
Abstract
Journalistic accounts of the opioid crisis often paint prescription opioids as the instrument of profit-minded pharmaceutical companies who enlisted pain specialists to overprescribe addictive drugs. Broadening beyond a focus on pharmaceutical power, this article offers a comparative-historical explanation, rooted in inter- and intra-professional dynamics, of the global increase in rates of opioid prescribing. Through archival analysis and in-depth interviews with pain specialists and public-health officials in the United States and France, I explain how and why opioids emerged as the “right tool for the job” of pain relief in the 1980s and 1990s, affecting how pain science is produced, pain management is administered, and a right to pain relief is promised in different national contexts. I argue that opioids, selected and destigmatized as the technology for pain relief, helped establish a global network of pain expertise, linking a fledgling field of pain specialists to the resources of global-health governance, public-health administration, humanitarian organizations, and pharmaceutical companies. I then compare how U.S. and French pain specialists leveraged opioids to strengthen the boundaries of their emergent fields. Pain specialists’ differing degrees of autonomy in each country’s network of pain expertise shaped the extent to which opioids could dominate pain management and lead to crisis. Tracing the relationship between opioids and pain expertise, I show how technologies can drive crises of expert credibility if and when they escape the control of the networked fields that selected them.
Since the early 2000s, the prescription opioid crisis has generated significant social suffering and public controversy. Between 1991 and 2013, global consumption of opioid analgesics increased by 618 percent, driven largely by North America and Europe (International Narcotics Control Board 2015:14). In 2017, 10.5 million U.S. residents were estimated to have misused prescription pain relievers (Substance Abuse and Mental Health Services Administration 2018). To explain these statistics, people typically turn to the familiar story of profit-driven pharmaceutical companies who enlisted doctors to overprescribe opioids to patients in pain (Hoffman 2019; Keefe 2017; Khazan 2020; Macy 2018; Meier 2003, 2018). However, prevailing journalistic accounts of the opioid crisis overlook the global, historical, and inter-institutional processes by which government officials, humanitarian actors, and medical experts promoted opioids for pain relief as a public-health priority and patient right.
In this article, I offer a historical and empirical account, rooted in inter- and intra-professional dynamics, for the global increase in rates of opioid prescribing from the late 1980s through the mid-2000s. Opioid manufacturers, most notably Purdue Pharma, knowingly downplayed the addictive potential of opioids from the mid-1990s to as late as 2017. Providing doctors with incentives to act as “opinion leaders” who touted the safety and efficacy of extended release opioids, pharmaceutical companies stoked the over-prescription of highly addictive drugs (Armstrong 2019; Bogdanich and Forsythe 2020). However, the actions of multinational pharmaceutical companies during the late 1990s cannot alone explain how and why opioids won out as the solution to manage pain. The pharmaceutical industry served as a necessary but insufficient driver of this process.
From the late 1980s onward, I trace the formation of a global pain-management network responsible for the development of opioid-centric pain-management policies at the World Health Organization and across two leading national contexts in the “fight against pain”: the United States and France. Drawing on theories of expertise, networks, fields, and technologies (Camic 2013; Clarke and Fujimura 2014; Eyal 2013b; Eyal and Buchholz 2010; Krause 2018, 2018; Medvetz 2012; Panofsky 2011), I approach pain expertise as a network, composed of multiple professional fields and technologies (Eyal 2013a), to explain why several fields selected opioids as the “right tool for the job” of pain relief (Clarke and Fujimura 2014). I then identify how, despite a shared initial commitment to opioids, French and U.S. pain-specialist fields managed their strategic relationships to opioid technologies differently, insulating France from a prescription opioid crisis among pain patients.
My analysis rests on science and technology studies that analyze why social actors select certain technologies as the right innovation to solve a problem (Casper and Clarke 1998; Clarke and Fujimura 2014; Pinch and Bijker 1984) and assert, via Actor Network Theory, that technologies themselves shape how science and expertise are produced and legitimated (Fujimura 1988; Latour and Woolgar 1986). A “linking” technology, opioids brought together pain specialists, public-health officials, hospital administrators, humanitarian organizations, and the pharmaceutical industry to exchange material resources, moral credibility, and scientific legitimacy across field boundaries (Krause 2018).
Selected as “the right tool for the job,” opioids have operated as both resources and actants in the emergent inter-field network of pain expertise. Aiming to demarcate the boundaries of their nascent professional field, pain specialists endorsed opioids as resources to attract capital and recognition from other fields. Standardizable, easily delivered, and relatively cheap, opioids matched the needs of healthcare systems in the Global North seeking to efficiently address a growing pain problem. Opioids’ material and symbolic value drove how pain specialists and health policymakers constructed new clinical practices and rights to pain relief. Linking fields together, opioids, as actants, organized the network of pain expertise, shaping what knowledge about pain management was produced and implemented. Opioids’ addictive properties then proved uncontrollable. Opioids destabilized the global network, discredited pain specialists, and cast doubt on the viability of the right to pain relief.
The opioid crisis is often portrayed as a uniquely American problem, but ballooning rates of opioid prescribing have been a transnational process with global implications for pain management and patient rights. Big pharma’s lobbyists intervene in health policy in most developed countries, and the power of pharmaceutical interests is not a strictly U.S. phenomenon (Lakoff 2005; Petryna, Lakoff, and Kleinman 2006). Comparing the history of French and U.S. approaches to pain management reveals that pharmaceutical actors encouraged the selection of opioids as the technology of pain management in both countries. In the United States and France, prescription-opioid consumption increased markedly over the past two decades, but France’s prescription opioid problem remains at a smaller scale than that of the United States (Hider-Mlynarz, Cavalié, and Maison 2018; Monzon and Richard 2019). Pharmaceutical power, alone, cannot explain why the United States outpaced France in prescribing opioids for pain. I argue that this difference in magnitude can be attributed to how pain specialists worked with politicians, public-health officials, and hospital administrators to implement opioid-centric expertise. Pain specialists in each country navigated challenges to their field by leveraging opioids as links to other powerful fields. French and U.S. pain specialists’ differing ability to maintain their field’s autonomy in the broader network of pain expertise shaped opioids’ capacity to dominate pain management and lead to crisis.
The United States and France are ideal national cases for this analysis because (1) they were leading national consumers of prescription opioids per capita throughout the early 2000s (when the U.S. opioid crisis began to take hold), and (2) French and U.S. pain specialists successfully harnessed political interest in pain, framing pain as a public-health crisis in the late 1980s, earlier than most countries in the Global North (International Narcotics Control Board 2002). Both countries’ pain-management policies prioritized the use of opioids to promise patients a “right to pain relief.” From these shared points of departure, I compare how opioids, as linking technologies, structured each country’s interprofessional “fight against pain,” leading to different outcomes for opioid prescribing patterns, the availability of non-pharmacological treatments, and the survival of the pain-specialist field.
This article demonstrates how technologies shape the “co-production” of expertise (Jasanoff 2010). Linking technologies facilitate an exchange of resources across the fields that make up networks of knowledge production. As such, they are a mechanism of stability and crisis both for the network and its composite fields. When diverse fields of scientists, practitioners, manufacturers, activists, and policymakers come together to select one technology as the “right tool for the job,” that technology’s material properties and changing symbolic value limit how actors in the network define the problem and its solutions. Tracing the relationship between opioids and pain expertise, I show that linking technologies, like opioids, edge out other more flexible, resilient, and adaptive solutions to pressing problems. In this way, technologies can lead to crises of expert credibility if and when they escape the control of the networked fields that selected them.
Opioids and the Field of Pain Specialists
Sociological accounts of pain management’s professionalization as a medical subspecialty note that pain specialists founded their field through the establishment of multi-modal pain clinics and advances in pain science like the gate control theory of pain, the discovery of opioid receptors, and attempts to classify different types of pain (Baszanger 1998; Meldrum 2005; Whelan 2009). Since the 1970s, pain specialists have agreed that a multi-modal approach to pain management, which resists an overreliance on pharmacological solutions to pain, is the gold standard, particularly for chronic pain (Baszanger 1998). However, opioid-centric approaches to pain now dominate globally, resulting in competing models of pain management: multi-modal treatment in interdisciplinary pain clinics versus the narrow use of pharmacological treatments, in particular, opioids. Sociological research has not yet examined why opioids emerged as the dominant technology of pain management, despite the pain-specialist field’s initial evidence-based preference for multi-modal (not strictly pharmacological) approaches.
Pharmaceutical interests cannot explain why opioids appealed to pain-management stakeholders in the 1980s, well before Purdue’s infamous OxyContin entered the market in 1995. Nor can pharmaceutical power capture why pain specialists in the United States and France gambled on opioids in a bid to strengthen the boundaries of their young subspecialty field. At the beginning of the 1980s, opioids were highly stigmatized, associated with a sinister history of misuse in the nineteenth century and contemporary criminality and addiction. Pain specialists’ decision to destigmatize opioids was a high-stakes endeavor. It sparked internal field struggles in the United States and France, yielding to a consensus that stigmatized opioids could valuably supplement more orthodox multi-modal approaches to managing chronic pain.
How did opioids shift from being a heterodox to orthodox technology for pain specialists in the United States and France? I argue that opioids offered material and symbolic incentives to pain specialists looking to solidify their field’s boundaries, autonomy, and legitimacy within the medical profession. Political opportunities and professional concerns, in addition to the resources provided by pharmaceutical companies, convinced skeptical pain specialists in France and the United States to back opioids. Pain specialists have consistently struggled for jurisdiction over questions of pain management (Baszanger 1998; Chiarello 2018; Petit 2014). The low prestige of pain management relative to other medical specialties, and the long-held belief among the broader medical community that pain is simply a symptom of disease, not a disease in itself, had, for the first few decades of pain management’s professionalization (the 1960s to mid-1980s), left its entrepreneurs fighting for legitimacy (Baszanger 1998; Wailoo 2014; Whelan 2009). Importantly, my findings show that pain specialists were not bought by pharma. Rather, pain specialists endorsed opioids in an attempt to solidify their field’s autonomy in the medical profession.
Opioids initially boosted pain specialists’ legitimacy and resources for three reasons. First, pain specialists successfully framed their knowledge and the practice of pain management as fundamental to the delivery of a new, achievable right to pain relief. Second, the framing of opioids as the technology for pain management promised public-health and pharmaceutical funding for otherwise difficult to finance pain research and advocacy. Third, prescription opioids, as easily standardized and implementable technologies, appealed to healthcare systems eager to develop efficient means to approach complex, chronic health problems, like chronic pain and cancer.
As highly addictive actants, prescription opioids have propelled a global addiction and overdose crisis, introducing new threats to the international pain-specialist field’s hard-earned gains toward credibility. Chiarello (2018) demonstrates that the success of the “pain management movement” in U.S. medicine contributed to the opioid epidemic, which in turn, pressured public-health and criminal-justice fields to curb the “spillover effects” of the unfolding crisis by encroaching on the autonomy of healthcare professionals, and pain specialists, in particular. However, in countries outside the United States, pain specialists have not suffered a comparable professional fallout. In France, national statistics indicate a smaller, by U.S. standards, but worrying increase in prescription opioid overdoses (Hider-Mlynarz et al. 2018). Yet, French pain specialists have faced less public backlash over prescription opioid-related deaths than their U.S. counterparts. Prescribing patterns and partnerships with pharmaceutical companies are increasingly scrutinized, but the French pain-specialist field has not lost its autonomy or credibility.
By tracing how opioids became the organizing technology of global pain expertise, I show that when technologies form the basis of relationships between fields, the broader network of expertise becomes vulnerable to changes initiated by the linking technology’s material properties and fluctuating symbolic value. As a resource, opioids beneficially linked pain specialists to other fields in a network of pain expertise. As an actant, opioids then shaped how that network produced pain science and policy to meet the demands of public-health politics, healthcare delivery systems, and pain-patient advocates. Inter-field relationships between pain specialists, public-health officials, politicians, humanitarian advocates, and pharmaceutical companies structured how the network of pain expertise implemented, and then variably contained, opioids as the tool for pain management in the United States and France.
Literature Review
Opioids and the Biomedicalization of Suffering
Throughout the twentieth and twenty-first centuries, industrialized countries have witnessed a clear rise in rates of reported chronic pain (Zajacova, Grol-Prokopczyk, and Zimmer 2021; Zimmer and Zajacova 2020; Zimmer, Zajacova, and Grol-Prokopczyk 2020). Facing increased demand for effective pain management, governments, medical professionals, and international health organizations have struggled to address the pain problem. Sociologists have described how contemporary institutions medicalize pain and suffering (Baszanger 1998; Fassin 2012; Illouz 2008; Rose 1999; Shilling 2014). However, even as medicine recognizes suffering as under its professional purview, clinicians often lack the tools and resources to effectively diagnose and treat pain, particularly as they try to avoid the potential dangers posed by addictive analgesics, like opioids, and interventional surgeries with high failure rates (Crowley-Matoka 2020; Crowley-Matoka and True 2012; Rubin et al. 2018).
Sociological work on the entanglements of chronic pain and prescription opioid misuse reveals that public-health policies and medical practices meant to address the undertreatment of pain often rely on opioid analgesics as an imperfect solution (Chiarello 2018; Rubin et al. 2018). The use of opiates to administer pain relief is not new. For centuries, societies across the globe have turned to opiates (Miller 2015; Schalick 2003), and the contemporary opioid crisis is not the first opiate panic (Musto 1999; Reinarman 1994). However, use of opiates for pain management was stigmatized, and even illegal, in many countries through the 1980s (Meldrum 2016). In the 1980s, with increasing numbers of people suffering from cancer and HIV/AIDS, vociferous debates around physician-assisted-suicide, and aging populations in the Global North, opioids reemerged as a potentially attractive solution to the pain problem.
Politicians, clinicians, and patient advocates began to frame untreated pain as morally reprehensible. In her work on the birth of pain management in the United States and France, Baszanger (1998:121) finds that in the 1970s and 1980s, early French pain physicians were “motivated by the ‘scandal’ of pain,” highlighting the presence of moral frames in pain specialists’ constructions of their work and professional identity. Research in communications studies charts how the U.S. market for prescription opioid analgesics grew alongside demand for patient rights to pain relief (Sherman 2017). By encouraging governments to recognize undertreated pain as a public-health crisis, pain specialists sought recognition that their specialized expertise was valuable to humanitarian efforts to improve the human condition.
The reframing of pain relief as a humanitarian issue echoes Fassin’s (2012:1) argument that throughout the 1980s and 1990s, public officials in the Global North perceived the alleviation of suffering as an obligation of governance—part of an emergent “humanitarian reason,” which encourages the “deployment of moral sentiments in contemporary politics” to “manage, regulate and support the existence of human beings.” This shift to humanitarian reason coincided with a flurry of human rights declarations that updated the post-World War II United Nations’ human rights framework, recognizing diverse objectives such as health, freedom from gender-based violence, and a clean environment. The recognition of new health-based human rights justified innovative governance strategies meant to reduce suffering, often producing complex and unintended consequences for how new human rights are implemented and claimed (Krause 2014; Merry 2011; Sherman 2017; Ticktin 2011).
This article contributes to scholarship on the biomedicalization of suffering and the unintended consequences of humanitarian health projects by analyzing how opioid-centric pain expertise has been “co-produced” by scientists, medical professionals, patients, pharmaceutical executives, politicians, and public-health actors looking to alleviate suffering (Jasanoff 2010). Appealing to a humanitarian agenda, the field of pain specialists amassed moral and technical credibility through the project to implement a new “right to pain relief.” Importantly, this project developed around the promise of prescription opioids even when pain specialists agreed that multidisciplinary approaches, which did not rely singularly on pharmaceuticals, were ideal for pain management.
Sociologists have observed that material objects can accrue moral and economic worth affecting how actors make decisions about the value of their health, possessions, finances, and the natural environment (Barnard 2016; Degenshein 2017; Fourcade 2011; Livne 2014; Zelizer 2010). “Humanitarian technologies” define, standardize, and commensurate what counts as sexual violence (Morse 2014), and end-of-life palliative care moralizes scarcity of material medical interventions (Livne 2014). These examples reveal the entanglements of technologies with moral projects, yet sociologists of science, technology, and knowledge have yet to analyze how and why expert actors imbue technologies with symbolic value to justify that a certain technology is “the right tool for the job.”
How did opioids win out as the technology to deliver pain management on the global scale, and what was the role of the pharmaceutical industry in this process? In the next section, I contend that turning to theories of fields, technologies, and expertise reveals why opioids appealed to a specific assemblage of actors, who destigmatized opioids to form a global network of pain-management expertise. This network co-produced opioid-centric pain research, clinical guidelines, public-health initiatives, and the promise of a human right to pain relief. The pharmaceutical industry, while a necessary component of this network, did not alone drive the global embrace of opioids as the right tool for pain management. Actors in public-health, political, humanitarian, and pain-specialist fields selected opioids as a technology, because opioids met their diverse needs in solving the pain problem. I then explain why, when opioids proved to be a difficult to control and addictive actant, the global network of pain expertise and the national fields of pain specialists embedded within it, experienced varying degrees of crisis.
Technologies and Fields in Networks of Expertise
Classic work in the sociology of knowledge establishes that intra-professional dynamics affect how medical expertise is created, legitimated, and put into practice (Abbott 1988; Freidson 1988). However, recent applications of field theory to the sociology of knowledge identify the space between fields as an important site of knowledge production (Camic 2013; Eyal 2013b; Hess and Frickel 2014; Medvetz 2012; Panofsky 2011). Scholars variably call this interprofessional space an “interstitial field” (Medvetz 2012), “network” (Callon 1986; Cambrosio, Limoges, and Hoffman 1992; Eyal 2013a), “archipelago” (Panofsky 2014), “interface” (Fujimura 1988), or “multiplex” (Camic 2013:195). To explain how certain forms of expertise gain and lose power, fields-based approaches highlight the relational nature of knowledge to multiple fields and track the transfer of material and symbolic capital across field boundaries (Camic 2013; Eyal 2013a, 2013b; Eyal and Buchholz 2010; Fourcade and Khurana 2013; Gorski 2013a, 2013b; Krause 2014, 2018; Panofsky 2011).
I use Eyal’s (2013a, 2013b) “network of expertise” to refer to the inter-field space of knowledge production. Reconciling elements of Actor Network Theory with theories of fields, Eyal’s (2013a:871) network enables sociologists to analyze how multiple fields of actors and material “tools and devices” affect how expertise is produced, broadening traditional professions-based approaches that only “focus on the actors and their skills.” In this network, knowledge production spans the “jurisdictional boundaries” of established professional fields (Abbott 1988), and fields in the network can be bridged by socio-material links, like technologies (Eyal 2013b; Krause 2018). I draw on this concept of the network to establish how networks of expertise cohere and destabilize around linking technologies, which affect inter- and intra-field dynamics.
When referring to the component fields of the inter-field network, I denote a meso-level “configuration of objective relations between positions” (Wacquant and Bourdieu 1992:97). Fields are “socially constructed arenas within which actors with varying resource endowments vie for advantage” (Fligstein and McAdam 2011:3). Positions in a field can be occupied by individuals or institutions, and these positions are hierarchical, meaning different positions wield varying levels of capital within the field. Actors within the field are oriented toward field-specific forms of capital and shared nomos or “modalities of activities” (Bourdieu 1996; Eyal 2013b:161). Fields can be characterized by their degree of “autonomy”: the capacity of the field to organize internally (without undue external influence from other fields) around shared core principles, norms, field-specific capital, and practices (Bourdieu 1996; Krause 2018).
Pain specialists (pain-management clinicians and researchers) comprise an important professional field within the inter-field network of pain expertise; they recognize a shared objective to improve patient access to and efficacy of pain relief. Elites in the field include leaders of pain expert societies, founders of pain centers and pain education programs in medical schools, and principal investigators of major pain research initiatives. Pain specialists accrue field-specific capital by demonstrating a commitment to establishing pain management as a standalone medical specialty, which, although multidisciplinary by design, is independent from other established medical specialties and areas of research that approach pain as a symptom or comorbidity rather than a disease in itself. Pain specialists continue to fight for professional autonomy and formal recognition as a clinical specialty in the United States and France. In the United States, doctors can choose to pursue additional certification in pain as a subspecialty, after completing a residency in anesthesiology, emergency medicine, family medicine, physical medicine, neurology, or radiology. In France, pain is recognized by the French National Academy of Medicine as a cross-disciplinary sub-specialization. In both the United States and France, pain expert societies and select research hospitals with pain-management clinics are the loci of professional training and certification.
The field of pain specialists differs from other fields in the network of pain expertise because those auxiliary fields’ boundaries and internal field dynamics are not primarily oriented toward pain relief. These fields belong to the broader network of pain expertise, but they do not necessarily share a professional commitment to pain, nor are these fields’ autonomy and boundaries as dependent on the credibility of pain expertise. Other fields comprising the network of pain-management expertise include global-health governance, the global pharmaceutical industry, national public-health administration, healthcare reimbursement, patient advocacy, and policymakers (see Figure 1). Throughout the article, I use the term “resources” when referring to the material and symbolic capital that fields exchange across the network.
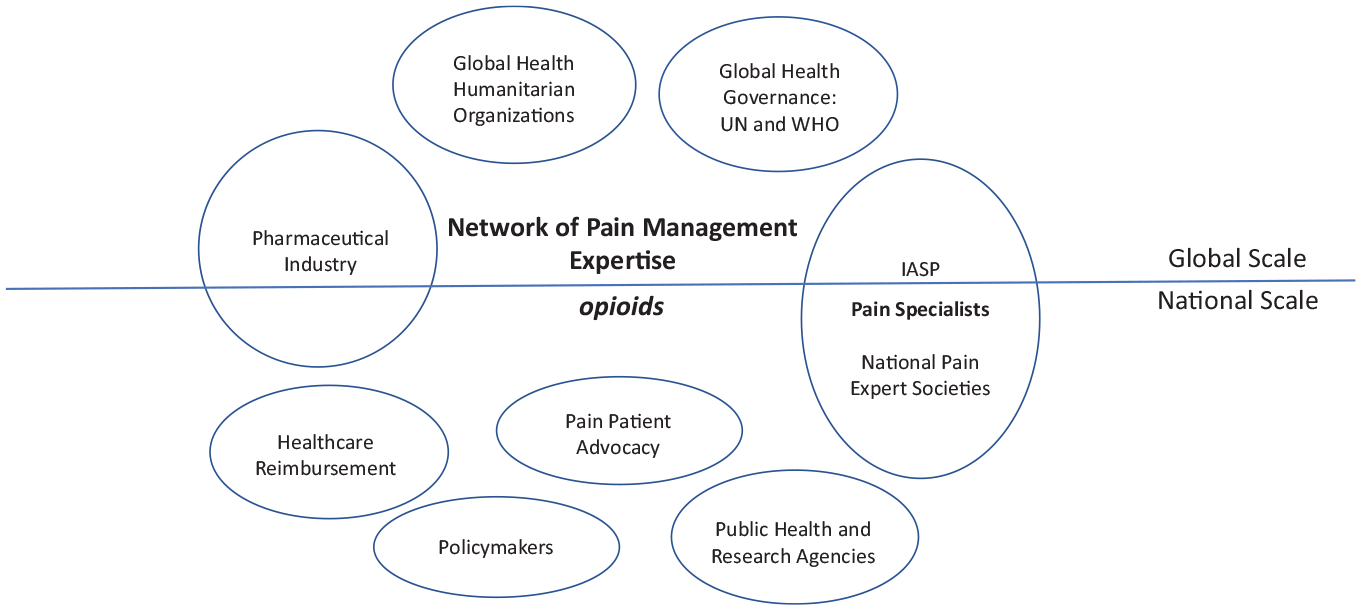
Network of Pain Management Expertise
Recent work has interrogated the dynamism of within-field processes, charting how fields emerge, change, destabilize, and serve as valuable conceptual tools in historical analysis (Dromi 2016; Fligstein 2013; Gorski 2013a; Steinmetz 2017). To grasp the relationships between fields in an inter-field network of expertise over time, one must understand how the composite fields are linked and what these links do to catalyze changes within fields and across the network. Krause (2018:10) argues that these links between fields can and should be analyzed “with attention to [the] socio-material aspects of these links . . . we can examine in some detail the technologies and devices that are doing the linking and their history and implications.”
If technologies act as a socio-material link connecting fields and shaping inter-field dynamics (Baker 2017; Benson 2005; Benson et al. 2012; Chiarello 2021; Dominguez Rubio and Silva 2013; Krause 2014, 2018), how and why are they selected? How do changes to a technology’s symbolic and material value affect the fields it links together in a network of expertise? Sociologists of knowledge demonstrate that actors within fields can leverage the transfer of material and symbolic resources across fields to strengthen the boundary of their own field (Camic 2013; Eyal 2013b; Gorski 2013a, 2013b). Technologies can facilitate this transfer. As links, they shape how fields demarcate their boundaries while working together to produce expertise. Thus, the composite fields of an inter-field network can both derive and lose autonomy by selecting technologies that connect them to other fields in the network. Endorsing a technology as the “right tool for the job” attracts capital and recognition for fields seeking to position themselves as credible experts. In this sense, fields in networks of expertise select technologies as resources. However, once the technology has been selected, it begins to operate as an actant in the network, shaping how and what expertise is produced.
Pain specialists destigmatized opioids to access and exchange symbolic and material resources with other fields interested in improving the delivery of pain management. However, by organizing around opioids as the technology of pain expertise, the field of pain specialists opened itself to the risk of crisis when opioids, as unmanageable actants, fueled an epidemic. Comparing outcomes in France and the United States shows that how fields are able to manage linking technologies is an overlooked mechanism of expert credibility, affecting how knowledge is produced, professional autonomy is maintained, and rights are delivered.
Data and Methods
This article combines findings from qualitative analysis of primary historical documents, secondary historical sources, legislative and public-health archives in the United States and France, and 50 in-depth, semi-structured interviews conducted with pain-management professionals, advocates, and public-health officials in the United States and France. The primary historical texts analyzed include transcripts of U.S. congressional and French parliamentary debates (1988 to 2017); U.S. and French public-health institutions’ archival materials, legislative archives, and newspaper coverage of pain-management issues (1988 to 2018); and publications of the World Health Organization (WHO) and the International Association for the Study of Pain (IASP). I also consulted and cite secondary sources on the history of U.S. and French pain management, the IASP, and the birth of the WHO’s cancer pain initiatives.
I operationalize the pain-specialist field as composed of researchers and clinicians who explicitly orient their professional identity and practices toward policy, research, and the practice of pain management. Actors in this field typically belong to international and national societies of pain expertise, such as the IASP, the American Academy of Pain Medicine (AAPM), and the French Society for the Study and Treatment of Pain (SFETD). Thus, the professional pain-specialist field spans global and national scales. I identified seven additional fields contributing to the network of pain expertise: the pharmaceutical industry, global-health governance, global-health humanitarian organizations, patient advocacy, public health, healthcare reimbursement, and the political field of policymakers. I focus on the field effects for pain specialists within the broader inter-field network of pain expertise. However, each field in the network experienced challenges stemming from the re-stigmatization of opioid technologies in the wake of the opioid epidemic.
France and the United States are ideal comparative cases for this analysis. U.S. and French pain specialists and public-health officials were at the forefront of international health organizations’ discussions about establishing pain relief as a right. In both countries, doctors and researchers with an interest in pain medicine attempted to establish pain management as a medical subspecialty throughout the 1970s and 1980s (earlier than most other countries in the Global North) (Baszanger 1998). Legislation promising resources to promote adequate pain relief, especially for patients with terminal illness, found support across party lines in both countries in the 1990s. The two countries’ healthcare systems are certainly different, but the ways pain specialists enlisted political support for their projects by destigmatizing opioids share notable similarities. In 2000, the United States and France were the top two national utilizers of morphine and thebaine (a material necessary for the manufacture of oxycodone and codeine) (International Narcotics Control Board 2002). Today, however, the United States and France differ in the magnitude of their prescription opioid crises. Furthermore, the U.S. pain-specialist field has all but collapsed in the wake of the opioid crisis, whereas the French pain-specialist field has maintained its autonomy and credibility.
Interviews were conducted between 2016 and 2018 in France and the United States. I identified key contemporary actors engaged in public-health debates around pain management. In France, I interviewed 16 pain-management clinical researchers and practitioners who were also active in efforts to reform public-health policy, training standards, and reimbursement schedules around pain management. Many of these pain-management experts were also involved in the French national chapter of the IASP. I interviewed four pain-patient advocates and five public-health and social-services administrators who worked on pain-management issues. Most of the interviews in France were conducted in French or a mix of French and English based on the preference of the interviewee. In the United States, I interviewed 19 pain-management researchers and clinical practitioners and six pain-patient advocates and lobbyists. Several of those interviewed had been involved in interagency efforts between the National Institutes of Health, the Department of Health and Human Services, the National Institute on Drug Abuse, the Agency for Healthcare Research and Quality, and the Centers for Disease Control to provide expert testimony in the development of pain-management research initiatives and clinical guidelines.
I asked French and U.S. interviewees about their perceptions of the history of pain management as a subspecialty in their respective countries, pain-management standards, and best practices in the wake of the opioid crisis, and whether they believed pain relief should be promised as a right. I asked respondents who practiced during the 1980s and 1990s to recall their work enlisting political and pharmaceutical support for pain-management initiatives, research, and advocacy. In my analysis of interview transcripts, I triangulated participants’ recollections of the history of pain-management debates and policies with archival materials, media coverage, and secondary historical sources. Finally, I asked all participants about their contemporary attitudes toward the use of opioids in pain management.
Through inductive analysis of media reports, documents, historical accounts, and interview transcripts, I traced the role of opioid technologies in the emergence of a global network of pain-management expertise. In international health organization publications and French and U.S. archival materials, the justification for supporting the development of the pain-specialist professional field was often framed in humanitarian terms: all people deserve relief from pain. However, this idea was nearly always discussed in terms of access to prescription analgesics, specifically morphine or other opioids. I used ATLAS.ti software to code my data for mentions of the role of opioids in the production of pain-management expertise, inter-institutional partnerships between pain specialists and other fields, and the construction of pain relief as a right. I thus tracked how a global network of pain expertise grew around a commitment to increasing prescription opioid availability and creating standards for opioid-centered therapies. I analyzed how that global network extended into the United States and France. I then coded how pain specialists in each country responded to the opioid crisis and described the current state of pain expertise.
Findings
The Emergence of a Global Network: Opioids and a Right to Pain Relief
Pain management as a medical subspecialty originated in the United States in the 1950s, largely due to the work of Dr. John Bonica, a U.S. anesthesiologist who Time Magazine dubbed “Pain Relief’s Founding Father” (Thompson 1984). From its inception, the pain specialty has engaged in a struggle for credibility among the wider medical community, as doctors have traditionally approached pain as a symptom rather than a disease in itself (Baszanger 1998; Chiarello 2018; Whelan 2009). The gate control theory of pain, proposed by psychologist Ronald Melzack and neuroscientist Patrick Wall in 1965, enabled an international field of pain specialists to organize around a common scientific theory of pain perception to inform and legitimate pain management as a clinical subspecialty (Baszanger 1998). This set of shared principles bolstered the incipient pain-specialist field’s professional autonomy. However, the emergence and survival of an international field of pain specialists could not rely on breakthroughs in pain science alone. Pain specialists needed to enroll political support, biomedical industry funding, and the cooperation of national public-health administrators to secure their recognition by hospital systems, insurers, medical schools, and research funders.
Bonica was at the center of this professional project to expand institutional support for the pain specialty in countries across the globe. He founded the International Association for the Study of Pain (IASP) in 1974, eliciting financial support from the National Institutes of Health, other U.S. national medical institutes, and “several pharmaceutical and medical equipment companies” (Jones 2010:2). Most of the Association’s first financial backers were based in the United States, but the multinational pharmaceutical and medical equipment companies had global reach. By 1975, the IASP had facilitated the establishment of 14 regional pain expert chapters across the United States, Argentina, Canada, France, Germany, Belgium, the Netherlands, Japan, Scandinavia, Italy, and the United Kingdom (Jones 2010:11). Acting as a hub of international pain expertise, Bonica and the IASP called for the development of national pain-management policies.
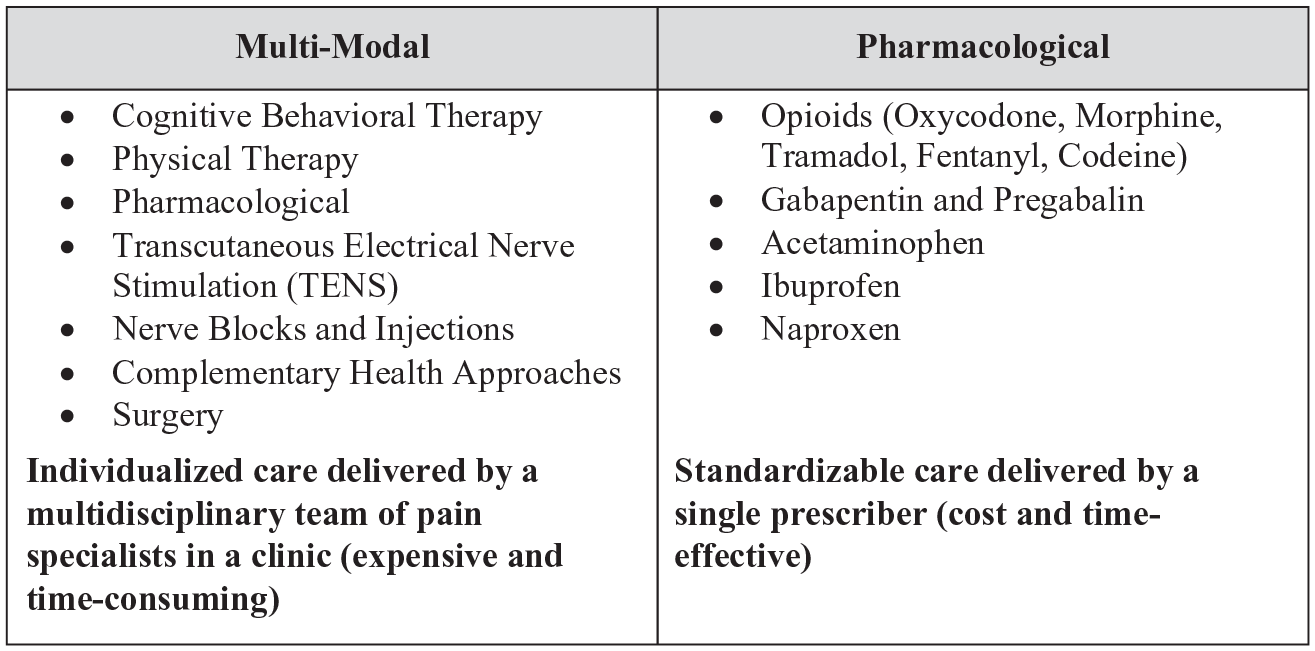
From the start of their international initiatives, Bonica and the IASP’s vision for pain management followed the tenets of the gate control theory of pain. Gate control theory conceptualizes pain perception as a physiological and psychological process. Importantly, this holistic definition invites a multi-modal treatment approach. Pain specialists argue that pain management should be an interdisciplinary endeavor, housed in specialized clinics, staffed by doctors trained in a variety of specialties that integrate interventional, pharmacological, non-pharmacological, and psychological approaches (see Figure 2). Contemporary research on pain management continues to recognize this model, which does not rely solely on pharmaceuticals for relief, as the most effective in treating chronic pain. Opioids are a tool in pain management’s toolkit, but from the start, pain specialists accepted they were not a silver bullet, and multi-modal approaches were preferable.
Multi-Modal versus Pharmacological Approaches to Pain
In the language of fields, early actors in the pain-specialist field recognized the multi-modal clinic approach to pain management as orthodox. Pain specialists agreed that opioids were risky and suited only to specific contexts (primarily palliative care). Thus, at the early stages of the pain-specialist field’s formation, opioids were heterodox. They carried cultural stigma, and their medical use was highly regulated, if not prohibited, throughout the 1970s.
Surprisingly, despite the orthodoxy of non-pharmacological therapies within the young field of pain specialists, the first major global-health initiatives around pain management focused on destigmatizing and increasing opioid prescribing, specifically for cancer pain. The WHO’s Cancer Unit led the first global pain initiative in 1982. The WHO working group, which included Bonica and other luminaries in the emerging fields of pain and palliative care, identified a significant lack of knowledge around pain management and the utilization of opioids among cancer specialists across the world (Meldrum 2005). They agreed to develop guidelines, recognizing the need to “reframe the use of opioids as a therapeutic skill based on pharmacologic knowledge, rather than a risky practice inevitably leading to drug dependence” (Meldrum 2005:42). This project provided pain specialists the opportunity to link up with the powerful field of global-health governance and assert their professional jurisdiction over the specialized “therapeutic skill” necessary to safely treat cancer pain with opioids.
Given anxieties around opioid dependence, the interprofessional WHO working group recognized the power of expert-backed standards to change medical and legal attitudes around opioid prescribing for pain management (Meldrum 2005:45). They thus created an easy-to-use tool that would destigmatize the use of opioids in clinical practice and promote pain relief as a humanitarian global-health goal. The result was the opioid-oriented “cancer pain ladder,” a three-tier classification system that ranks analgesics starting with Step 1: non-opioid analgesics, such as paracetamol and ibuprofen, characterized by their low risk of misuse, dependence, addiction, and overdose. If pain persists, the ladder recommends Step 2: weak opioids like codeine and tramadol. Finally, if moderate to intense pain persists, medical professionals should move to Step 3: strong opioids, such as oxycodone, morphine, and fentanyl (WHO 1986). The ladder is easy to understand and implement in a variety of clinical encounters. It framed opioids as valuable tools to ensure adequate pain management. However, opioids’ negative reputation continued to challenge pain and cancer specialists, who recognized that the major obstacle to the pain ladder’s use was opioids’ differing availability in different countries and the stigma surrounding opioids that prevented doctors from prescribing them (Cousins, Brennan, and Carr 2004).
Due to this stigma and reluctance to encourage the global spread of morphine, it took another two years for the WHO Publications Office to release the pain ladder recommendations (Meldrum 2005:51). The WHO published the recommendations in 1987, and “with the assistance of national departments of health and pharmaceutical companies, the small handbook was translated into 15 languages and distributed around the globe . . . quickly becoming a ‘bestseller’” (Meldrum 2005:51). The ladder was a success. Adopted by medical schools and public-health agencies, it destigmatized opioids and legitimized the idea that pain relief was a safe and reasonable goal in the care of cancer patients. Over the next two decades, national public-health agencies increasingly adopted the cancer pain ladder (and its opioid-focused recommendations) as the standard for pain treatment, even in cases of chronic pain of non-cancerous origin.
The WHO cancer pain ladder established mutually beneficial partnerships between pain specialists, cancer specialists, global-health administrators, and pharmaceutical manufacturers. Through their collaboration with these fields, pain specialists began to accept once heterodox opioids as a powerful resource for their field, connecting them to public-health officials and pharmaceutical funding. Participation in this emergent global network of pain expertise also appealed to pharmaceutical companies. Purdue Pharma’s OxyContin was still a decade away, but projects like the cancer pain ladder, which destigmatized the use of morphine and other prescription opioids, were strategic for pharmaceutical companies. They promised a pathway to a favorable humanitarian reputation for companies publicly committed to ensuring global access to analgesics, and they expanded those companies’ potential markets.
The WHO pain group’s initial focus on opioids for cancer pain is important. Pain and palliative care specialists framed the risk of opioid misuse as secondary to the pressing need to quickly alleviate cancer patients’ suffering. Medical providers, public-health officials, and politicians consistently position cancer patients as the model pain patient, avoiding “difficult patients” with chronic non-cancer pain, who are often portrayed as malingerers and possible drug-seekers. As one pain-patient advocate explained, chronic pain patients, in contrast to cancer patients, “are seen as weak of mind, weak of spirit” (Interview, U.S., 2017). 1 The worthiness of cancer patients’ pain, and the perceived moral imperative to relieve terminal cancer patients’ suffering, helped justify the WHO’s focus on pain, the turn to opioids as a resource, and calls to establish rights to pain relief. Yet other pain patient groups also stood to benefit. Global pain-management efforts in the 1980s developed alongside the growing international HIV/AIDS crisis, which was responsible for a new population of chronic pain patients. Rates of non-cancer chronic pain conditions were also on the rise (Global Burden of Disease Study 2013 Collaborators 2015).
Framing suffering as a public-health and human-rights concern opened opportunities for collaboration between medical, humanitarian, political, and industry fields, establishing the basis for a global network of pain expertise. Pain specialists’ and public-health officials’ partnerships with pharmaceutical companies increased the moral capital of the oft-stigmatized pharmaceutical industry. In exchange, the pharmaceutical industry contributed economic capital to the network of pain expertise. Opioids, selected by the network as the “right tool for the job,” defined the scope of the humanitarian promises the network could make, laying the groundwork for a seemingly achievable human right to pain relief. Pain specialists, situated at the intersection of chronic pain and palliative care, could claim they were uniquely positioned to provide the technical expertise to standardize and implement safe opioid therapies. International pain specialists asserted that their field was the right medical specialty to lead the charge.
Thus, the initial creation of the WHO cancer pain ladder was as much a technical project as it was a moral one. As public-health officials committed to destigmatize opioids to improve global access to pain management and palliative care, pain specialists and the broader pain network gained credibility, not only as medical experts, but also as moral actors. Humanitarian leaders now took note of the issue of pain relief. In 1987, Bonica was invited to meet Pope John Paul II to discuss the IASP and the humanitarian work of its spin-off organization, the International Pain Foundation (Jones 2010:25). With access to pain relief recognized as a worthy humanitarian goal, pain specialists found increased visibility and support from fields outside of medicine and public health.
These developments, in conjunction with pressure from palliative care activists and cancer patient advocates, built momentum for programs to track and ensure access to opioid analgesics as a human right. In 1989, the United Nations International Narcotics Board (INB) adopted recommendations for member countries to train healthcare providers on best practices in cancer pain management. Until the 1980s, the INB, formed in 1961 as part of the Single Convention on Narcotic Drugs, had primarily regulated the global manufacture and distribution of narcotics. However, after 1989, the INB began to monitor how effectively UN member countries provided medical access to opioids. The international collection of prescription opioid statistics had begun. Here, national metrics on medical opioid consumption emerged as indicators of a healthcare system’s ability to provide patients with adequate pain relief (Interview, Pain Specialist, U.S., 2018).
The push to recognize opioid-centric pain relief as a global health goal incrementally gathered steam over the 1990s and 2000s, broadening to encompass chronic non-cancer pain. Newfound political interest in pain management beyond palliative care provided opportunities for pain specialists to assert their field’s autonomy as a medical specialization in many countries. Publications produced by the WHO, and partnerships between professional groups like the American Medical Association, the European Pain Federation, and pharmaceutical companies and patient advocates defined access to pain relief as access to analgesics. Multi-modal approaches were cumbersome, requiring healthcare infrastructures that could attract, coordinate, and reimburse interdisciplinary teams of specialists to assess patients’ subjective needs. Opioids appeared as a feasible one-size-fits-all solution—not ideal, but perhaps the only way to deliver on the promise of providing pain relief as a right. Opioids’ material qualities appealed to public-health, big pharma, and global-health advocates, increasing opioids’ power to shape the future of pain expertise and the meaning of a right to pain relief. Throughout the 1990s, patient-controlled anesthesia pumps, pain scales, and new formulations of prescription opioid tablets (specifically oxycodone and tramadol) cemented the selection of prescription opioids as the tool to manage the global pain problem. Destigmatized, opioids were now the symbol of pain management in global health.
The global pain-specialist field’s humanitarian commitment to promote pain management led to its actors participating in movements to recognize pain relief as a human right. In 2004, the WHO, the IASP, and the European Federation of IASP Chapters launched a campaign to declare pain relief a human right (Brennan, Carr, and Cousins 2016; Cousins et al. 2004). In 2010, as news of the North American prescription opioid crisis spread, the IASP drafted the Declaration of Montreal for the organization’s International Pain Summit. The Summit was attended by “250 representatives from 84 countries and professional and human rights organizations” (Brennan et al. 2016:1785). Broadening the scope of pain-patient rights to include chronic non-cancer pain, the Declaration demanded global recognition of “[t]he right of all people to have access to pain management without discrimination; the right of people in pain to the acknowledgment of their pain and to be informed about how it can be assessed and managed; and the right of all people with pain to have access to appropriate assessment and treatment of the pain by adequately trained health care professionals” (IASP 2010).
The assertion that “adequately trained health care professionals,” presumably pain specialists, are integral to a human right to pain relief demonstrates pain specialists’ attempt to protect their field’s boundaries and autonomy in the face of the opioid crisis. Many of the pain specialists and public-health administrators I interviewed continue to believe that improving access to pain management is a moral obligation. However, opioids have escaped pain specialists’ control as a highly addictive agent. Re-stigmatized opioids destabilized the inter-field relationships once built on a shared commitment to increase opioid availability to deliver a human right to pain relief. Thrown into crisis, the global network of pain expertise and initiatives to combat pain suffered a dramatic loss of credibility. The reverberations of this shift are now felt across the globe.
From Global Health to National Approaches: Opioids and Pain Expertise in the United States and France
To further illustrate how opioids as linking technologies shaped and unsettled pain expertise, I now turn to two national contexts: the United States and France. In the sections that follow, I trace these two countries’ parallel pain-management histories. I show how pain specialists overcame internal field struggles to invest in the material and symbolic value of opioids as linking technologies. I then demonstrate that the difference in magnitude between U.S. and French opioid prescribing and crises of pain expertise reflect how each country’s field of pain specialists leveraged opioids as resources in their professional fielding projects. Pain specialists’ success or failure to use opioids to protect their field’s autonomy affected how each country’s field could manage opioids as technologies capable of overrunning and destabilizing the broader network of pain expertise. Thus, national variation in how pain specialists adopted opioids as links to other fields in the network set the two countries on different paths, shaping the internal field dynamics of pain specialists, the relative dominance of opioids over multi-modal approaches, and the definition of patient rights to pain relief.
The United States
Throughout the late 1980s and 1990s, U.S. pain specialists, professional medical associations, public-health agencies, and the pharmaceutical industry co-produced pain expertise. Pharmaceutical companies provided financial support for pain-management professional societies and underwrote expert lecture circuits that promoted the “fifth vital-sign movement,” which mandated pain be treated as a fifth vital sign and evaluated and monitored like pulse, temperature, blood pressure, and respiration (Chiarello 2018; Meier 2003; Wailoo 2014). These inter-field efforts extolled the virtues of opioids in treating acute, cancer, and chronic non-cancer pain.
Adopting opioids as orthodox to the pain-specialist field opened access to pharmaceutical resources, but pain specialists were not passive representatives of pharmaceutical interests. Pain specialists tried to leverage their support of opioids to sustain support for complementary non-pharmacological approaches. Prominent pain specialists like Dr. Russell Portenoy have recently gained notoriety and legal exposure for their work in the 1980s and 1990s that promoted the safety of opioids (McGreal 2019), but even Portenoy argued for the continued value of a multi-modal approach—particularly cognitive behavioral therapy—to effectively treat chronic pain (Portenoy and Farkash 1988; Portenoy and Foley 1986). Portenoy and Foley’s (1986:183) infamous (now repudiated) research note, which suggested long-term opioid therapy for chronic pain was safe and effective, included the following caution: Opioid maintenance therapy should be considered only after all reasonable attempts at pain control have failed and persistent pain is the major impediment to improved function. . . . Improved function, however, should always be pursued during opioid maintenance therapy through the concurrent use of ancillary cognitive/behavioral and physical therapies.
In this research note, arguably the most influential early endorsement of opioids by pain specialists, Portenoy and Foley advocated for multi-modal and non-pharmacological therapies. Such balanced recommendations were common among U.S. pain specialists, who worked with pharmaceutical interests to destigmatize opioids while fighting for the expansion of multi-modal clinics to better address pain.
As pain specialists called for the maintenance of multi-modal approaches to pain management, U.S. public-health organizations seized on the promise of opioids. In 1993, the American Medical Association (AMA 1993:412) resolved to “investigate the barriers to appropriate management of pain, including institutional restrictions, intimidation by regulatory and enforcement agencies, and the attitudes of health care professionals.” The report compiled in response to this resolution carefully states that its recommendations only pertain to acute and chronic malignant pain. However, the report focused solely on opioids as the tool of pain management: Concern about addiction should never result in undermedication for acute pain. . . . Fear of inducing addiction should never be the basis for withholding opioid agents from a patient without a history of substance abuse. Patients with a history of opioid abuse present a special problem, but opioids can be used safely and effectively to control pain in such individuals and should be used when indicated to control pain. Withholding of therapy in the patient with a history of addiction when opioid drugs are clearly indicated is inappropriate and unacceptable. (AMA 1995:310)
Even for patients with a history of addiction, the AMA stressed the fundamental right to appropriate pain relief through the administration of opioids.
The AMA would go on to draft a model bill for U.S. state legislatures. In 1997, the AMA Board of Trustees recommended a policy statement confirming that “the AMA supports the position that physicians who appropriately prescribe and/or administer controlled substances to relieve intractable pain should not be subject to the burdens of excessive regulatory scrutiny, inappropriate disciplinary action or criminal prosecution” (AMA 1997:16). The AMA’s legal advocacy in this period demonstrates how opioids, cast as the tool to provide patients with a right to pain relief, brought pain specialists, pain-patient advocates, and the nation’s most powerful professional medical association together to protect doctors’ professional discretion in pain management. However, it also signals the symbolic erasure of the multi-modal model in favor of opioids in U.S. public-health strategies to improve pain management.
Concurrent with the AMA’s advocacy in 1997, leading U.S. pain-management professional societies, the American Academy of Pain Medicine (AAPM) and the American Pain Society (APS), issued a consensus statement on “The Use of Opioids for the Treatment of Chronic Pain.” Noting that “in the last several years, health policy-makers, health professionals, regulators and the public have become increasingly interested in the provision of better pain therapies,” the statement cited U.S. Department of Health and Human Services Clinical Practice Guidelines, which validated “that opioids . . . are an essential part of a pain management plan” for acute pain and cancer pain (AAPM and APS 1997). The AAPM and APS (1997) used these guidelines to suggest the use of opioids to manage chronic non-cancer pain deserved similar protection, with the caveat that the statement “not be misconstrued as advocating the imprudent use of opioids.”
The AAPM and APS (1997) endorsed opioids for chronic pain while justifying the continued relevance of the multi-modal model, explaining, “Many strategies and options exist to treat chronic non-cancer pain. Since chronic pain is not a single entity, but may have myriad causes and perpetuating factors, these strategies and options vary from behavioral methods and rehabilitation approaches to the use of a number of different medications, including opioids.” In the recommendations that followed, these elite organizations in the pain-specialist field attempted to strengthen the field’s authority, arguing that pain specialists’ technical expertise was necessary to assess when opioids were the right tool for managing chronic pain: Treatment planning should be tailored both to the individual and to the presenting problem. Consideration should be given to different treatment modalities, such as a formal pain rehabilitation program, the use of behavioral strategies, the use of noninvasive techniques or the use of medications, depending upon the physical and psychosocial impairment related to the pain. . . . An opioid trial should not be done in the absence of a complete assessment of the pain complaint. . . . Consultation with a specialist in pain medicine or with a psychologist may be warranted, depending on the expertise of the practitioner and the complexity of the presenting problem. (AAPM and APS 1997)
The AAPM and APS recommendations capture a fateful moment in the trajectory of the U.S. pain-specialist field. Elites in this field appreciated that health policymakers and regulators had finally recognized pain management as a public-health problem. However, pain specialists understood that these auxiliary fields interpreted the problem of undertreated pain as a problem of under-utilized opioids. In a bid for authority, pain specialists asserted their professional jurisdiction over appropriate opioid-prescribing. Thus, the U.S. field of pain specialists accepted opioids as orthodox, redefining the boundaries and organizing principles of their field, and linking part of their professional identity to opioid prescribing.
Reflecting on this history, a leading pain specialist (Interview, U.S., 2017) described the turn to opioids in the United States as a move to encourage the unification of an already “fragmented” field besieged by institutional challenges to its work: In the 80s, we began to feel that pain deserved to have more attention and that there were a lot of people who were suffering that we basically thought we didn’t have any tools to address. There were really . . . two different philosophies of how to address the pain problem . . . a multidisciplinary approach was always fundamental to the treatment of pain. But the payers were not onboard for that, and it was mostly palliative treatment [because] it wasn’t about curing. It was about just trying to make people more functional. . . . The pharmacology approach, nothing worked well except opioids it seemed, so opioids became the common treatment.
This doctor glossed the intra-field struggles among pain-specialists throughout the 1980s and 1990s: a tension between a palliative multi-modal approach meant to help chronic pain patients regain functionality, and a seemingly curative, results-oriented opioid-centric direction. He noted that this internal field struggle over best practices was partially settled by shifts in the U.S. healthcare system (including Medicaid and Medicare) toward managed care, and its reluctance to reimburse interdisciplinary, non-pharmacological therapies oriented toward regaining function rather than eliminating pain. This observation echoes analysis by psychologists specializing in chronic pain that “as a means of cutting costs, managed care organizations have been ‘carving out’ portions of the integrated comprehensive [pain management] programs by sending patients to outside providers for their various needs (because they have contracted with such providers, who cost them less) even though such providers do not have an understanding of true interdisciplinary care. This fragmented care dilutes the successful outcomes of integrated programs” (Gatchel et al. 2014:127).
Payers and public-health officials preferred opioids’ seemingly curative properties. Opioids’ apparent efficiency and low labor costs won out over the time-consuming and labor-intensive multi-modal approach, even when the majority of pain specialists viewed the multi-modal model as the safest evidence-based therapy. This preference shifted the availability of material resources within the network of pain expertise. In so doing, it presented pain specialists with a conundrum: embrace the demands of a healthcare system intent on quick fixes prescribed by a single provider or continue to defend cumbersome multi-modal clinics. Here, the pain specialists I interviewed claimed it was less incentives from pharma and more a public-health interest in the efficiency of opioids and the constraints imposed by “payers” (insurance companies and hospital administrators) that convinced skeptical pain specialists to champion opioids as orthodox to their field. This move to align the field with the desires of public-health operatives and insurers weakened the autonomy of the U.S. pain-specialist field and symbolically reduced its work to opioid prescribing.
With opioids as the organizing technology of the broader network of pain expertise, U.S. pain specialists lost their multi-modal clinics. In 1999, an estimated 1,000 multi-modal pain-management clinics operated in the United States; by 2011, this number was approximately 150 (Jeffery et al. 2011; Schatman 2010). Research grants offered by pharmaceutical companies, the realities of reimbursement under the managed care model (Robbins et al. 2003), and the promotion of opioid accessibility by global-health actors and humanitarian organizations meant pain specialists viewed the survival of their field as tied to developing specialized expertise around opioid-prescribing best practices (Interviews, U.S., 2017 to 2018).
Pain specialists ambivalently adapted to the opioid-focused agenda, finding creative ways to practice interdisciplinary pain medicine without a clinic structure, and many relied on pharmaceutical funding to continue research and political lobbying around chronic pain as a public-health crisis. Some pain specialists reportedly left the field rather than face these institutional challenges to a once multi-modal profession, returning to practice under their primary specializations of anesthesiology, physiology, or neurology. This movement of actors out of the field reintroduced a threat to the pain specialty’s autonomy and survival.
The weakening of the U.S. pain-specialist field’s boundaries intensified after Purdue Pharma’s launch of OxyContin in 1995, which paved the way for the widespread uptake by non-specialist general practitioners of the new extended-release, and purportedly “safer,” formulation of oxycodone to treat patients’ pain. As general practitioners became more confident they could manage their patients’ pain with opioids, pain specialists received fewer referrals. This was concerning both professionally and ethically for pain specialists because, as several of my respondents explained, chronic pain patients require careful, specialized care and monitoring, especially if prescribed an opioid regimen. Pain specialists responded by reasserting their disciplinary boundaries, casting themselves as the right specialty to oversee safe and effective opioid management therapies.
During this time, an onslaught of publications in leading medical journals, pain specialists’ media spots, and aggressive advertising methods utilized by pharmaceutical companies pressured hospitals and medical providers to evaluate patients’ pain using 0 to 10 pain scales (Chiarello 2018; Meier 2003; Sherman 2017). A 2001 decision by the Accreditation, Healthcare, Certification Organization (Joint Commission) mandated that every patient’s pain be assessed during each clinical encounter. One prominent pain specialist (Interview, U.S., 2017) involved in U.S. pain-management education and policy reform reflected on the role of the 0 to 10 pain scale in reorienting pain-management expectations to realize the promise of opioids as a quick fix: I think we have a problem as a society, at least in this country, instant gratification and a pill for every ill. This 0 to 10 pain scale, which is an intensity scale, if that’s your only measure. I’m an anesthesiologist by training, there’s nobody on the planet I can’t get their pain to zero. Now they might be on the carpet blowing spit bubbles, but that wasn’t the question. The question was get their pain to zero.
As healthcare institutions implemented 0 to 10 pain scales as the metric of effective pain management, opioids were one of the only tools that could meet the potentially dangerous expectation that patients’ pain levels should be reduced to zero. The power of opioids drove new norms that pain could be totally eliminated. Pain scales and the expectations that accompanied them were incompatible with the multi-modal model, further weakening support for specialized, interdisciplinary pain management.
American pain specialists’ move to embrace opioids as orthodox to the pain-specialist field did not produce the intended effect of increasing the field’s resources and autonomy. In fact, relying on opioids eroded the field’s boundaries. Physicians and nurses without specialized pain training comfortably prescribed opioids for chronic pain patients. With an emphasis on “instant gratification,” patients and healthcare institutions balked at the “tailored” interdisciplinary pain assessment outlined by the AAPM and APS in their 1997 chronic pain opioid-prescribing recommendations.
With opioids as the gold standard for pain relief, patients began to see their right to pain relief as a right to be prescribed opioids. Another pain specialist (Interview, U.S., 2017) explained: It was well accepted and appreciated that we should treat pain. That’s where we got the specific vital sign and whatever pain is, or a patient says it is, it is. It is a human right to have your pain treated. That was all the 90s, and then probably in the early part of this century. . . . Now in the last five years, certainly since 2010, the emphasis is all about the harm of the opioids and there is almost no attention to the needs of people in pain, because pain treatments for maybe a decade was synonymous with opioids. I mean, they were almost viewed as if you had pain, that meant you were going to get opioids as opposed to the way one should think about it.
“Synonymous” with pain management, opioids pushed U.S. pain specialists to develop their reputation as expert opioid prescribers to ensure the steady flow of resources from other fields in the network of pain expertise. From the mid-1990s onward, opioids dominated the network as an imperfect tool, edging out other approaches.
By 2010, rates of prescription opioid misuse and overdose in the United States raised alarm. Specialists once revered as preeminent pain experts faced legal prosecution based on patient overdose deaths and their record of opioid prescribing (Chen and Schulzke 2017). In 2019, the American Pain Society, the U.S. branch of the International Association of Pain and an elite actor in the field of pain specialists, declared bankruptcy and dissolved after facing numerous lawsuits alleging it was a front for pharmaceutical interests (an allegation the Society’s leadership and prominent pain specialists fiercely deny) (Clark 2019).
A history of pharmaceutical funding to support pain-management initiatives had been a marker of status in the professional field of pain specialists, but now, any record of receiving research funding from opioid manufacturers could tarnish a pain specialist’s reputation. The stigma reattached to prescription opioids meant these technologies, once a bridge for the exchange of resources between the pharmaceutical industry, public-health officials, and the field of pain specialists, were now the source of discord and crisis. Opioids had escaped pain specialists’ control. A pain researcher (Interview, U.S., 2017) involved in interagency public-health initiatives around pain described this dynamic: The opioid thing kept growing and growing . . . so at that point, there was a lot of nervousness amongst the pain community and the efforts that began to really take traction in addressing the opioid epidemic and people were worried that we no longer would be able to get the medications that we need. We’re going to be more stigmatized because people are starting to see us as part of the problem . . . as having created the opioid crisis problem.
The gravity of the opioid epidemic destabilized the broader network of pain expertise and all but dissolved the already weak U.S. field of pain specialists. The positive humanitarian associations between opioids and a right to pain relief were spoiled, and the technology that once had offered pain specialists resources held no value, especially with actors in the public-health field now focused on stemming the opioid epidemic. With the opioid crisis came what several U.S. interviewees identified and experienced as intense “legal scrutiny” of the pain specialization and concerns about the “chilling effect” on doctors’ willingness to treat patients’ pain with or without opioids (Interviews, Pain Specialists, U.S., 2017 to 2018).
Can over-prescription of opioids in the United States be solely attributed to an outsized influence of pharmaceutical companies exceptional to the U.S. context? My findings indicate that the pharmaceutical industry certainly contributed to U.S. pain-management expertise and policy. However, pharma’s power insufficiently explains why public-health officials and pain specialists selected and promoted opioids as the tool to deliver a right to pain relief. The fit between opioids’ material qualities and the demands of a U.S. healthcare system oriented toward quick and seemingly curative therapies collided with the belief that a right to pain relief was worth the gamble of prescribing narcotics. Opioids had seemed to meet the diverse professional needs of fledgling pain specialists, eager public-health advocates, and medical organizations. Once highly addictive opioids proved unmanageable by these fields in the U.S. network of pain-management expertise, the field of pain specialists fell into crisis. Already suffering from fragmentation and weak boundaries, the U.S. field of pain specialists lost the requisite autonomy and authority to direct the future of pain-management expertise, leaving patients without access to opioids or multi-modal clinics.
France
Tracing the history of the French network of pain expertise reveals a parallel story of opioids as a linking technology. Pain specialists worked with public-health officials to destigmatize opioids as the tool of pain management, drawing on pharmaceutical funding for pain research and advocacy, and encouraging the idea of an achievable patient right to pain relief. However, French pain specialists more successfully strengthened their field’s boundaries, protecting against the crisis of credibility that befell their U.S. colleagues. French pain specialists effectively institutionalized the multi-modal model alongside opioids as approaches to pain management in the French healthcare system. Acquiescing to an opioid-centric public-health approach, the French pain specialty accrued resources and political partnerships, but they leveraged those inter-field relationships to safeguard multi-modal clinics in public hospitals.
Throughout the 1970s and 1980s, French physicians with an interest in pain management tracked developments in the United States and began to organize around pain management as an informal subspecialty (Baszanger 1998). French doctors and researchers were well-represented through the early years of the IASP (Jones 2010:11). Baszanger finds that two defined camps of pain specialists emerged and compromised to establish the French pain-specialist field throughout the 1980s and early 1990s. One group, led by anesthesiologists and neurosurgeons who were well-connected to national public research institutes, focused on applying gate control theory to accurately diagnose the causes of chronic pain, aiming to cure patients’ suffering (Baszanger 1998:121, 124). The second multidisciplinary group, composed of neurophysiologists, neurologists, general practitioners, and psychiatrists/psychoanalysts, sought to apply gate control theory’s insights through a holistic perspective that recognized social-psychological factors in chronic pain patients’ pain perceptions (Baszanger 1998:131–32). This second group approached chronic pain as difficult, if not impossible, to cure and thus focused on developing treatment strategies to manage pain through psychological and physiological interventions (Baszanger 1998).
Despite the two groups’ different perspectives, they shared a commitment to the multi-modal pain clinic model, and they found common ground in the goal to strengthen the boundaries of the pain specialty field in the French healthcare system and medical education. They worked together to enlist political support for certifying, standardizing, and institutionalizing pain centers across France. My archival findings suggest that through the French pain-specialist field’s encounters with public-health officials, health policymakers, and pharmaceutical representatives, pain specialists from both camps cautiously adopted a politically popular pro-opioid stance with assurances from public-health officials that the government would recognize and support the continued expansion of pain clinics in the public hospital system. Opioids’ strongest French proponents tended to be doctors who moved between pain and palliative care fields. However, even these opioid advocates recognized the multi-modal model as orthodox and core to the pain-specialist field’s professional identity.
Following the WHO analgesic ladder in 1987, the young field of French pain specialists began to partner with politicians to bring attention to the problem of undertreated pain. In 1993, Paris hosted the IASP’s Global Congress on Pain. By 1994, French legislators targeted pain management as a priority of new health policy. Politicians justified efforts to reform pain management in the healthcare system by pointing to France’s poor ranking in international statistics on opioid consumption. The French Minister of Health condemned the healthcare system’s failures in pain care: “It is obvious, our country, today, lags behind in the fight against pain. As such, we rank 39th, globally, for the prescription of opioids” (Sénat 1994:5766).
Such damning evaluations of the French healthcare system’s place in the global order of pain relief coincided with the watershed, now discredited, assertion that opioids, when prescribed to patients with legitimate pain, were not addictive (Portenoy and Foley 1986). Evoking this building consensus in pain science, the French Minister of Health heralded the country’s initial pain-management reforms as “historic”: “For cultural reasons, our country is not in the habit of considering pain, and the biases are impressive with regard to pain management. For example, we are always afraid that patients will become dependent on morphine. However, we know very well that morphine administered orally does not pose any threat of addiction. This is what must be taught to doctors and to medical students” (Sénat 1994:5767). Pain specialists, public-health officials, and politicians used comparative opioid consumption statistics as the primary evidence of their health system’s failure to deliver relief from suffering. Opioids thus accrued symbolic value in the French network of pain expertise.
In 1994, Senator Lucien Neuwirth directed the first report on pain in France. The report begins with a quote from the WHO’s Declaration of the Right to Health, setting the tone for a human rights framing of the French pain problem (Neuwirth 1994:5). In the years that followed, the French public-health officials responsible for the administration of pain-management reforms were embedded in the field of global-health humanitarianism. Bernard Kouchner, Philippe Douste-Blazy, and Jean-François Mattéi, some of the most involved directors of pain-relief reforms during their tenures as Ministers of Health, served as leaders in Doctors without Borders, UNITAD, and the Red Cross, respectively. Other Ministers of Health who oversaw important pain-management reforms had previously worked for the French branches of multinational pharmaceutical companies. French politicians in the field of global-health humanitarianism and the global pharmaceutical industry favorably observed that opioids could make a human right to pain relief possible. The French political field thus gravitated to opioids as the tool for pain management.
In response to these opportunities to partner with politicians, pain specialists supported the destigmatization of opioid use in the French healthcare system. However, prominent pain specialists continued to lobby for multi-modal pain clinics and non-pharmacological approaches. Amid opioid optimism, Dr. François Boreau, a luminary in the French pain-specialist field, advised congressional leaders that the pain problem went beyond opioids and the needs of terminal patients. Boreau contended that multi-modal pain centers would remain necessary to treat complex chronic pain even if opioid restrictions were relaxed: Many [pain] patients will need to be supported, not because they have terminal illnesses, but because they will have to live with pain and reintegrate socially and psychologically. . . . In other words, one of the main axes of the consultation of pain is this double sidedness of a strictly classical medical approach and of a broad psycho-social approach. This is made possible by clinics where rheumatologists, anesthesiologists, neurosurgeons, psychiatrists, psychologists, neurologists, etc. collaborate in the same team. All these skills need to collaborate in an integrated way in a pain team. (Boreau quoted in Neuwirth [1994:90]; translated from French by the author)
Boreau implied that chronic pain could not be easily cured but could be effectively managed to help patients “live with pain and reintegrate socially and psychologically.” This perspective reflected his membership in the group of pain specialists committed to palliative pain management rather than curative pain relief. Both groups of French pain specialists conceded that France’s strict opioid regulations prevented the appropriate treatment of severe pain experienced by (often terminally ill) patients. However, the consolidating field of pain specialists focused on exploiting political interest in the pain problem to institutionalize multi-modal pain clinics across the country.
Following consultations with leaders in the pain-specialist field, French public-health officials gathered data to establish more regional pain centers in France. Yet, politicians and the Ministry of Health continued to publicly frame the pain crisis as one of inadequate opioid prescribing. In 1999, Bernard Kouchner, then Minister of Health, wrote the preface to a leading French pain-management medical education text, underscoring that his experience with Doctors without Borders informed his belief that medical professionals had a moral obligation to treat those suffering from pain with morphine: Pain expresses the human part of illness, injury, and care. Basically, it is the only serious thing in medicine. Why have so many doctors neglected it? They have retained their power while avoiding the management of suffering. French doctors, since the turn of the century, have refused to sufficiently use opioids and other analgesics. They intended to preserve their profession and give it, in times when science was looking for it, a grandeur that it did not have. (Kouchner 2001:x, translated from French by the author)
Drawing on his work in global-health humanitarianism, Kouchner critiqued French doctors who sought professional grandeur, sidelined suffering as unscientific, and refused to prescribe opioids. Kouchner celebrated the field of pain specialists, who prioritized the “human” concern of pain over technical, biomedical “grandeur,” but he linked the obligation to treat pain with the provision of opioids.
Kouchner and other officials in the French public-health field sidestepped medical debates around theories of pain perception and treatment goals that defined the intra-field struggles between French pain specialists. Instead, public-health officials encouraged pain specialists to unify and develop plans to improve opioid access for suffering patients. Successive Ministers of Health approached improving access to opioids as an achievable and politically expedient objective. Initial pain-management reforms passed by French Parliament in the 1990s focused on dispelling perceived misconceptions among the medical community around the dangers of morphine and other opioid formulations. Through negotiations with multinational pharmaceutical companies, the government purchased and distributed patient-controlled anesthesia pain pumps to hospitals. The Ministry of Health circulated guides to pain management, emphasizing the physician’s duty to treat pain. Hospitals did away with the cumbersome carnet à souche—a special protocol for prescribing and dispensing morphine that made delivering morphine to patients in pain a lengthy and bureaucratic process, in favor of streamlined securitized pharmaceutical scripts. However, these opioid-centric pain reforms also delivered on requests from the field of pain specialists to ensure the multi-modal model’s place in French healthcare. The government approved expanded pain-management training for medical students and the development of multi-modal pain-management centers.
During this time, pharmaceutical manufacturers competed for contracts with the French government to furnish the equipment needed to increase the healthcare system’s capacity to provide opioids. These contracts were signed against the backdrop of political support and public funds for innovative pharmaceutical research, development, and manufacturing activities (Bonnemain and Bonnemain 2002:245). Along with implementing opioid technologies like patient-controlled analgesia pumps in hospitals and distributing guidelines that encouraged the use of analgesics for patients in pain, the Ministry of Health also exhorted doctors to consult their local multi-modal pain center on complex pain cases. New public-health policies relaxed regulations around the prescription of opioids, but they also reaffirmed the importance of pain specialists’ multi-modal expertise in managing patients’ pain with opioids. Pain specialists increased their political reach within the French healthcare system by working with the government to revise opioid regulations. In this way, pain specialists solidified the boundaries of their field, establishing themselves within the French healthcare landscape through their engagement with politicians around opioid availability, while building political support for a national system of interdisciplinary pain specialists, housed in clinics.
In 2002, Kouchner, acting as Minister of Health, produced a new patients’ rights health code. The code required that pain contracts and pain scales be distributed by hospitals to every patient. At the direction of the Ministry of Health, pharmaceutical companies developed model sliding pain scales. These pharmaceutical companies also produced the most popular analgesics in the French market—including formulations of fentanyl, morphine, tramadol, and codeine. As a result of this inter-field partnership, the very tool used to measure patients’ pain often advertised prescription opioids or devices for their administration. Opioids continued to wield tremendous symbolic and material power in the French network of pain expertise.
Early working partnerships between French public-health administrators and pharmaceutical companies led to the pain problem being framed as an under-utilization of opioids. The positive symbolic value ascribed to opioids as linking technologies lasted until 2004, when a prominent pain specialist and advisor for pain-management policy questioned whether French doctors might now be overprescribing opioids. In an email to relevant officials at the Ministry, the pain specialist cited the latest data on pharmaceutical consumption patterns released by the National Conservatory of Arts and Crafts (CNAM), a research and higher-education institution run by the French government: For the first time . . . pain management medications comprise the largest volume of prescriptions. . . . The incorrect use of strong opioids (morphine and its derivatives) equally sustains numerous concerns. . . . Portenoy, in a Lancet editorial, on August 28th 2004, underlines the dangers of inappropriate prescribing of strong opioids in non-cancer pain with a notable risk of iatrogenic addiction that has widely touched the USA over the last years. . . . Until present, no official alert has been given about the specific French context. (Direction Générale de la Santé Archives 2011)
Summarizing the risk posed by relying too heavily on strong opioids in pain management, the email underlined the potential public relations nightmare that could result from a perceived collaboration between the government, pain specialists, and pharmaceutical companies: Finally, the Ministry planned . . . a public meeting (that should be very well-covered by the media) . . . this private [pain advocacy] initiative is financed at 95% by commercial pharmaceutical laboratories. According to our information, alarmist numbers will be put forward. . . . In order to avoid manipulation by the media, it seems to me, an urgent necessity to make a brief update within the Ministry in order to unify and calibrate our responses. (Direction Générale de la Santé Archives 2011)
As mounting coverage of the opioid crisis in the United States made international headlines, actors in the French pain-specialist field found themselves in a new position. France’s low prescription-opioid consumption index once justified moral outrage and catalyzed political interest to bolster resources for French pain specialists. Now, however, French public-health actors and pain specialists began to plan how to “recalibrate” their relationship to opioid technologies. This recalibration coincided with the end of sustained political support for the recognition of pain as a public-health crisis in France. Pain specialists rapidly returned to emphasizing their multi-modal rather than opioid-centric work. Yet, the loss of opioids as a linking technology to political and public-health fields prompted concern among pain specialists that their pain centers would soon face administrative budget cuts (Interviews, France, 2017 to 2018).
From 2010, while Purdue Pharma faced legal sanctions in the United States, its global arm, MundiPharma, continued to fund pain-management research, advocacy, and lobbying efforts in France. Publications from these partnerships consistently framed access to opioids for pain relief as a humanitarian goal, describing pain management as a “fundamental right of the patient” and a “human right.”
Quietly using resources from Mundi-Pharma for research and lobbying efforts, French pain specialists publicly distanced themselves from the stigma of opioid manufacturers. One French pain specialist (Interview, Pain Specialist, France, 2018) explained this relationship between the pharmaceutical industry and pain research and policy: We have a system of public education, which helps us. The fact that there is more government control . . . and the fact that professional expert societies . . . make an effort to [direct pain policy and research] that has helped. It’s not the absolute best, and . . . I think that it is getting better with time with research and now the expert recommendations [for opioid-prescribing practices]. . . . It’s a marriage of necessity [with the pharmaceutical companies], but with a little bit of separation . . . it’s like laïcité [separation between religion and the state] in France . . . between the pharmaceutical companies and [French pain specialists].
In France, the commitment to destigmatize the use of prescription opioids in pain relief productively linked pain specialists to public-health officials and global pharmaceutical companies like MundiPharma. Opioid-centric pain-management guidelines and the construction of a patient’s right to pain-relief emerged from these inter-field partnerships and continue to affect how lobbying and research around pain management are conducted in France. Working in the shadow of the opioid crisis, pain specialists distanced themselves from symbolically spoiled opioids, navigating a “separation” that destabilized their inter-field links to pharmaceutical companies, which once reliably provided funding for pain research and lobbying.
In this unsettled landscape, French pain specialists faced intensified intra-field struggles. Some pain specialists privately cast doubt on their colleagues’ research funded by pharmaceutical interests; others recognize that pharmaceutical grants are one of the only reliable sources of research funding after the pain crisis lost political popularity (Interviews, Pain Specialists, France, 2018). In the absence of new public-health pain initiatives and government support, pharmaceutical companies remain a lifeline for financing lobbying and research efforts that support pain specialists’ autonomy within the medical profession, but not without potential reputational cost. Faced with the “managerialization” of the French public hospital system (Hassenteufel and Palier 2007) and declining numbers of new doctors entering the pain field, pain specialists reported that their multi-modal clinics were under threat. One pain specialist (Interview, France, 2018) detailed how he stopped his hospital’s administrative plan to “quietly reorganize” its pain clinic due to budget concerns: Pain, normally, it must always be multidisciplinary in France. . . . They don’t talk of closing [the pain center] but of “reorganizing” it by keeping only one doctor, and even still that position is not certain. It’s not a pain center if it doesn’t correspond to the texts that define how we know that we are a [multidisciplinary pain] center. . . . If the [patient’s pain] complaint is always equated with prescribing opioids, then there’s no need for [specialized pain-management] training. These are simplistic [administrative] visions. . . . The problem is that the public system is bankrupt and there are huge financial problems. So here we are destroying hospitals and French medicine, which has been among the best.
Despite concerns over hospital administrations’ “simplistic vision” to rely on opioids, pain specialists have thus far maintained their field’s autonomy and authority by ensuring multi-modal pain clinics remain at the heart of French pain management. In 2017, there were 254 multidisciplinary pain centers in France (SFETD 2017). Demand for pain management continues to overwhelm these clinics, and a generation of pain specialists will soon retire, placing stress on the system. However, the number of pain clinics has held steady over the past 15 years. French pain expert societies (like the SFETD) remain respected professional organizations. Unlike their U.S. counterparts, French pain specialists defended their field’s boundaries by successfully preventing opioids from completely dominating pain expertise.
In summary, starting in the late 1980s, French and U.S. networks of pain expertise organized around opioids as a linking technology. Multiple fields selected and invested in opioids as the tool for pain management. Opioids connected each country’s young pain-specialist field to the more established and resourced political, medical-industry, and public-health fields. In both countries, pain specialists’ investment in opioids as a linking technology collided with institutional challenges to multi-modal pain management: the demands of healthcare delivery reform, reimbursement systems, and the pharma-dominated landscape of research funding.
In the United States, the shift to managed care and changing insurance-fee schedules amplified the power of opioids in the network of pain expertise, favoring the priorities of public-health, private insurance, and pharmaceutical fields over the vision of pain specialists. Thus, U.S. pain specialists’ endorsement of opioids ultimately weakened their field’s ability to steer the direction of the inter-field network’s expertise. In France, cost-control measures implemented by the government threatened the viability of the multi-modal clinic model in the public healthcare system. However, French pain specialists defended the boundaries of their field, justifying the value of multi-modal clinics and warning of the dangers of defaulting to opioids as the only tool for pain management. Thus, national variation in how pain specialists were able to adopt opioids as links to other fields in the network set the two countries on different paths, shaping the internal field dynamics of pain specialists, the relative dominance of opioids in pain expertise, and the survival of patient rights to pain relief in the wake of the opioid crisis.
Discussion
Focusing on how opioids shaped the rise and fall of a global network of pain expertise, I show that emergent scientific fields (i.e., the field of pain specialists) build relationships with economic and political fields (i.e., the pharmaceutical and public-health fields) through linking technologies. These relationships allowed pain specialists to accrue capital, assert their autonomy as a medical specialty, and implement their expertise in different institutional contexts. In this way, the field of pain specialists complicates extant sociological theories of professionalization, autonomy, and closure, because the field established itself through its interconnectedness to other fields and technologies.
Many contemporary spaces of knowledge production exhibit field and network-like characteristics, encouraging an inter-field exchange of resources (Camic 2013; Eyal 2013a; Medvetz 2012; Panofsky 2011). As Medvetz’s (2012:24) work on think tanks shows, fields oriented toward knowledge production draw on “a complex mixture of institutionalized resources . . . from the academic, political, economic, and media fields. However, the same organization must also seek to avoid the appearance of complete dependence on any of these institutions.” Medicine, which demonstrates its own field-like qualities (institutionalized and embodied sets of rules, objectives, and forms of capital) collaborates with and relies heavily on other powerful institutional fields, like the economic healthcare industry (including pharmaceutical and device manufacturers), the political (public-health and healthcare reimbursement systems), and the academic (clinical and basic research and medical education). The inter-field balance, constantly renegotiated to keep medical knowledge production humming, has been theorized as “countervailing powers” (Light 2005) and a product of (bio)medicalization (Clarke et al. 2003; Conrad 2007).
Understanding how technologies structure medical professionals’ interactions with other fields can explain why, despite consensus about evidence-based best practices within a specialized field, medical experts partner with politicians, pharmaceutical actors, patient advocates, and the media, who assert competing claims, leading to “credibility struggles” (Epstein 1998). My findings illustrate that linking medical technologies are a crucial mechanism of inter-field consensus and discord. Opioids, as resources, facilitated the exchange of capital across fields, building an opioid-focused network of pain expertise. Once selected as the “right tool for the job,” opioids, as actants, drove what forms of pain-management expertise, policy, and patient rights became dominant. Then, when opioids’ addictive properties escaped the control of pain-specialist and public-health fields in the network, they threatened the credibility of pain expertise.
The pharmaceutical industry alone did not determine the selection of opioids as the technology for pain relief. Groups of pain specialists in France and the United States initially saw opioids as heterodox to professional fielding projects rooted in the promise of multi-modal clinics for pain management. However, these groups cautiously accepted prescription opioids as orthodox due to opioids’ popularity with public-health officials, professional medical organizations, and humanitarian actors in the emergent inter-field network of pain expertise. Capable of injecting capital into the pain-specialist field, these auxiliary fields offered resources and recognition that pain specialists believed could help solidify the boundaries of their field against the threat of reabsorption by multiple, competing, and established medical specialties.
Leveraging their endorsement of opioids, pain specialists not only tried to distinguish their field from other medical specialties; they also attempted to exert their autonomy against the power of pharma and public-health fields in the network. By framing their work and knowledge as indispensable to the project of safely administering opioids, U.S. and French pain specialists gained clout in public-health administration. Offsetting their opioid-centric work, pain specialists in both countries used pharmaceutical resources to fund research centers, professional societies, and clinical studies that defended the efficacy of non-pharmacological therapies for pain, demonstrating autonomy from brute pharmaceutical interest.
Despite deploying some similar strategies to strengthen their fields, French and U.S. pain specialists used opioids as a resource to redefine their fields’ boundaries in different ways. It is important to note that pain specialists’ institutional environments affected how they were able to link up with other fields and define their own work through opioids. In both countries, political and economic pressures to reform healthcare delivery in the 1990s and early 2000s idealized efficient and cost-effective medicine (Gatchel et al. 2014; Hassenteufel and Palier 2007; Schatman 2010; Steffen 2010). Health administration privileged fast, standardized, and seemingly curative opioid-centric pain relief overseen by a single provider over the tailored, interdisciplinary approach of the multi-modal clinic.
In the United States, pain specialists struggled to maintain their multi-modal clinics through the shift to managed care, which restricted reimbursement and the necessary institutional infrastructure for interdisciplinary medicine (Gatchel et al. 2014; Robbins et al. 2003; Schatman 2010). Faced with these institutional challenges, U.S. pain specialists pivoted to opioids, riskily redefining their professional jurisdiction through a claim to specialized opioid expertise. However, opioids’ material qualities, specifically the ease with which oral formulations could be administered, coupled with the pain-specialist field’s already weak boundaries, led to the belief that opioid prescribing need not be a specialized practice. These beliefs undermined pain specialists’ attempts to redefine their field’s boundaries and assert their authority as experts in safe opioid prescribing. The field failed to consolidate, struggling to retain autonomy in the increasingly opioid-focused network of pain expertise. Then, evidence of the opioid crisis emerged. U.S. pain specialists’ involvement in the selection of opioids as the tool for pain management was public knowledge. The already weakly defined field could not defend against the threat that opioids, as out-of-control technologies, posed to their field and society at large. The U.S. pain-specialist field is now in crisis.
In France, pain specialists also reported mounting pressure from healthcare administrators to treat patients quickly and efficiently, challenging the time-intensive multi-modal model. However, the power of doctors’ unions to prevent proposed budget caps that would impede their work; a robust public hospital system overseen by a centralized health authority (Hassenteufel and Palier 2007); and national accrediting guidelines that stated pain centers in public hospitals should be multi-modal muted the effects of neoliberal healthcare reform on French pain specialists. These more favorable institutional conditions likely helped French pain specialists maintain their multi-modal clinics while investing in opioids as linking technologies.
Thus, French pain specialists managed the resources they accessed from the opioid-centric network of pain expertise to navigate changes to French healthcare politics and administration, ultimately defending their field’s boundaries. When opioids proved difficult to manage, French pain specialists leaned on their multi-modal work to reassert their professional autonomy, positioning their non-pharmacological therapies as solutions to the threat of opioids. The path forward for French pain specialists is uncertain. Hospital administrators still view multi-modal clinics as inefficient and costly, and pain specialists anxiously navigate a disrupted flow of resources from public-health and pharmaceutical fields thanks to the re-stigmatization of opioids. However, the French pain-specialist field’s stronger claim to autonomy through its multi-modal clinics has insulated it from blame for increasing opioid-related overdoses in France.
The differences in how French and U.S. pain specialists were able to maintain their fields’ autonomy, while linking with other fields through opioids, help explain why U.S. pain specialists lost the power to steer pain-management expertise. Struggling to unify their field, U.S. pain specialists’ opioid optimism led to a loss of autonomy and credibility. The U.S pain-specialist field’s failure to consolidate mirrors Panofsky’s (2014:34) observation of crises of expertise in behavioral genetics: “a field’s fragmentation, anomie, and persistent controversy are closely interrelated.” Similar to Panofsky’s behavioral geneticists, the U.S. pain-specialist field has been plagued by fragmentation, unable to unify behind treatment modalities other than opioids. By selecting opioids as the tool for pain management, the field linked itself to the interests of public-health and pharmaceutical fields. Scrambling to assert their authority in the opioid-centric network of pain expertise, U.S. pain specialists’ pivot to opioids cost the field its multi-modal clinics. From there, the field struggled to maintain its already weak boundaries and autonomy. Opioids overran the network of pain expertise, escaping the control of public-health actors, pain specialists, and even, arguably, the pharmaceutical industry.
Conclusion
Purdue Pharma’s recent 4.5-billion-dollar bankruptcy settlement with the U.S. government recognizes big pharma’s culpability in the opioid epidemic. However, politicians, plaintiffs, and judges argue that the settlement fees do not sufficiently hold these companies and their owners accountable (Hoffman 2021). In offering an inter-field account of the promotion of opioids for pain management, I do not mean to suggest big pharma did not knowingly and unconscionably profit from the opioid crisis. Nor do I intend to imply that pain specialists and their professional ambitions are to blame. I contend that a complete understanding of opioid overprescribing in the Global North warrants attention to what conditions provided incentives for the selection of opioids, by several fields, as the central tool for pain management. The opportunity for opioids to dominate pain expertise was created through multiple fields’ collaboration in responding to pain as a public-health crisis within institutional constraints that demanded efficient, one-size-fits-all, standardizable approaches. Opioids appealed to a diverse set of fields because they could be easily implemented, anywhere, amid changing cultural and political norms around the moral obligation to alleviate suffering.
Technologies, when deployed as a means to promote and deliver new humanitarian projects, like the right to pain relief, are powerful resources for professional fields looking to attain capital, autonomy, and credibility. The successful rebranding of prescription opioids as effective guarantors of a right to pain relief offered the pain-specialist field access to a broader network of interinstitutional resources with which to assert the indispensability of their specialized work. The opioid-focused guidelines produced by the network of pain expertise cannot be reduced to the pharmaceutical industry’s agenda. Opioids, when used appropriately, are an indispensable tool to provide relief to suffering patients. As fields in the network selected and organized around opioids as the “right tool” for pain management, pain specialists, public-health officials, healthcare institutions, and even nation-states worked to be leaders in the “fight against pain” by promoting opioid prescribing.
A growing body of sociological work examines the conditions that precipitate and insulate against crises of expert credibility (Alexander 2018; Decoteau and Daniel 2020; Eyal 2019; Panofsky 2014). In his work on the “societalization of social problems,” Alexander (2018:1049) argues that the “societalization” of problems happens “only when [problems] move outside their own spheres and appear to endanger society at large.” As a field loses control of the framing of the problem, “routine strains become sharply scrutinized, once lauded institutions are ferociously criticized, elites are threatened and punished, and far-reaching institutional reforms are lauded and sometimes achieved” (Alexander 2018:1050). Alexander observes that when a problem escapes a field’s control, public interpretations of the field’s work frame how the crisis is problematized. The civil sphere’s definition of a problem can challenge established fields’ dynamics, disrupting a field’s boundaries, internal hierarchies, and symbolic capital. Studies have focused on how professional fields lose control over crises through external scrutiny from the civil sphere or the incursion of competing institutional fields (Alexander 2018; Chiarello 2018). My findings demonstrate that linking technologies are also mechanisms of crisis for fields in networks of expertise.
Taking opioids as a case, this article demonstrates that the technologies selected by networks of expertise as “the right tool for the job” limit how professional fields can prevent, manage, and control emergent crises. The selection of a technology to solve a multi-faceted problem can serve field-specific interests but can also lead to crises of field autonomy and credibility. When a network of expertise stabilizes around a technology as “the right tool for the job,” the chosen technology structures how fields in the network exchange symbolic and material resources and demarcate their own boundaries (Clarke and Fujimura 2014; Krause 2014). Investing in a single technology to solve a problem limits how lawmakers, researchers, and practitioners co-produce policy and imagine alternative solutions. Fields within a network of expertise are exposed to crisis if and when the technology defies expectations and escapes control.
The relationship between opioids and pain expertise demonstrates the hazards of addressing complex social problems through silver bullet technologies. When expert actors select a technology to solve a problem, that technology’s material properties and symbolic value narrow how actors from different fields define their work, navigate institutional obstacles, and respond with resilience to unexpected outcomes. Several recent examples of technologies developed to fix vexing problems, such as self-driving cars meant to make our roads safer, vape pens promoted as a tool for smoking cessation, and even promising COVID-19 vaccines expected to end the pandemic, demonstrate that unbridled tech optimism can overtake expertise and policymaking in ways that limit how professionals can prevent, anticipate, and respond to emergent crises.
Footnotes
Acknowledgements
I thank Ann Orloff, Carol Heimer, Celeste Watkins-Hayes, Wendy Espeland, Charles Camic, Michael Rodriguez-Muñiz, Steven Epstein, Magda Boutros, Marie Laperrière, Emre Gerçek, Alka Menon, Savina Balasubramanian, Isabelle Baszanger, Elizabeth Chiarello, Anne Revillard, Bruno Palier, Henri Bergeron, Megan Crowley-Matoka, Alex V. Barnard, Arielle Tolman, Christopher Robertson, Nisa Göksel, Elizabeth Onasch, Talia Shiff, four anonymous reviewers, and the ASR editorial team, as well as the Northwestern University Culture and Society Workshop for their valuable feedback on earlier drafts of the article and the larger project. Special thanks to the pain specialists, researchers, patient advocates, and public health officials who shared their time and expertise. A version of this article was presented at the 2019 ASA Annual Meeting in the Regular Session on the Sociology of Technology.
Funding
This research was generously supported by a Graduate Exchange Fellowship with SciencesPo-OSC, a Graduate Research Grant from The Graduate School at Northwestern University, and a Graduate Dissertation Research Travel Award from the Buffett Institute for Global Studies at Northwestern University.