences diffused to other countries that contributed their own variations. Eventually, the accumulation of these experiences turned them into a legitimate norm that competed with the original international obligation, making it possible for developing countries to prevail in the Doha negotiations. The stages leading to the Doha Declaration suggest that accumulated experiences are a likely condition for developing countries’ success in international negotiations. Later experimentations with what is allowed under the Declaration suggest that reactive diffusion may lead to the construction of new policies.
Accumulation of experiences due to reactive diffusion is not the only way that global norms develop or change, but it may be more common than what prior studies suggest. A strong coalition, a forceful moral argument, and the support of transnational activists are all important, but developing countries may be more likely to prevail in international negotiations if they have already assembled victories at the domestic level. Coordinated resistance at the international level is more likely, and more likely to succeed, after a change in a large number of domestic sites has already occurred. Additionally, the TRIPS case suggests that the more coercive the origins of international obligations are, the more likely that those international obligations will encounter processes of reinvention through reactive diffusion that may eventually transform them. It is here, also, that the difference between these processes and explicit resistance becomes apparent: divergences tend not to reject but to build on original obligations, clarifying through reinterpretation rather than subversion. These reinterpretations are not necessarily linear; some divergences may reduce rather than broaden the existing gap between the original model and emerging norm, as the Indian Patent Act of 2005 reveals. Finally, this case suggests that influential policy reinvention is not equally distributed among countries. This is partly because middle-income countries are more likely than low-income countries to have resources for innovation. But this is also because reinventions that emerge in peripheral countries are more likely to be ignored by others. The central role of South Africa, Brazil, and Thailand was due to material conditions that enabled them to innovate and to innovation that attracted attention and enabled imitation and additional innovation.
We should not expect all global laws and norms to experience a similar trajectory of policy reinvention through reactive diffusion. Not all global norms and laws provoke critical reaction similar to TRIPS. Critical reactions do not all translate into significant divergences. In addition, not all significant divergences meet strong objections from powerful actors such as the U.S. government or pharmaceutical companies. Finally, strong objections from powerful actors do not all meet effective opposition backed by forceful moral claims. But the exceptional elements of the case of intellectual property protection of AIDS drugs simply make it easier to identify processes that are also likely to be present in less extreme cases. World society scholars have shown that loose coupling is surprisingly common, and studies on diffusion have shown that cross-national influence occurs frequently. Reactive diffusion and resulting accumulation of experiences should also occur often. The arguments offered here should therefore be useful for revealing processes in other cases of successful deviations from an international model. For example, differences in neoliberal policies in the United Kingdom and the United States, on the one hand, and Germany and France, on the other, may result not only from local conditions (Prasad 2006) but also from different sources of influence (Robertson and Waltman 1993). The notion of reinvention through reactive diffusion may also be useful in analyzing policy outcomes in other settings, such as federal governments, where federal laws may reflect reactive diffusion of laws at the state level. In short, the study of accumulation of experiences due to reactive diffusion holds promise for analyses that situate local processes in a meta-local context, such as international organizations or federal governments, and treating the meta-local context to consist of inter-connected local processes. It is through these multilayered processes that policies are, at times, remade.
Footnotes
Acknowledgements
Earlier versions of this article were presented at the Society for the Advancement of Socio-Economics, the International Political Economy Society, the American Sociological Association, the University of Arizona, George Washington University, and Harvard Law School. I received particularly helpful comments from Greta Krippner, Ken Shadlen, Andrew Schrank, James Jasper, Victoria Johnson, Alexandra Kalev, Susan Sell, Dorit Geva, and Samantha MacBride. Special thanks for the ASR editors and anonymous reviewers whose comments and suggestions led to the substantial improvement of the manuscript.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.