
Abstract
Political leaders play a potentially important role shaping behaviors and beliefs during crises. In the pandemic, a number of high-status politicians, notably leaders of populist parties, were seen to diminish compliance with institutional recommendations by casting doubt on COVID guidelines. But what happens when such leaders change position and endorse previously discouraged behaviors? Using longitudinal data from the Understanding Coronavirus in America panel with fixed-effects modeling, this article examines how Trump’s unexpected endorsement of facemasks in July 2020 affected individuals’ likelihood of wearing a facemask and belief in masks’ efficacy. I find that Trump’s pivot lifted Republicans’ use of facemasks, closing 40 percent of the preexisting gap with Democrats and with stronger effects among individuals who were more exposed to the early-summer spike in COVID cases. Additionally, I provide evidence for the unique significance of this moment in the history of the pandemic, showing that at almost no other time did partisan behaviors converge as sharply. However, in contrast to expectations from most dominant theoretical models of behavioral change, especially the health belief model, no corresponding shift in beliefs about facemasks can be detected. These results have important theoretical implications for understanding how pivots can shape behaviors during crises, the validity of existing models in public health, pandemic populism’s causes, and directions of future research.
Political communication is often considered an important means via which new behaviors and beliefs disseminate throughout society (Clayton et al. 2021; Druckman, Peterson, and Slothuus 2013; Karell et al. 2023; Nzitatira, Billing, and Edgerton 2024), especially in the field of health (Athey et al. 2023; Scheufele 2014; Van Bavel et al. 2024). When politicians get vaccinated on TV, wear a mask, or repeat public health guidelines, they send a powerful signal to followers about the need to adopt new behaviors (Hoffman and Tan 2015). Leaders can seek to support health behaviors’ uptake by encouraging compliance with institutional recommendations, but they can also play a detrimental role when they discredit life-saving medical guidance.
During the COVID crisis, politicians’ ability to shape behaviors became a topic of broad interest. Numerous studies document a strong negative association between support for populist parties—generally early opponents of COVID guidelines—and protective health behaviors’ adoption (Backhaus, Hoven, and Kawachi 2023; Dowd-Arrow, Burdette, and Smith 2023). Moreover, experimental and quasi-experimental evidence indicates that partisan gaps were, at the very least, exacerbated by populist critiques of public health guidance (Ajzenman, Cavalcanti, and Da Mata 2023; Bisbee and Lee 2022; Cherry, James, and Murphy 2021; Dickson and Hobolt 2025; Pink et al. 2021).
But what happens when leaders change position and endorse previously discouraged behaviors? Although largely unstudied, this question has important implications for (1) a sociological theory of the leader-follower relationship, and (2) a practical understanding of how to improve compliance with institutional recommendations during crises. On the one hand, if citizens are rationally ignorant actors (Downs 1957), inflexible and unwilling to digest cues contradicting preestablished choices, then such pivots may be entirely unable to induce behavioral change. Indeed, taking that logic just a step further, one could argue that any observed partisan gap is just a product of similar individuals clustering around political camps. On the other hand, if individuals are, at least under some circumstances, more cognitively flexible agents, open and attentive to cues—as Dual Process Theory (DPT) suggests—then politicians who early-on position themselves against public health recommendations might become important allies in improving compliance if persuaded to alter their stance (Evans 2008; Miles, Charron-Chénier, and Schleifer 2019).
Using Trump’s unexpected pivot over facemasks on July 1st, 2020—when he first endorsed their use, saying he looked like a cowboy while wearing one, specifically the Lone Ranger—I seek to arbitrate between these theoretical narratives in the COVID context. I focus on waves 3 to 8 of the Understanding Coronavirus in America survey, following a panel of 5,159 individuals from April 15th to July 22nd, 2020 (the period between the CDC’s endorsement of facemasks for the public up to Trump’s pivot). Using fixed effects, I compare within-individual trajectories of those who answered just before and after Trump’s interview to estimate this speech’s impact.
To structure this work, I ask three research questions. First, can leaders’ pivots improve protective health behaviors’ uptake? In line with literature on partisan reasoning (Barber and Pope 2019; Brooks and Manza 2013; Lenz 2012), I expect co-partisans (i.e., Republicans), but not opposition partisans, to adjust behaviors in line with a leader’s new cue.
Second, do leaders’ position reversals change beliefs about protective health behaviors’ efficacy? Consistent with the health belief model (Jones, Smith, and Llewellyn 2014; Kasl and Cobb 1966), I start from a view that if leaders can induce behavioral change among followers, they likely do so by changing views about a behavior’s protective efficacy. Nevertheless, I acknowledge a body of scholarship questioning the belief-behavior link (Acharya, Blackwell, and Sen 2018; Verplanken and Orbell 2022) and thus independently assess this mechanism’s validity.
Third, does the crisis context of a pivot moderate its impact? Building on psychological, historical, and cultural accounts of disaster (Lasco and Curato 2019; Marcus, Neuman, and MacKuen 2000; Vaisey 2009), I expect individuals living in areas worse hit by crisis to be more receptive to changing behaviors in response to leaders’ position reversals.
Ultimately, I find Trump’s pivot lifted Republicans’ facemask use, closing the gap with Democrats by around 40 percent. However, I also come to the surprising conclusion that this behavioral shift went unaccompanied by a change in beliefs, a finding seemingly incompatible with most dominant theoretical models for new health behaviors’ adoption. As a partial resolution to this paradox, I show that Trump’s speech had the most effect among Republicans in states worst hit by the early-summer 2020 spike in COVID cases, suggesting his ability to shape behaviors lay not so much in persuasion but in capitalizing on a moment of crisis when individuals were open to adopting novel behaviors.
Taken together, these results have important implications for debates at the intersection of political and medical sociology on pandemic populism’s fundamental causes, especially in the United States. Whereas some have argued that Republicans’ propensity toward low-compliance during the pandemic was indicative of a preexisting medical and institutional distrust (Cole, Schofer, and Velasco 2023; Zapp 2022)—a self-sorting into partisan groups and like-minded communities (Bonikowski, Feinstein, and Bock 2021; DellaPosta 2020; Estep and Greenberg 2020)—my findings suggest the opposite. Namely, Republicans’ low-compliance was to a large extent fueled by thin beliefs built around personal support for Trump (Bisbee and Lee 2022; Kaushal et al. 2022).
Moreover, the unconventional pathway by which Trump induced behavioral change among Republicans opens a wider discussion about how best to communicate with those most resistant to institutional guidance. Much previous work on elite cues assumes rational persuasion is an essential ingredient in changing behaviors (Blair et al. 2021; van Prooijen, Šrol, and Maglić 2025; West and Bergstrom 2021). However, my results bring that argument into question, echoing quantitative (Centola, Willer, and Macy 2005; Kim et al. 2024; Kim and Zuckerman Sivan 2017) and qualitative (Reich 2020; Tavory and Swidler 2009; Urena 2022) sociologists focused on disjunctures between private beliefs and public practices.
It is important to acknowledge that the event this article focuses on took place under specific conditions, a once in a century pandemic, and concerns a leader, Trump, who has perhaps a unique relationship with his followers (Ruisch and Ferguson 2022). Accordingly, this article should not be read as a description of the general case, but rather as the analysis of a significant yet unexplored moment in the pandemic’s history when the partisan divide in an important health behavior shrank substantially, showing how this process challenges existing theory on the link between leaders’ speech and followers’ actions. In so doing, the article highlights a consequential black swan—reflecting calls to pay greater attention to cases focused on extreme or deviant circumstances (Seawright 2016)—that can inform a broader theory of how political communication shapes behaviors during crises.
Political Speech and Human Behavior
Political speech has long been an object of sociological research (Greve et al. 2022; Hahl, Kim, and Zuckerman Sivan 2018; Mueller 1970; Weber [1919] 1946). Yet, across different settings, social scientists continue to debate the extent to which leaders’ cues can shift behaviors (Berman 2021; Druckman 2022). Specific answers are conditional on many elements—context, speakers’ characteristics, cues’ subject (Bullock 2020; Combs et al. 2023)—but at their most basic level, these discussions are all grounded in older disputes around human cognition (Jost, Baldassarri, and Druckman 2022; Taber 2011), with scholarship distributed between two major theoretical narratives.
Classically, dominant theories of the leader-follower relationship, emerging from a Downsian (1957) tradition, dismissed speech’s power to shape action. Beginning from an axiomatic view of cognition—inherited from rational choice theory (Neumann and Morgenstern [1947] 2007; Savage 1954)—this work imagined citizens as rationally ignorant, cognitively automated actors, reliant on sticky preferences to guide action, and discounting counterevidence to established positions. These assumptions implied leaders’ speech could only be a tool to attract followers, a device for citizens to identify who best reflects their views, and thus lacking any margin to affect change (Loewen and Rubenson 2011; Stanley et al. 2020).
Despite early prominence, two strands in the literature challenged the Downsian tradition. First, work demonstrating the degree to which people change behaviors to match those endorsed by authority figures and celebrities provided an indication that something beyond preexisting preferences had to lie behind action (Evans et al. 2014; Haslam and Reicher 2017; Myrick et al. 2024; Pease and Brewer 2008). Second, experimental research showing cues, especially when emotionally charged, could affect reported views and behaviors more directly attacked the self-stabilizing image of cognition underpinning the Downsian model (Ellsberg 1961; Hagmann, Minson, and Tinsley 2024; Kahneman and Tversky 1979).
In response to this mounting evidence, a new family of explanations emerged rooted in Dual Process Theory (DPT). DPT’s innovation was to argue that although people typically rely on automated cognition, certain conditions—potentially including crises—ignite a separate effortful pathway, heightening the attention paid to novel information and thereby elevating susceptibility to cues challenging preexisting habits (Lizardo et al. 2016; Miles et al. 2019). While allowing that individual choice is often stable, DPT provides a more fluid framework to understand how triggering situations moderate cognitive plasticity, opening up or closing down the possibility of shifting practices, even if scholars disagree on how these systems’ interplay ultimately leads to behavioral change (Barone 2025; Evans 2008).
Contemporary research now rarely disputes whether political cues matter in general. But these two models of cognition provide a useful way to understand the core axis around which more recent and contextually focused debates have revolved: placing those emphasizing partisan differences as a byproduct of selection into political camps based on ex ante preferences grounded in sticky cognitive processes (Kteily and Brandt 2025; Leong et al. 2020), against others who contend such divisions can only be fully explained by leaders exploiting more flexible cognitive pathways via speech (Boudreau and MacKenzie 2014; Lilleker 2014).
This basic tension has characterized the COVID literature, especially as it concerns pandemic populism’s origins. In line with the Downsian tradition’s rigid cognitive model, some scholars have asserted populists’ resistance to new health behaviors, such as vaccines, preceded the pandemic (Cole et al. 2023; Kennedy 2019; Zapp 2022), reflecting engrained medical and institutional distrust, linked to underlying skepticism toward science and democratic norms (Brzezinski et al. 2021; Ramirez and Wood 2024).
However, consistent with DPT’s more fluid vision of decision-making, an important literature developed showing populist supporters’ behavioral sensitivity to leaders’ cues. Ajzenman and colleagues (2023), Bisbee and Lee (2022), and Dickson and Hobolt (2025) all demonstrate, with aggregated data, presidential tweets’ capacity to affect social distancing. In survey experiments, Cherry and colleagues (2021) and Pink and colleagues (2021) found that individual acceptance of health behaviors increased when people were exposed to supportive cues from party elites.
Faced with these two seemingly credible narratives, the challenge lies in disentangling their relative importance. Pivots from prominent politicians provide just such an opportunity. By unexpectedly switching from one message to another, pivots represent a shock in the signal sent to citizens, enabling researchers to observe the extent to which previous behaviors are maintained (in line with explanations stressing sticky cognition) and the extent to which behaviors change (consistent with theories emphasizing more fluid decision-making).
Before going down the road of empirics, it is important to establish this article’s own expectations. Coherent with extant research on partisan reasoning (Barber and Pope 2019; Brooks and Manza 2013; Lenz 2012), and more broadly high-status individuals’ role in informing health choices (Hoffman and Tan 2015), I anticipate that co-partisans (i.e., Republicans), but not opposition partisans, will adopt the newly recommended behavior.
Hypothesis 1: Following a pivot by a leader, co-partisans will adjust their behavior to follow the leader’s cue.
Hypothesis 2: Following a pivot by a leader, opposition partisans will not adjust their behavior to follow the leader’s cue.
Doubtless, both speech and selection played a role driving the partisan divide in pandemic health behaviors. However, a recognition of this complexity, far from discouraging investigation, should open a deeper sociological discussion around political speech’s operation, thinking about both mediators and moderators of behavioral change.
Beliefs as a Key Mechanism
Assuming, in line with DPT, that pivots can induce behavioral change, a natural question arises: what is the mechanism by which leaders influence followers’ actions? An obvious explanation is that through position reversals, leaders rationally convince followers of a health behavior’s efficacy. Such a view is consistent with the health belief model (Jones et al. 2014; Kasl and Cobb 1966) and broader theories of Bayesian belief formation often used in political communication literature (Hafer, Izzo, and Landa 2025; Hill 2017), positing that individuals adjust health behaviors as a function of belief in a health threat’s seriousness and the efficacy of a given response. Coherent with this well-established theory, I expect any change in behaviors to be accompanied by a change in beliefs.
Hypothesis 3: Following the endorsement of a health behavior by a leader, co-partisans will adjust their beliefs to follow the leader’s cue.
Hypothesis 4: Following the endorsement of a health behavior by a leader, opposition partisans will not adjust their beliefs to follow the leader’s cue.
At face value, this story appears plausible. If, under some circumstances, individuals become cognitively open to changing behaviors, the same should apply to beliefs. Yet, narratives of behavioral change that assign a central role to beliefs overlook an old but important sociological observation—especially visible in survey research—namely, that individuals often publicly engage in practices they privately are not convinced of (Centola et al. 2005; Kim et al. 2024; Kim and Zuckerman Sivan 2017). From the first-year college student who drinks too much out of social pressure, to the populist voter who knows their leader is a liar while supporting them unquestioningly, scholars have observed, in numerous settings, individuals take up socially expected behaviors contradicting self-reported convictions (Sargent and Newman 2021).
Moreover, such rationally grounded models ignore evidence, particularly from qualitative medical sociology, showing individuals’ capacity to use sophisticated narratives justifying disparities between behaviors and beliefs. Urena (2022) and Tavory and Swidler (2009) show individuals often refuse preventative measures against sexual diseases, despite awareness of their efficacy, for fear of how it will affect intimacy. Reich (2020) identified cases of parents refusing vaccinations for their children, but accepting one themselves if put under sufficient institutional pressure. Noone and Stevens (2008) show a similarly paradoxical relationship studying men’s healthcare utilization, where interviewees emphasize the importance of seeking medical help but do not think these guidelines apply to them personally.
These insights are not incompatible with a DPT framework. However, they force a confrontation with the possibility that beliefs and behaviors operate on separate cognitive pathways—or more radically, in line with habit theory (Acharya et al. 2018; Verplanken and Orbell 2022), that beliefs might actually follow behaviors. This gap between dominant models of behavioral change and the wider pattern of evidence should provoke some reflection concerning the belief-behavior link’s direction and validity. Thus, while I expect beliefs to be a plausible causal pathway, I do not take it as given and I test this proposed mechanism’s credibility.
Crisis as Catalyst
Aside from concerns around mechanisms, it is crucial, given this article’s focus on the pandemic, to address a subject of equal importance: context. DPT holds that the balance between automated and effortful cognition varies according to external circumstances. But how such situational features, particularly crisis conditions, affect the power of cues challenging preexisting behaviors is not a settled issue. Some DPT scholars have thought of crises as catalyzing cognitive fluidity. 1 Perhaps best articulated by Affective Intelligence Theory (AIT), this work argues that by elevating anxiety, crises drive individuals to become information-seeking agents, making them more likely to act on cues contradicting previously established messaging (MacKuen et al. 2010; Marcus et al. 2000).
This psychological theory parallels qualitative historical work exploring how crises legitimize leaders’ power. From the Great Depression to modern terrorism’s rise, social scientists have observed how leaders capitalize on crises to grant themselves normative authority (Lasco and Curato 2019; Matovski 2021; Moffitt 2015), or a rally-round-the-flag effect (Baum 2002). AIT echoes many cultural sociologists’ observation that crises provoke individuals to recombine previous repertoires of action to solve immediate problems (Swidler 1986; Vaisey 2009; Zilberstein, Lamont, and Sanchez 2023). This scholarship implies exposure to crisis will positively moderate pivots’ effects.
Hypothesis 5: Leaders’ pivots will have more effect among individuals living in areas where the crisis has recently been more acute.
However, robust settings to examine how such conditions shape speech’s effects are challenging to find, largely because crisis tends to emerge everywhere all at once. As such, alternative plausible interpretations have arisen, embodied most clearly by System Justification Theory (SJT). Contrasting with AIT, SJT argues that individuals have a level of uncertainty they will tolerate, and if crises push them beyond that point, cognition ossifies—intensifying biases, making individuals more defensive about prior practices, and turning people off new ideas (Bisbee and Honig 2022; Jost 2020).
Without prejudicing one theory over another, these competing conceptualizations of the role of crisis make it an issue worth exploring. Pandemics, due to the geographically uneven nature of their spread, offer a rare instance where it is possible to study how political communication’s effects vary as a function of exposure to an underlying threat, providing an analytically useful setting to test competing accounts of crisis within DPT.
The Lone Ranger Interview
To examine these theoretical claims in the COVID setting, I exploit Trump’s unexpected pivot over facemasks on July 1, 2020, when he first endorsed their use. To contextualize this event, it is useful to revisit facemasks’ political history in the United States during the pandemic. Initially, the U.S. government recommended that non-medical personnel not use masks, motivated by the need to reserve stocks (Terry 2020). However, on April 3, 2020, responding to new evidence, the CDC changed its position to recommend non-medical personnel wear cloth facemasks (Goldberg et al. 2020).
The next day at his press conference, Trump reported the change in guidance but refused to endorse the policy or confirm he would wear one, saying, “This [wearing a facemask] is voluntary. I don’t think I’m going to be doing it” (Smith 2020). Over the following weeks, Trump’s initial reticence was reinforced by repeated opposition from Trump surrogates to facemask use and Trump’s persistent refusal to wear a mask in public (Young et al. 2022).
During a sharp rise in cases during early-summer 2020—with new daily cases doubling from 20,000 to 40,000 from the beginning to the end of June (see Figure 1)—Trump unexpectedly changed position in an interview with Fox News on July 1, 2020. Asked by the interviewer whether he would wear a facemask, Trump responded, “I’m all for masks. I think masks are good. . . . Actually I had a mask on, I sort of liked the way I looked. . . . It was a dark black mask and I thought I looked ok, I looked like the Lone Ranger.” 2 For context, the Lone Ranger was a popular fictional cowboy, prominent in the mid-twentieth century.
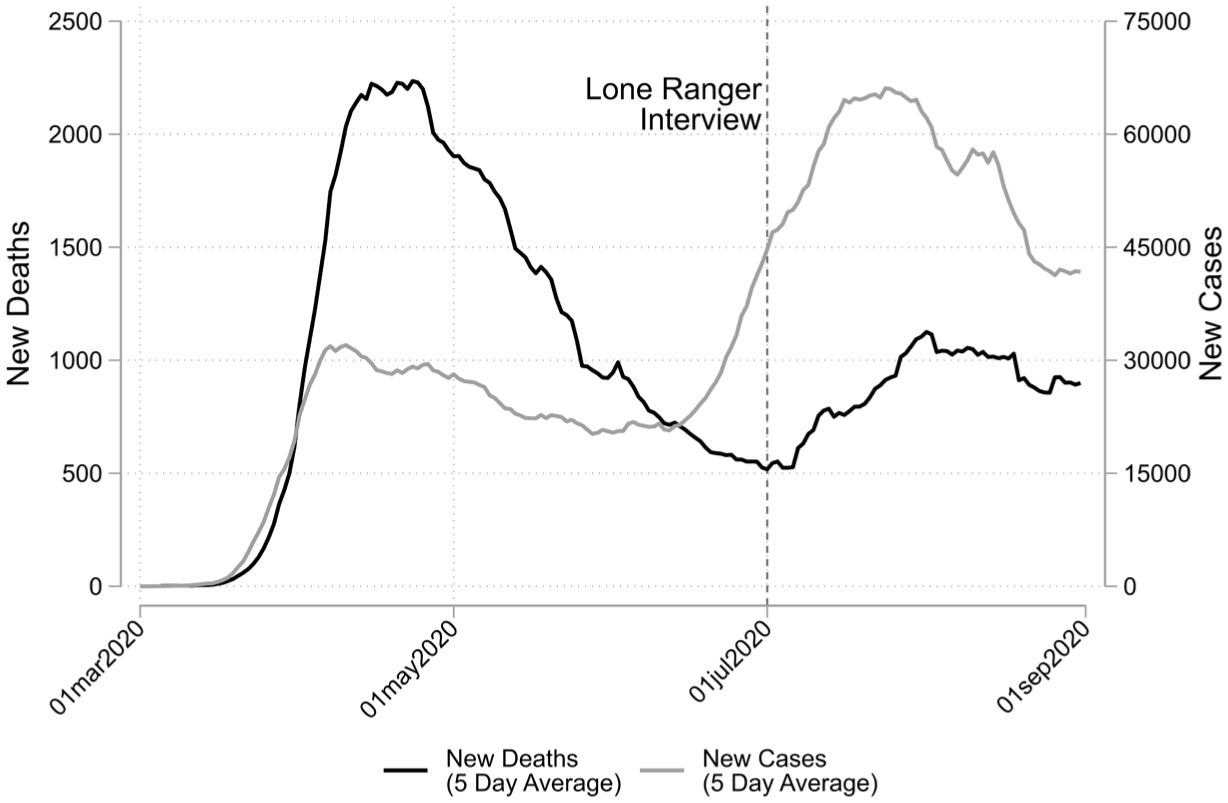
Trends in New COVID-19 Cases and Deaths in the United States between March 1 and September 1, 2020
Trump’s Lone Ranger interview offers a useful setting to study the effects of leaders’ pivots on health behaviors for three reasons. First, the event’s novelty—this was the first time Trump publicly supported mask-wearing—provides the best opportunity to examine a position reversal. This contrasts with other work, notably Bisbee and Lee (2022), that uses later events, such as Trump’s first tweet in support of facemasks.
Second, Trump’s position reversal was unexpected and seemingly spontaneous. There are no signs of prior briefing to media or anticipation that Trump would endorse facemasks, thus creating the cleanest conditions to estimate such a pivot’s effects.
Third, unlike work using survey experiments (Cherry et al. 2021; Pink et al. 2021), exploiting this event allows for the assessment of a leader’s cue when participants cannot be obliged to watch the cue itself. This enables me to provide an estimate reflecting that (1) many individuals may not take note of the cue, and (2) those who do take note may not be influenced by the cue itself, but rather by media reporting on the cue. Thus, this work provides a realistic evaluation of a leader’s position reversal, rather than showing the effect of watching a speech.
Data and Methods
Understanding Coronavirus in the United States
I use data from Understanding Coronavirus in America (UCA), an extension of the Understanding America Study, a longitudinal online panel following a nationally representative sample of 14,000 U.S. residents since 2014 (Alattar, Messel, and Rogofsky 2018), chosen via address-based sampling. UCA was based on a smaller fixed-panel of 8,815 respondents, following the same individuals across waves (with each individual limited to one response per wave), resurveyed at roughly two-week intervals, with a response rate of around 82 percent. UCA provides a rich source of questions on pandemic behaviors and beliefs, supplemented with previous waves of the Understanding America Study covering a range of political and demographic features.
UCA did not ask about partisanship. However, in Understanding America’s 2019 End of Year Survey, individuals’ partisanship was recorded based on the following question: “Regardless of if or how you are registered to vote, are you more closely aligned with . . .” Respondents were coded as Democrat, Republican, or other. Given partisanship’s importance to this work, only individuals responding in UCA and the 2019 End of Year Survey are used.
In order that all pre-treatment periods took place when there was a dissonance between Trump’s position over facemasks and the broader administration, I only use waves fielded after the CDC endorsed facemasks on April 3, 2020; waves 1 and 2 are thus excluded. Wave 7 is also excluded because the tail-end of responses overlaps with Trump’s pivot. To help visualize these choices and the broader data structure, Figure 2 shows the distribution of observations within and between waves across calendar dates.
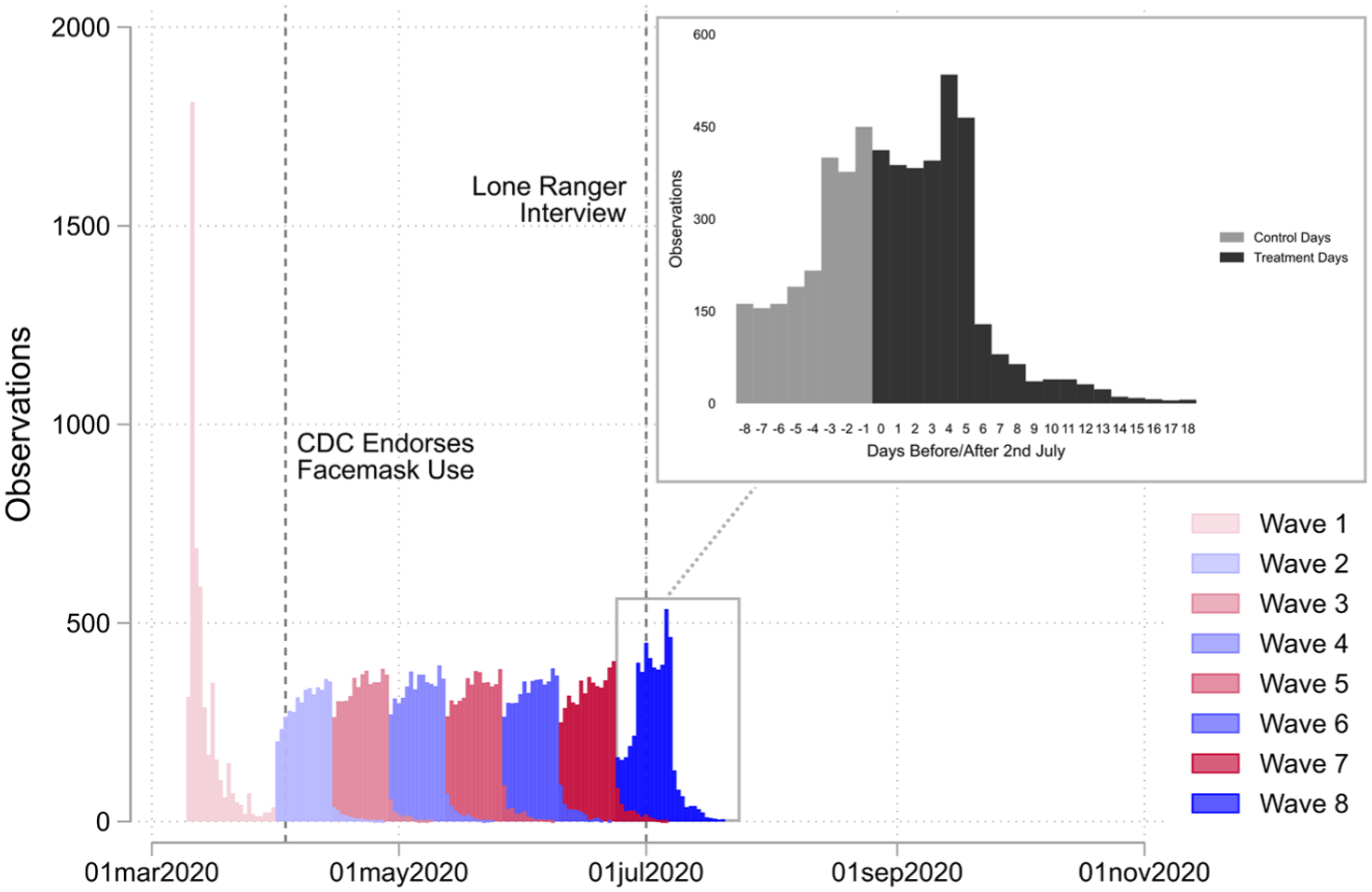
Distribution of Responses Across Waves 1 to 8
The main estimation thus focuses on five waves, treating waves 3 to 6 as pre-treatment periods and wave 8 as a post-treatment period, leaving a final sample of 5,169 individuals who collectively have an extremely low attrition rate (with 89 percent of respondents answering in all five waves and 96 percent answering in four or more waves). For a full calendar including attrition rates, see Table 1A in the online supplement. Unweighted baseline characteristics are shown in Table 1.
Unweighted Baseline Sample Characteristics
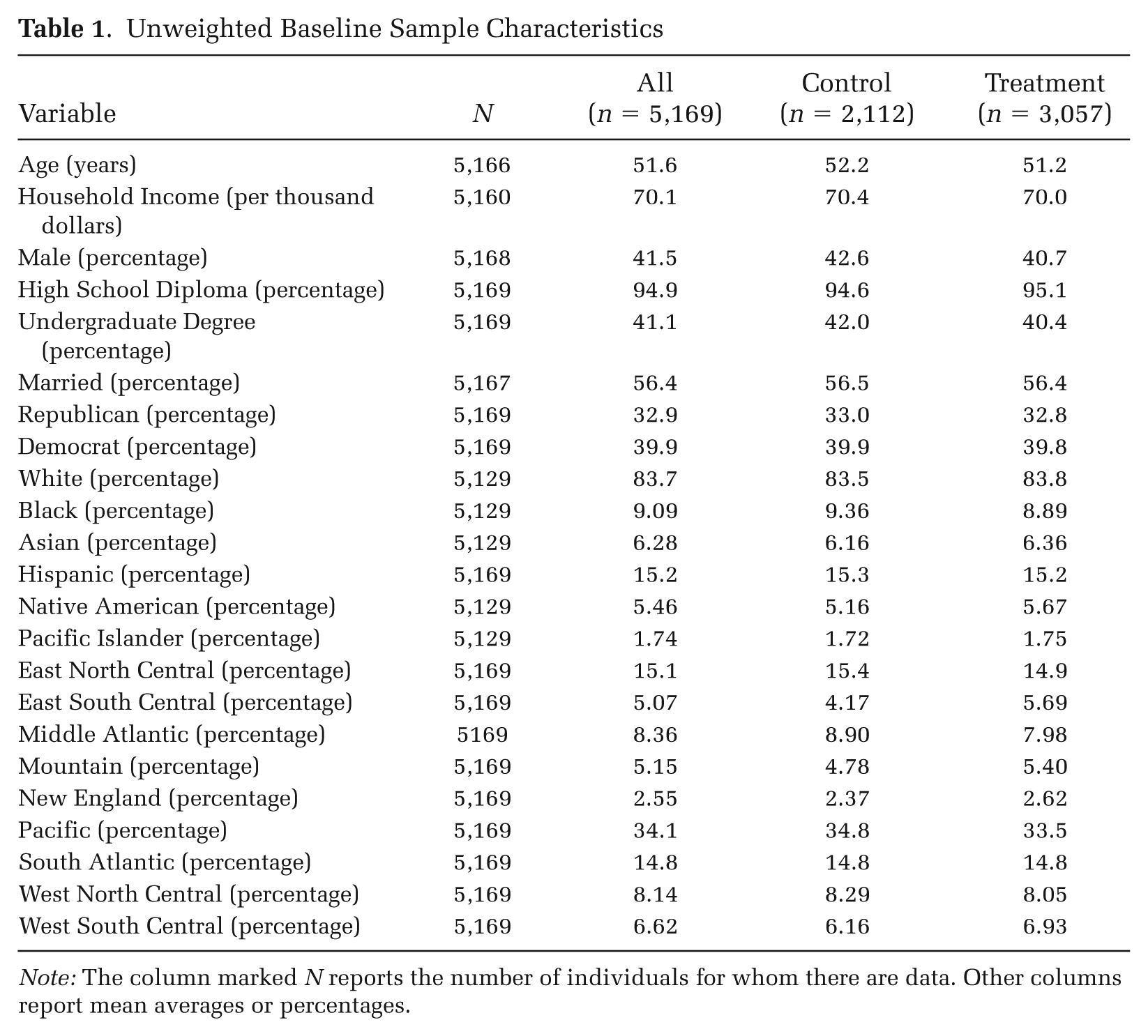
Note: The column marked N reports the number of individuals for whom there are data. Other columns report mean averages or percentages.
Dependent Variables
This article’s first dependent variable is a self-reported indicator of whether a respondent wore a facemask in the last week. Respondents were asked, “Which of the following have you done in the last seven days to keep yourself safe from coronavirus in addition to what you normally do? Only consider actions that you took or decisions that you made personally. Worn a face mask.” Respondents answered either “yes” (coded 1) or “no” (coded 0).
To assess health beliefs, a binary variable was coded indicating whether participants thought facemasks were an effective protection against COVID-19. Respondents were asked, “How effective are the following actions for keeping you safe from coronavirus? Wearing a face mask such as the one shown here,” with an image of an N95 facemask next to the question. Respondents who answered “extremely effective” or “somewhat effective” were coded 1. Those who answered “unsure,” “somewhat ineffective,” or “extremely ineffective” were coded 0.
To provide an overview of how these variables evolved, Figure 3 shows the average for each outcome by wave and partisanship. Waves 1 to 25 of UCA are all shown in Figure 3 (covering March 10, 2020 to March 29, 2021) to give a sense of how beliefs and behaviors developed pre and post Trump’s interview in wave 8. Following wave 8, when Trump pivoted, Republicans’ probability of wearing a facemask jumped sharply, by around 0.05, and remained above where it had previously been. Yet, belief in masks’ efficacy plateaued and even went into a slight decline. This is just a descriptive picture, but it already points to an important behavioral shift around Trump’s speech that was not accompanied by a change in beliefs.
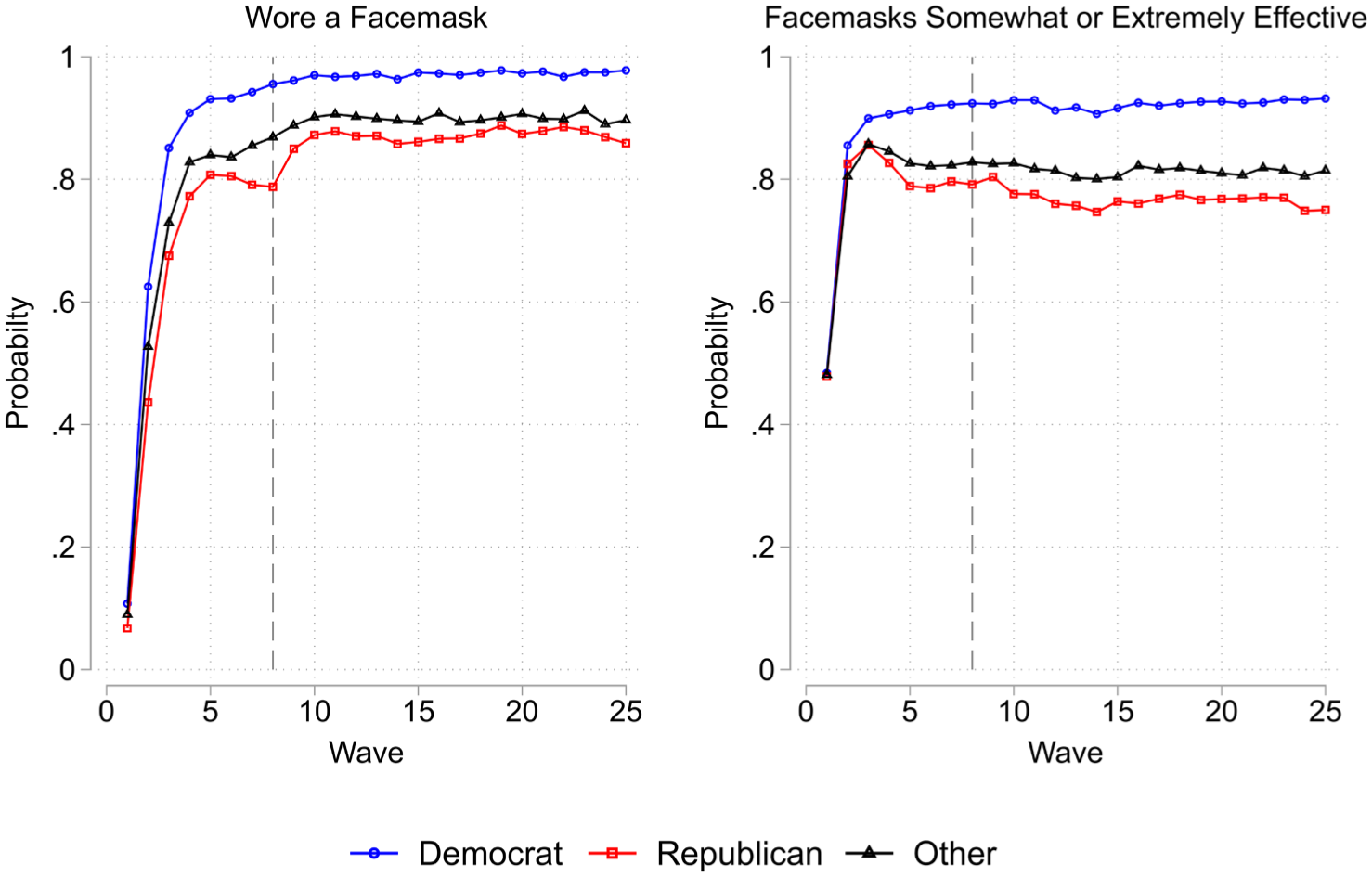
Probability of Wearing a Facemask and Belief in Facemasks’ Efficacy by Wave and Partisanship
Independent Variables
To evaluate the Lone Ranger interview’s effect, I coded a dichotomous variable D into the data, indicating whether in wave 8 respondents answered before or after Trump’s pivot. Respondents who answered on or prior to July 1, 2020, in wave 8 are coded 0 in every wave. Participants who answered after July 1, 2020, in wave 8 are coded 1 in every wave. This variable assigns individuals to control and treatment groups based on the cutoff between July 1st and 2nd, assuming those responding after July 1 would have been exposed to Trump’s speech, and those who answered beforehand would not.
As I am also interested in the epidemiological condition’s moderating role, I use a continuous variable, summer shock, recording the relative rise in cases at the state level in the build-up to Trump’s pivot. Employing weekly CDC data, I calculated the relative change in new cases between the first and last week of June for each state and Washington, DC. To provide a sense of how the June rise in cases varied, Figure 4 shows the percentage change in new cases between the first and last week of June by state. These data were merged into UCA by state of residence, standardized, and mean-centered around 0. Importantly, the summer shock variable is time-invariant: it records the severity of the sudden rise in cases during June 2020 between states, not how the epidemiological situation was evolving.
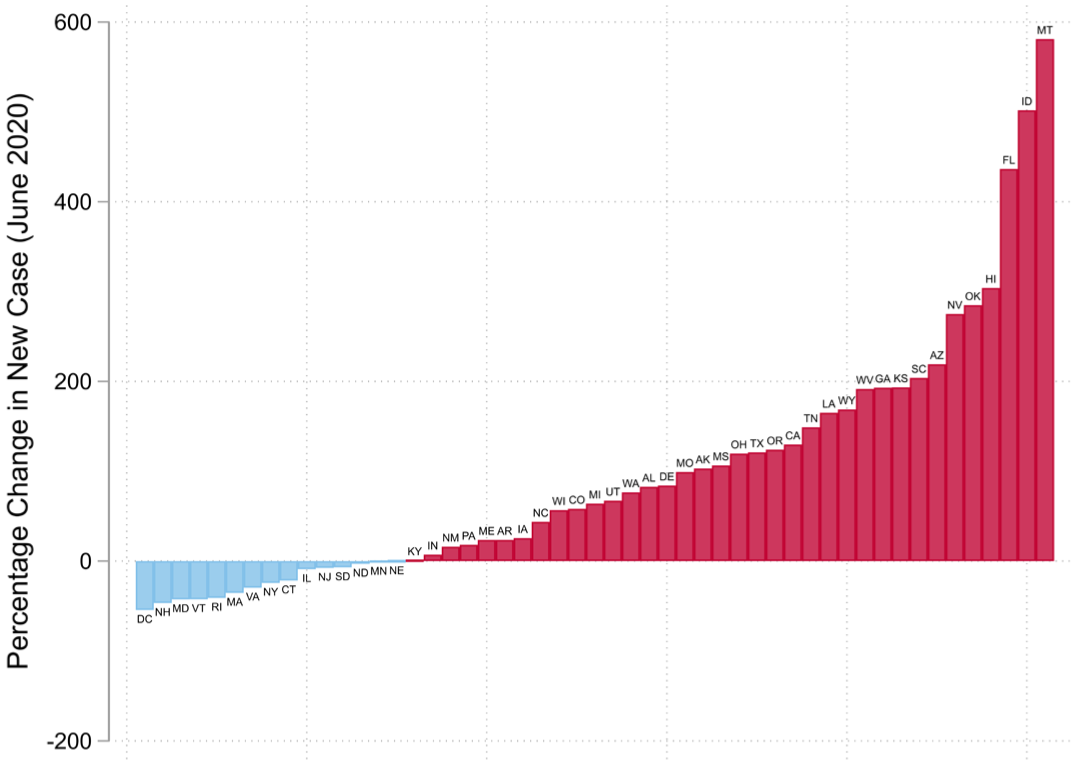
Percentage Change in New COVID-19 Cases between First and Last Week of June 2020
Additional controls account for (1) local policy differences, (2) evolving risk-perception, and (3) differences in exposure to COVID-19. First, to account for differences in state-level mask mandates, I include a binary indicator, based on the Oxford COVID-19 Government Response Tracker (Hale et al. 2021), coded 1 if a respondent’s state of residence had a compulsory mask ordinance in place on the day of their response and 0 otherwise. Second, to evaluate risk-perception, I include two items asking participants to assess their risk of infection from COVID-19 and dying from COVID-19 (in percentage terms). Both variables are normalized between 0 and 1. Finally, I use a dichotomous variable to indicate if individuals had been diagnosed with COVID-19, equal to 1 if they had received a positive diagnosis and 0 otherwise. Table 2 presents summary statistics.
Descriptive Statistics
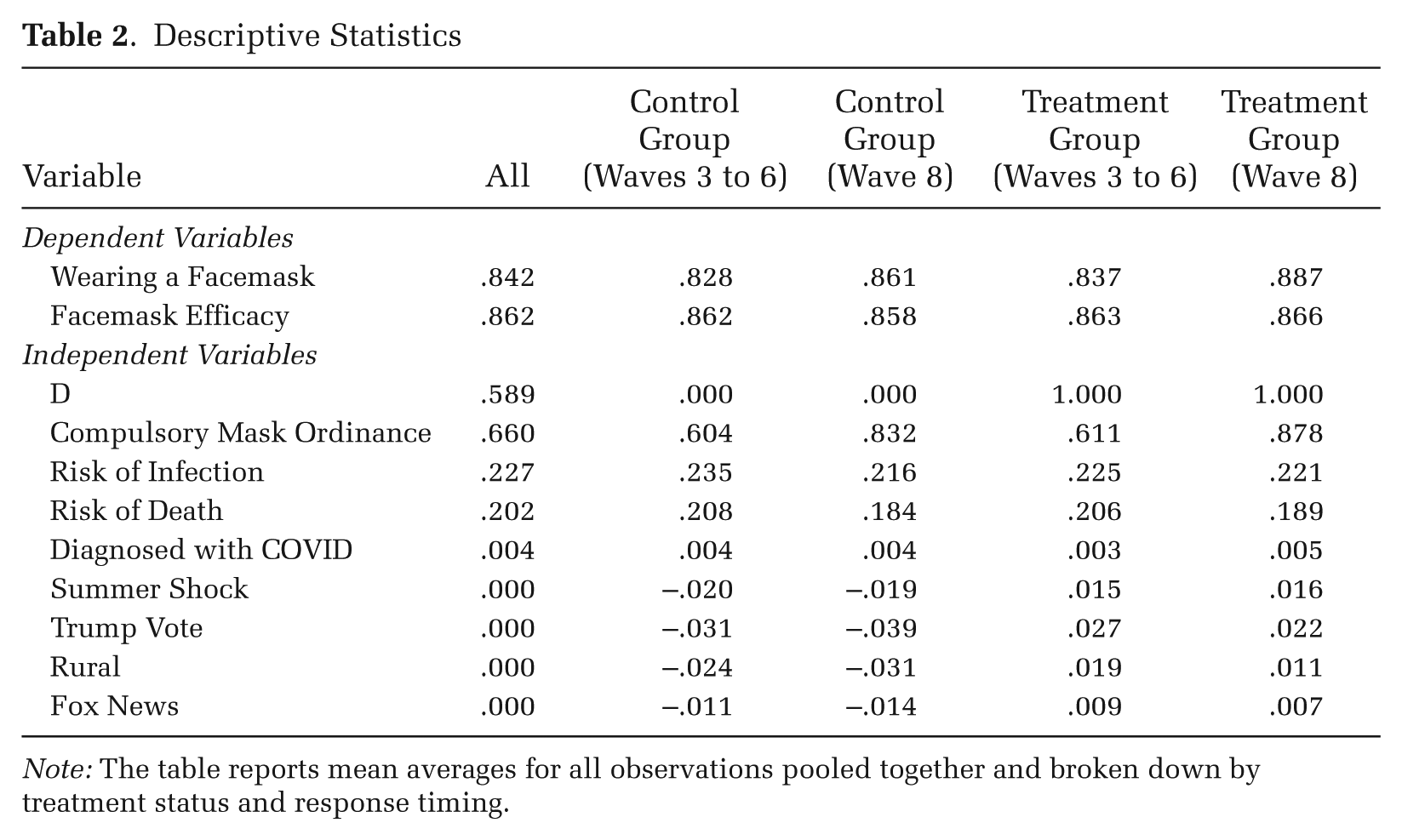
Note: The table reports mean averages for all observations pooled together and broken down by treatment status and response timing.
Although not used in the main estimation, I include a series of state-level variables to test the robustness of the local epidemiological condition’s moderating role. Looking at the rise in cases during June 2020, it appears that more conservative and rural states experienced the brunt of the epidemiological crisis. Therefore, to account for other elements of the political, media, and demographic environment, I consider three further variables: (1) the proportion of individuals who voted for Trump in the 2016 presidential election (Trump vote); (2) the proportion of individuals living in rural areas in 2020, based on U.S. Census estimates (rural); and (3) Google Trend Interest Scores for Fox News during June 2020 (Fox News). 3 All three are standardized and mean-centered around 0.
Analytic Strategy
I aim to evaluate three relationships in this article: first, the association between Trump’s pivot and masking behaviors; second, the mediating role of beliefs about masks’ efficacy; and third, the extent to which crisis conditions (i.e., rising cases) moderate the effect of Trump’s intervention. Figure 5 provides a graphic summary.
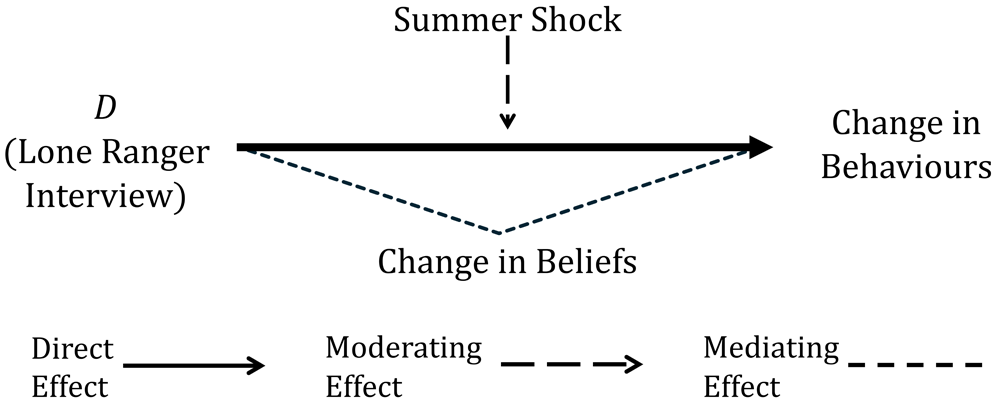
Directed Acyclic Graph of Hypothesized Relationships
Concerning the first two relationships, the most common approach to estimating the effect of a similarly large, one-off event such as Trump’s pivot would be a between-group comparison, similar to a regression discontinuity (RD) design (Flores 2018; Frey 2022; Legewie 2013; Roman and Thompson 2025; Wimmer et al. 2025). Here, the key idea is that if event D takes place mid-survey, its effect can be estimated by comparing the difference in outcome y between individuals i who answered just before and after the event, assuming response timings are exogenous. For this study, the assignment rule can be expressed as follows:
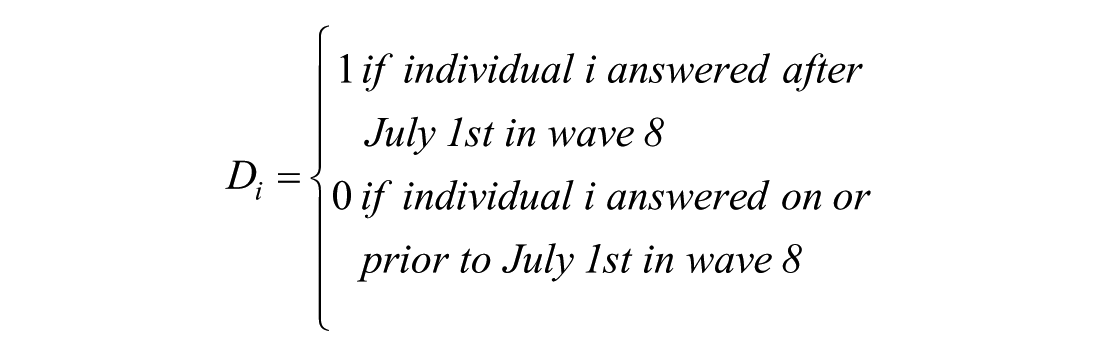
Although a powerful technique, such cross-sectional RDs have a limited ability to account for unobserved sources of bias, especially at the individual level (Kreiss and Rothe 2023). In this case, such designs would not account for the prior gap in mask use or belief in masks’ efficacy between respondents who answered pre and post Trump’s pivot.
Therefore, I propose an extension to the RD approach, exploiting UCA’s panel structure (in which the same people are observed over multiple waves) with fixed effects, to explicitly model changes both between groups (i.e., respondents who answered pre versus post Trump’s pivot in wave 8) and within individuals over waves. By holding D’s value constant for individuals across waves, the effect of Trump’s pivot can be recovered with a two-way interaction, comparing the within-individual change from prior waves (which could not have been affected by Trump’s pivot [waves 3 to 6]) to the wave when the event took place (wave 8), between individuals who answered just before and after the intervention in wave 8, and (in this case) limiting that comparison to respondents who live in the same state, reflecting states’ fundamentally divergent trajectories across the course of the pandemic (Grossman et al. 2020). This approach, which constitutes the article’s preferred specification, can be summarized with the following linear probability model (LPM):

where i is individual i, t is wave t, d is calendar date d, and s is state s. β estimates the effect of Trump’s Lone Ranger interview.
As an aside, I favor LPMs over alternatives such as logit models for two reasons. First, such alternatives do not allow for easily interpretable comparisons when stratifying by subgroup (Mood 2010), a mainstay of my later analysis. Second, logit FEs effectively exclude units if the outcome is constant (Beck 2020). Given my interest in assessing change versus stability, such techniques would undermine the strategy’s central theoretical motivation.
Returning to the main approach, this specification’s validity hinges on three assumptions. First, in the absence of Trump’s intervention, respondents who answered pre and post his pivot in wave 8 should have evolved similarly between waves (i.e., the parallel trends assumption). Second, assignment to treatment should be exogenous, that is, there should be no systematic reason respondents answered before or after Trump’s interview. Third, there should be no confounder correlated with the treatment. In particular, no other event should have occurred during the period of time being examined in wave 8 that would bias results.
To identify potential violations of parallel trends, in addition to the static specification, I also provide dynamic estimates. This allows for an intuitive evaluation of parallel trends using relative lags to examine if the two groups evolved similarly prior to wave 8. I also ran a battery of post-estimation tests, outlined in the results sections.
Two pieces of evidence suggest that assignment to treatment was exogenous. First, as seen in Table 1, control and treatment groups have similar compositions in terms of time-invariant characteristics. Second, when examining the distribution of responses across wave 8 (see Figure 2), it is clear the frequency of answers was evolving smoothly between July 1st and 2nd, suggesting no manipulation around the cutoff.
Finally, given UCA’s long collection periods, often running for a month, it seems improbable that no other relevant event would have occurred during wave 8 when using the whole sample. Therefore, in the main results, the estimation only uses individuals who answered tightly around the cutoff between July 1 and 2, 2020. As in all sharp cutoff designs, there is a trade-off in setting this bandwidth between including more observations for greater precision and imposing tighter restrictions, making the underlying assumptions more plausible.
The online supplement shows the specification run with several selections, but in the main results, the bandwidth is set to +/– 3 days around the cutoff, that is, respondents who in wave 8 answered between June 29 and July 4. There are at least two reasons to make this selection. First, this choice approximates the optimal bandwidth obtained using Calonico, Cattaneo, and Farrell’s (2020) procedure for a cross-sectional RD (h ≈ 2.8 days). Second, this selection avoids a number of other events that might affect participants’, especially Republicans’, behaviors and views around facemasks (e.g., Pence’s endorsement of facemasks on June 28 [Kelley 2020] and later interventions by Trump, such as his first television appearance with a facemask on July 11 [Egkolfopoulou 2020]).
Next, I turn to the third relationship, that is, the moderating role of epidemiological conditions. To that end, it is possible to extend the previous specification to a three-way interaction, an approach that can be summarized as follows:
Three-way interactions can be difficult to decipher. However, the use of state-wave fixed effects allows for a simple explanation. In essence, this specification performs two calculations simultaneously. First, it computes an estimated effect for Trump’s pivot for each state, using the same method as before. Second, it makes a weighted comparison between states, testing whether the effect of Trump’s pivot is systematically larger or smaller as a function of the summer shock variable, and if so by how much.
As such, the model’s coefficients assume a straightforward interpretation. β1 estimates how much more or less of an effect Trump’s intervention had for every one-standard-deviation increase in the summer shock variable. β2 provides an estimate for the effect of Trump’s intervention when the summer shock variable is equal to 0 (i.e., at the mean). As they are perfectly colinear with the fixed effects, I do not include separate terms for the summer shock variable, its interaction term with wave 8, and its interaction with the treatment D.
Trump’s Pivot and Facemask Use
In this section, I report estimates for Trump’s pivot, stratified by partisanship, on respondents’ reported use of facemasks (see Table 3). When all participants are included, Trump’s intervention had no significant effect. But when only Republicans are used, Trump’s pivot is associated with a 0.05 increase in the probability of facemask use, with no substantial change including or excluding covariates. Table 1B in the online supplement presents results without individual or state-wave fixed effects, arriving at substantively the same results.
Static Results for Wearing a Facemask Stratified by Partisanship
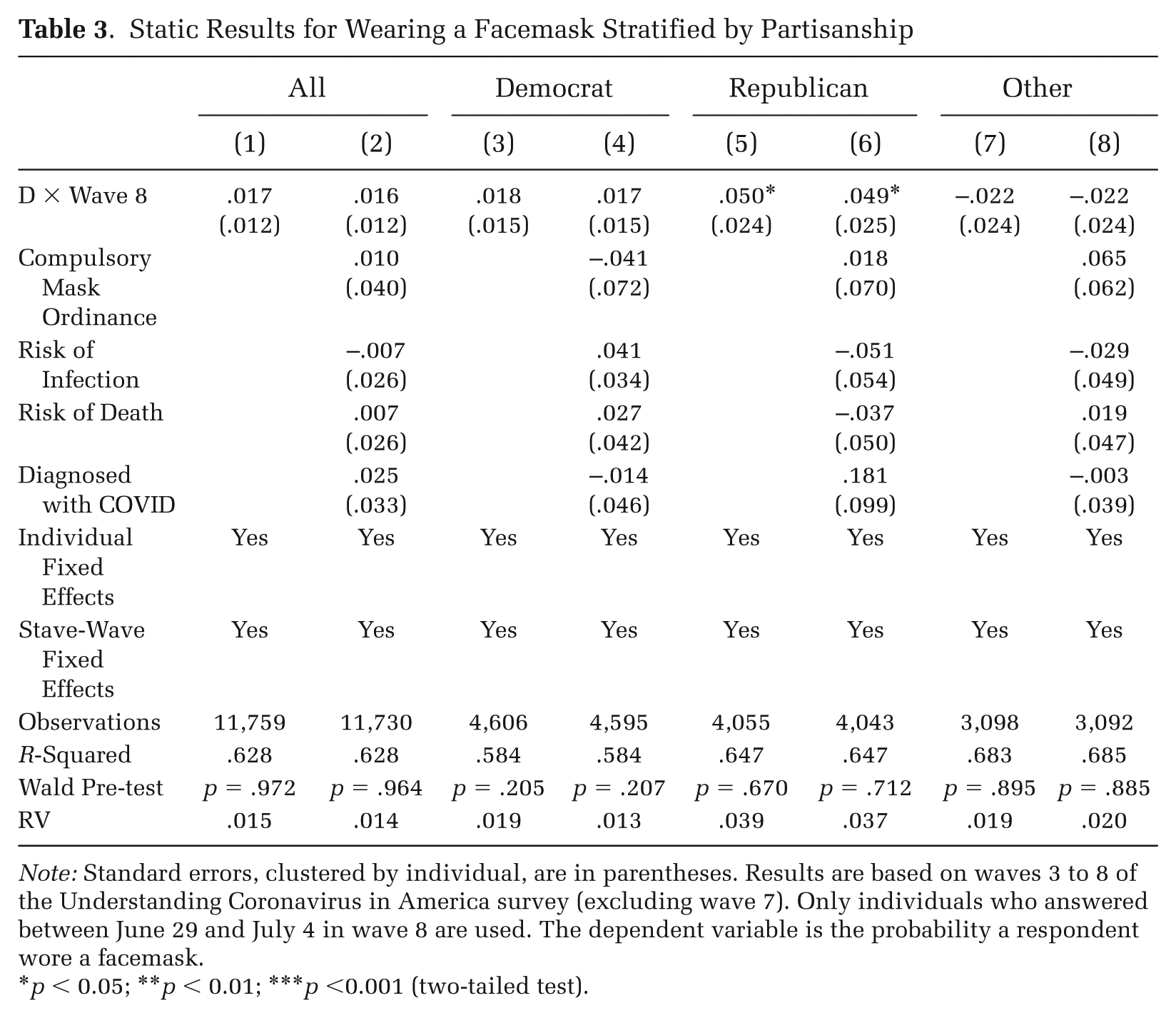
Note: Standard errors, clustered by individual, are in parentheses. Results are based on waves 3 to 8 of the Understanding Coronavirus in America survey (excluding wave 7). Only individuals who answered between June 29 and July 4 in wave 8 are used. The dependent variable is the probability a respondent wore a facemask.
p < 0.05; **p < 0.01; ***p <0.001 (two-tailed test).
To contextualize this effect’s magnitude, it is helpful to consider the baseline partisan divide in mask use. In wave 6, conducted about a month before Trump’s speech, Republicans’ probability of wearing a mask was 0.12 lower than Democrats’ (see Figure 3). Hence, a back of the envelope calculation suggests Trump’s intervention, at least in the short-term, closed 40 percent of the preexisting Republican–Democratic gap. These results imply that even if the absolute effect size is small, Trump’s pivot greatly reduced partisan differences.
The online supplement provides results across different bandwidths (see Tables 2B to 5B). For all selections, Trump’s intervention led to a significant rise in Republicans’ mask use, although effect sizes are larger at tighter bandwidths, ranging from 0.12 (+/– 1 day) to 0.05 (+/– 7 days).
To formally test if Republicans reacted differently to Trump’s pivot, a three-way interaction is estimated in the online supplement, where all individuals are included, and a dichotomous variable for being a Republican is used as the third difference (see Table 6B). Generally, we see a significant difference between Republicans’ reaction versus other groups. I also ran this specification looking only at Republicans and Democrats and obtained almost identical effect sizes, although at tighter bandwidths significance is harder to achieve due to small sample sizes (see Table 7B).
Analytic Threats and Robustness Checks
Although seemingly robust, it is important to consider threats to the analysis. Therefore, I conducted a number of additional checks to respond to the three largest potential concerns.
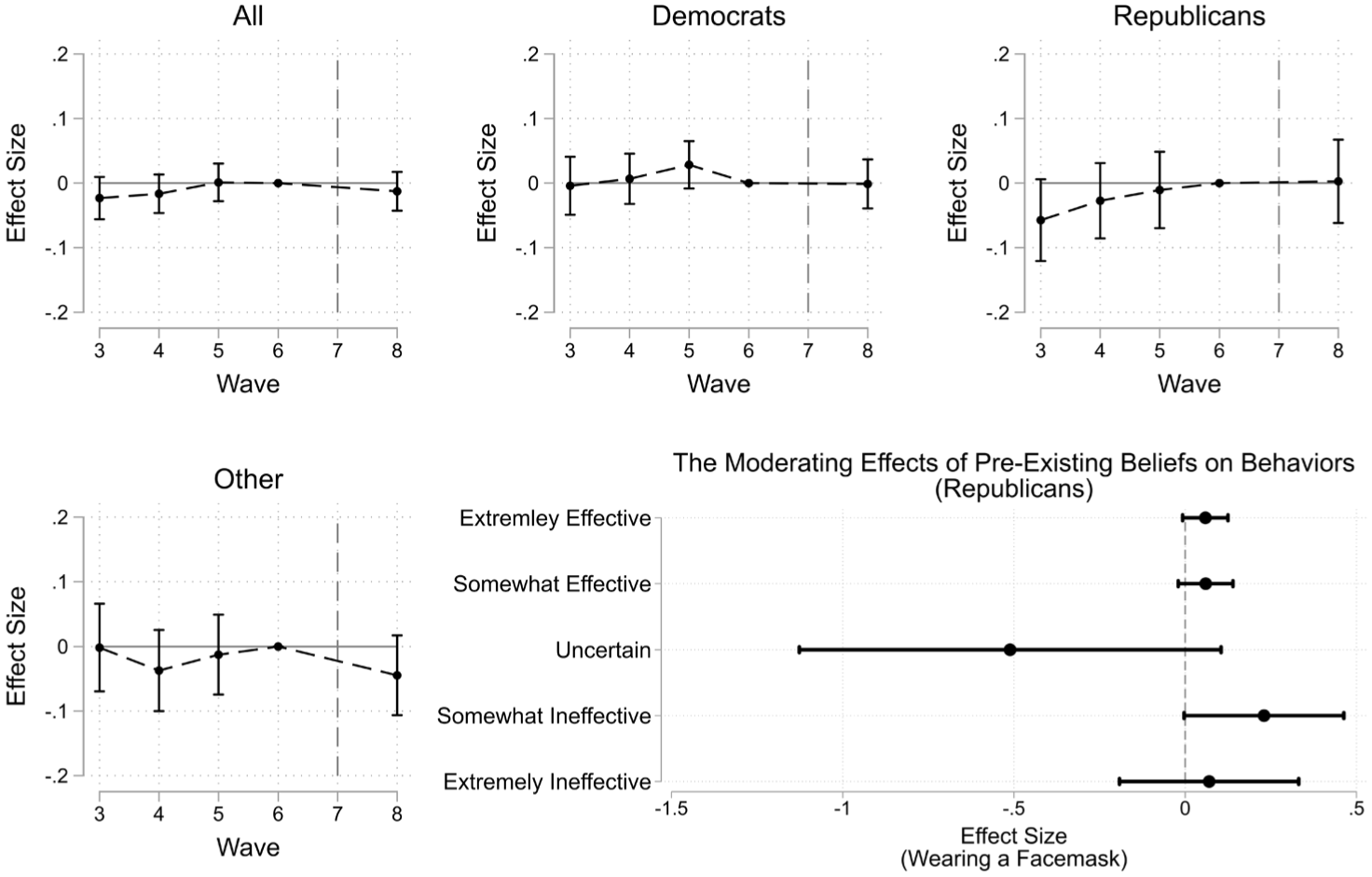
(1) Results could be sensitive to violations of the parallel trends assumption. As an initial test, I estimated a dynamic specification to see if there are obvious violations in relative lags (see Figure 6). Among Republicans, there was no significant difference in control and treatment groups’ evolution prior to wave 8, suggesting, on first appearance, there is a reasonable case for parallel trends.
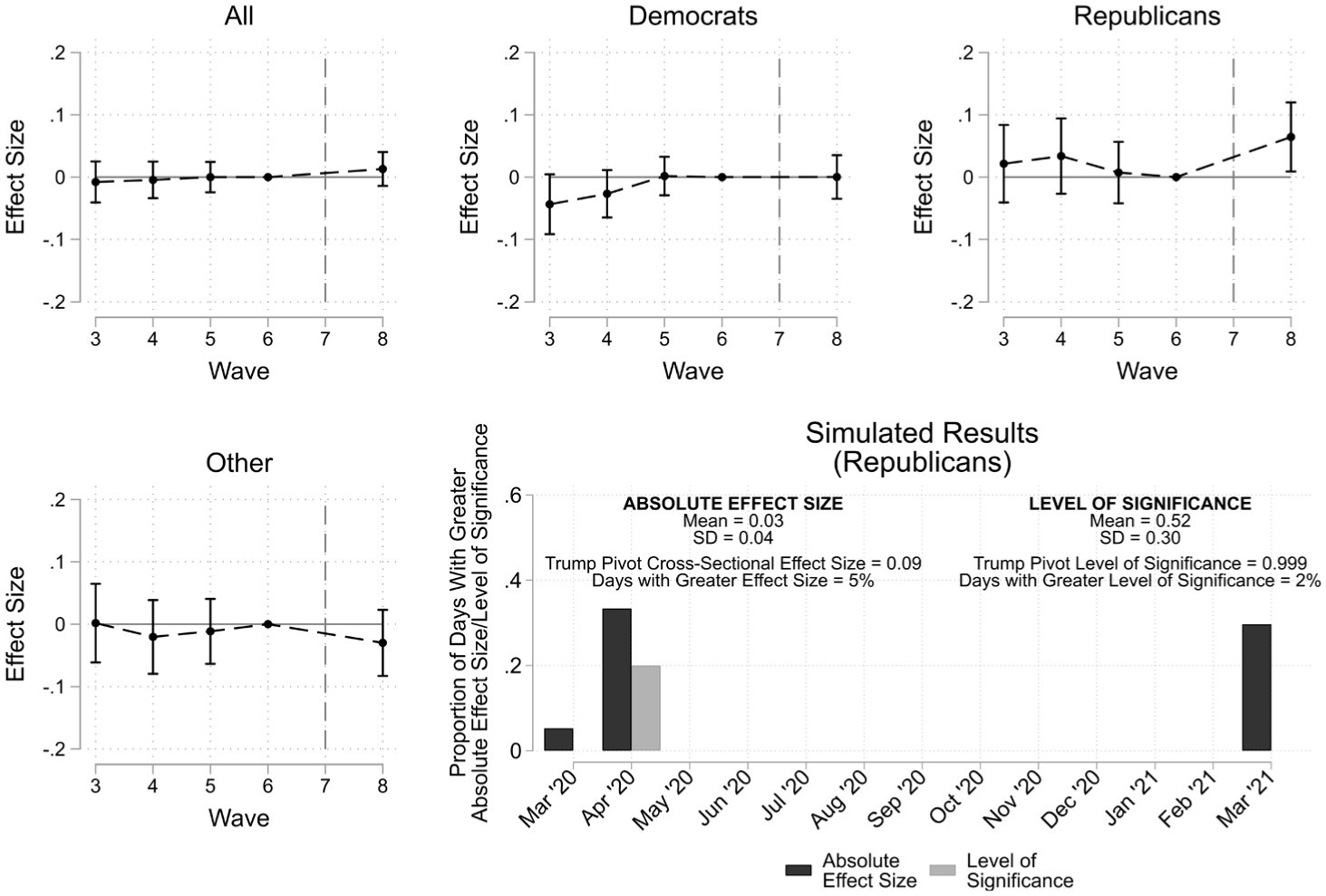
Dynamic Results for Wearing a Facemask, Stratified by Partisanship and Summary of Simulated Results
Individual lags may be underpowered to detect violations. Thus, I ran a Wald test of joint-nullity on pre-treatment lags (i.e., dynamic estimates from waves 3, 4, and 5). This test evaluates the null hypothesis that pre-treatment estimates do not significantly diverge from zero pooled across waves. In no model is the null hypothesis rejected, further supporting parallel trends.
As an alternative evaluation of parallel trends, I conducted a series of placebo tests modeling pre-treatment periods as post-treatment periods. First, the data are restricted to waves 3 to 6, and wave 6 is modeled as the post-treatment period; the same procedure is repeated using wave 5 and then wave 4 as post-treatment periods. The idea behind this test is that if violations are present, similar positive results should be found during periods before Trump’s pivot. Ultimately, placebo tests do not reveal significant violations (see Table 8B in the online supplement).
I also ran models using trajectory balancing, reweighting treatment and control groups to enforce balance on the outcome in waves 3 to 6. I used two different procedures, mean and kernel weighting (see Hazlett and Xu 2018), both with individual and wave demeaning. If pre-treatment differences are biasing results, trajectory balancing should produce substantively different findings. In the end, these procedures find similar estimates (see Table 9B in the online supplement).
(2) Results could be biased by confounders correlated with treatment. Most obviously, this could happen if other cues took place close to Trump’s pivot. To address this threat, I ran the same specification keeping the bandwidth at +/– 3 days but moving the cutoff to other dates in wave 8 (see Tables 10B to 13B in the online supplement). The intuition is that if such cues exist, similar discontinuities should appear at alternative cutoffs. In general, results are not significant at other dates. In one instance, it seems as if results might be significant for Republicans at another cutoff, but these results are not robust to tighter bandwidths, suggesting it should not be a source of concern (see Table 14B).
There may also be other unobserved channels via which confounders are introduced. In response to this concern, I report Cinelli and Hazlett’s (2020) robust value (RV) statistic for the main specification and results from different bandwidths, computing the strength of association required between the interaction and a confounder, in terms of partial R², to produce an effect of 0. At wider bandwidths, potentially weak confounders (explaining just 3 to 4 percent of residual variance) could produce such results. Although even this level is relatively robust: for example, at +/– 3 days, such a confounder would need to be 37 times more strongly associated with the interaction than a COVID diagnosis, the covariate with the largest impact, to produce an effect of 0 (see Table 15B in the online supplement). At tighter selections this risk is reduced, with a confounder needing to explain 9 percent of residual variance at +/– 1 day. Therefore, it seems unlikely such substantial factors could emerge without detection.
(3) I made a pragmatic choice to exclude waves that posed problems for the integrity of the analysis. I excluded waves before the CDC’s endorsement of facemasks (waves 1 and 2), and I removed wave 7 due to late responders bleeding into wave 8 past Trump’s pivot. To show these choices did not bias results, I explore what happens if these data are reintegrated. Using the full set of waves 1 to 8, I constructed a new sample where individuals are excluded if in wave 7 they answered after the first day of wave 8 (June 24, 2020). I then re-estimated the specification, including and excluding waves 1 and 2.
Estimates with this new sample produce similar findings (see Table 16B in the online supplement). However, examining Wald pre-tests, the inclusion of waves 1 and 2 (in which late responders were more likely to be exposed to the CDC’s facemask endorsement) weakens parallel trends, especially among the politically unaligned. To demonstrate that the imbalance generated by including these waves does not change results, I provide estimates using trajectory balancing on waves 1 to 7, showing broadly equivalent effects (see Table 17B in the online supplement).
Simulation of Fictitious Events
Even with the checks outlined above, there may still be concerns over these estimates’ validity and, perhaps more importantly, their scientific relevance. The most significant issue is that because the specification focuses on a particular moment in time, I may be ignoring other substantial events, especially further out from the Lone Ranger interview and possibly from other actors, which could affect Republicans’ propensity to wear masks.
Of course, it is difficult to account for every event affecting Republicans’ mask use. However, taking inspiration from Legewie (2013), it is possible to estimate the likelihood that an event of a similar magnitude could appear at random. To do so, I adopt a more straightforward estimation strategy: maintaining a bandwidth of +/– 3 days, I estimate a series of cross-sectional LPMs, for Republicans, with a pre/post dummy, without fixed effects or controls, for all 379 cutoffs of waves 1 to 25 of UCA for which there is sufficient data (i.e., March 13, 2020 to March 27, 2021, inclusive) to see if there is any date when a larger discontinuity can be observed.
The simulated results are summarized in the graph on the bottom-right of Figure 6. The y-axis shows the proportion of days (in each month) with a larger absolute effect size and a greater level of significance (i.e., 1 minus the p-value) than setting the cutoff at July 1st/2nd. Overall, this exercise demonstrates that few alternative cutoffs produce larger effects or greater levels of significance. The chance of randomly picking a day with a greater discontinuity or level of significance is about 0.05 and 0.02, respectively. Moreover, all cutoffs with larger discontinuities appear at the very beginning or end of the pandemic, in March and April, suggesting similarly important events, which could bias results, are unlikely to have occurred, especially during the middle period of the pandemic, the focus of this study.
These findings not only emphasize the uniqueness of Trump’s Lone Ranger interview, but also go to support this article’s core assumptions. If the timing of survey responses were not exogenous or if the discontinuity in mask-wearing were part of some broader trend, similar discontinuities should be observable throughout. However, the relative stability in the outcome should provide further confidence in the initial findings’ robustness.
The Paradox of Sticky Health Beliefs
Having seen Trump’s pivot was associated with an increase in Republicans’ reported facemask use, I now turn to whether health beliefs provide a credible mechanism to explain the observed behavioral change. Thus, I ran the original specification but used belief in masks’ efficacy as the outcome. Overall, I find no evidence that Trump’s pivot changed individual views about masks’ efficacy (see Table 4 and Figure 7).
Static Results for Belief in Facemask Efficacy Stratified by Partisanship
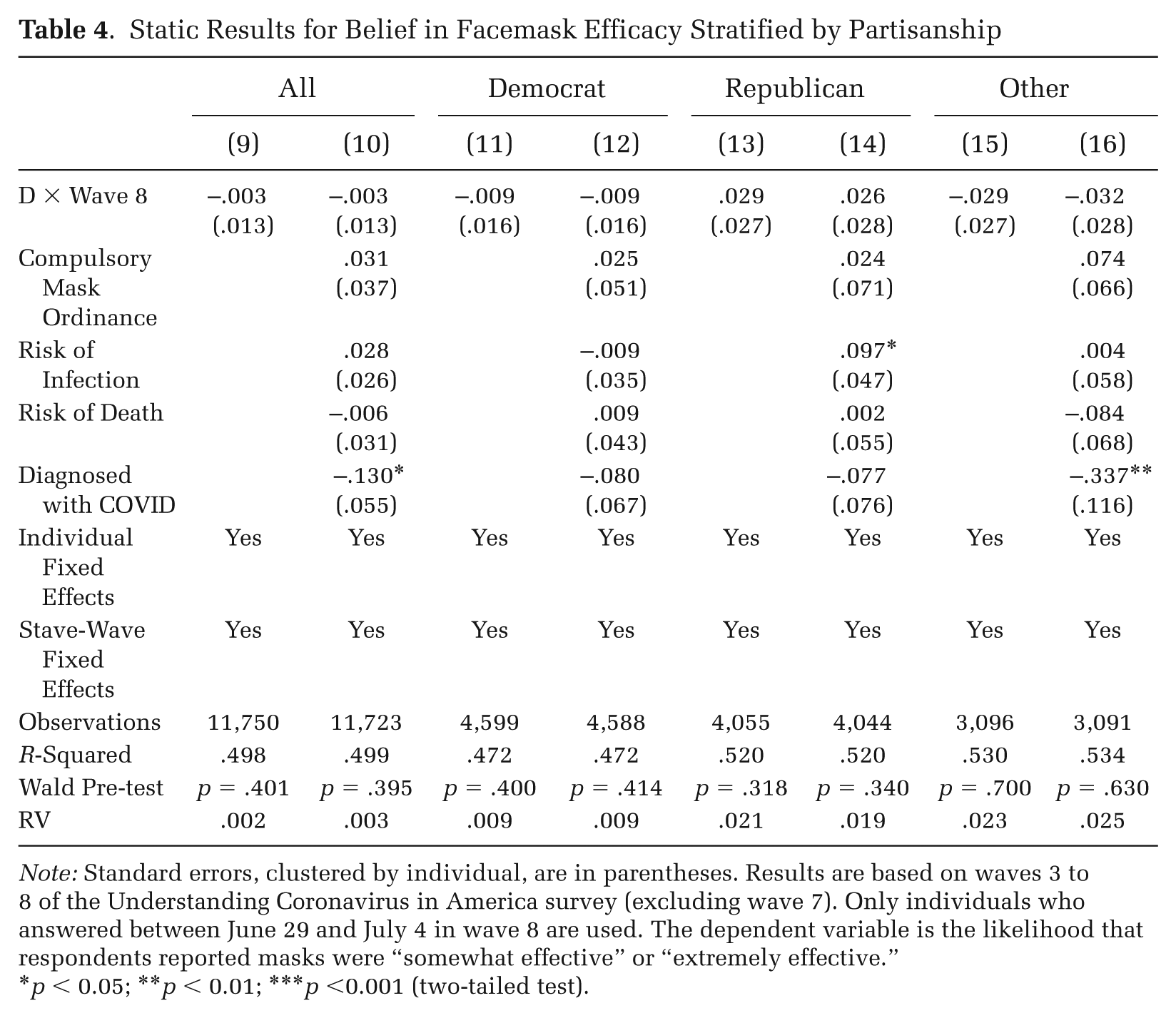
Note: Standard errors, clustered by individual, are in parentheses. Results are based on waves 3 to 8 of the Understanding Coronavirus in America survey (excluding wave 7). Only individuals who answered between June 29 and July 4 in wave 8 are used. The dependent variable is the likelihood that respondents reported masks were “somewhat effective” or “extremely effective.”
p < 0.05; **p < 0.01; ***p <0.001 (two-tailed test).
Dynamic Results for Facemask Efficacy, Stratified by Partisanship and Moderation Analysis
To confirm these null results, I conducted a number of tests. First, to check this result is not the product of an excessively tight bandwidth, I reran results at different selections. At no bandwidth selection do I find significant results for Trump’s pivot (see Tables 1C to 4C in the online supplement).
Second, I reapplied alternative approaches that were previously attempted: removing individual and state-wave fixed effects (Table 5C), trajectory balancing (Table 6C), and using the full set of waves (Table 7C). None of these procedures change the previously found null results.
Third, I estimated results with the dependent variable coded differently. For example, only coding “extremely effective” as 1 and all other responses as 0, or treating the health belief item as a continuous scale from 0 to 4, with 0 being “extremely ineffective” and 4 being “extremely effective.” Again, no effect on beliefs can be identified (see Table 8C in the online supplement).
Fourth, to ensure this null effect is not the consequence of a backlash (i.e., of some Republicans’ decreasing belief in masks’ efficacy), I reexamined results for the dynamic specification stratifying individuals by whether they thought facemasks were effective in wave 6. I find no sign of such a reversal in Republicans’ views on masks (see Figure 1C in the online supplement).
Overall, these findings suggest belief in masks’ efficacy was less responsive than behaviors. Counter to theoretical expectations, health beliefs, or at least belief in masks’ efficacy, appear an unlikely pathway by which Trump fostered masks’ uptake.
Question Wording
Although these estimates seemingly demonstrate that Trump’s pivot did not persuade Republicans of the efficacy of facemasks, that does not rule out the possibility that his intervention might have affected other views about masks. Perhaps had the question been worded in terms more amenable to Republicans, the results too would have been different.
In response to this concern, the online supplement presents evidence from a broader battery of questions on masks introduced in wave 8. Respondents were asked, “We would like to learn your general opinion about wearing a mask or face covering. Do you agree or disagree with each of the following statements?” Individuals were presented with 12 statements, in a random order, covering a wide array of potential views. Some statements were explicitly political, for example, “We live in a free country and no one can force me to wear a mask.” Some statements were more interpersonal: “Others may feel threatened if I cover my face.” For a full list of statements, see Table 9C in the online supplement. For each item, responses are coded 1 if participants answered “agree” or “strongly agree” and 0 otherwise.
Using only wave 8, I ran LPMs for each item, using the same set of controls and state fixed effects (to remain as close as possible to the main specification), with a simple pre-post design. Among Republicans, I find no evidence of a significant change on any item, suggesting the null results are not simply an artifact of question wording (see Tables 10C to 13C in the online supplement).
Alternative Narratives for Health Beliefs
Given these null results, it is reasonable to ask if beliefs might have played a different role. At least two alternative narratives could be proposed. First, Trump’s pivot, although not persuading Republicans of masks’ efficacy, might have given permission to those already convinced they worked to use one. Second, the effect of Trump’s intervention may have differed as a product of the strength of individuals’ convictions about masks, that is, Republicans who were uncertain or held moderate views about masks’ efficacy may have been more swayed, in terms of subsequent behaviors, than those fully convinced of their position.
To examine the plausibility of these alternative explanations, I re-estimated the original specification with facemask use as the dependent variable, comparing results for Republicans stratified by their self-reported belief in masks’ efficacy to protect against COVID-19 in wave 6 (see graphical results in the bottom-right of Figure 7 and numerical results in Table 14C in the online supplement). Although the smaller sample makes effects generally insignificant, it is clear that results do not vary substantially, with the exception of the small group of Republicans who answered “uncertain” in wave 6 (N = 33), for whom Trump’s pivot seems to have been less effective. Although these results are inconclusive, overall these findings do not suggest any clear moderating role for preexisting beliefs. Instead, these results demonstrate small but positive effects for respondents who were previously supportive or previously skeptical of masks’ efficacy.
As a theoretically relevant extension, I repeat the above approach in the online supplement using the original binary variable for belief in facemask efficacy as the outcome. Again, no discernable pattern can be detected (see Table 15C in the online supplement), further supporting the notion that outcomes did not significantly vary as a function of previous beliefs.
The Moderating Effects of Crisis
Finally, I consider whether the effect of Trump’s pivot was moderated by local epidemiological conditions, specifically the extent of the early-summer 2020 spike in COVID-19 cases. To that end, I estimated a three-way interaction, using the summer shock variable to gauge how much more or less effective Trump’s position reversal was as a function of rising cases during June 2020 at the state level (for results at alternative bandwidths, see Table 5 and Tables 1D to 4D in the online supplement). Figure 8 displays these results.
Three-Way Interaction Results for Wearing a Facemask
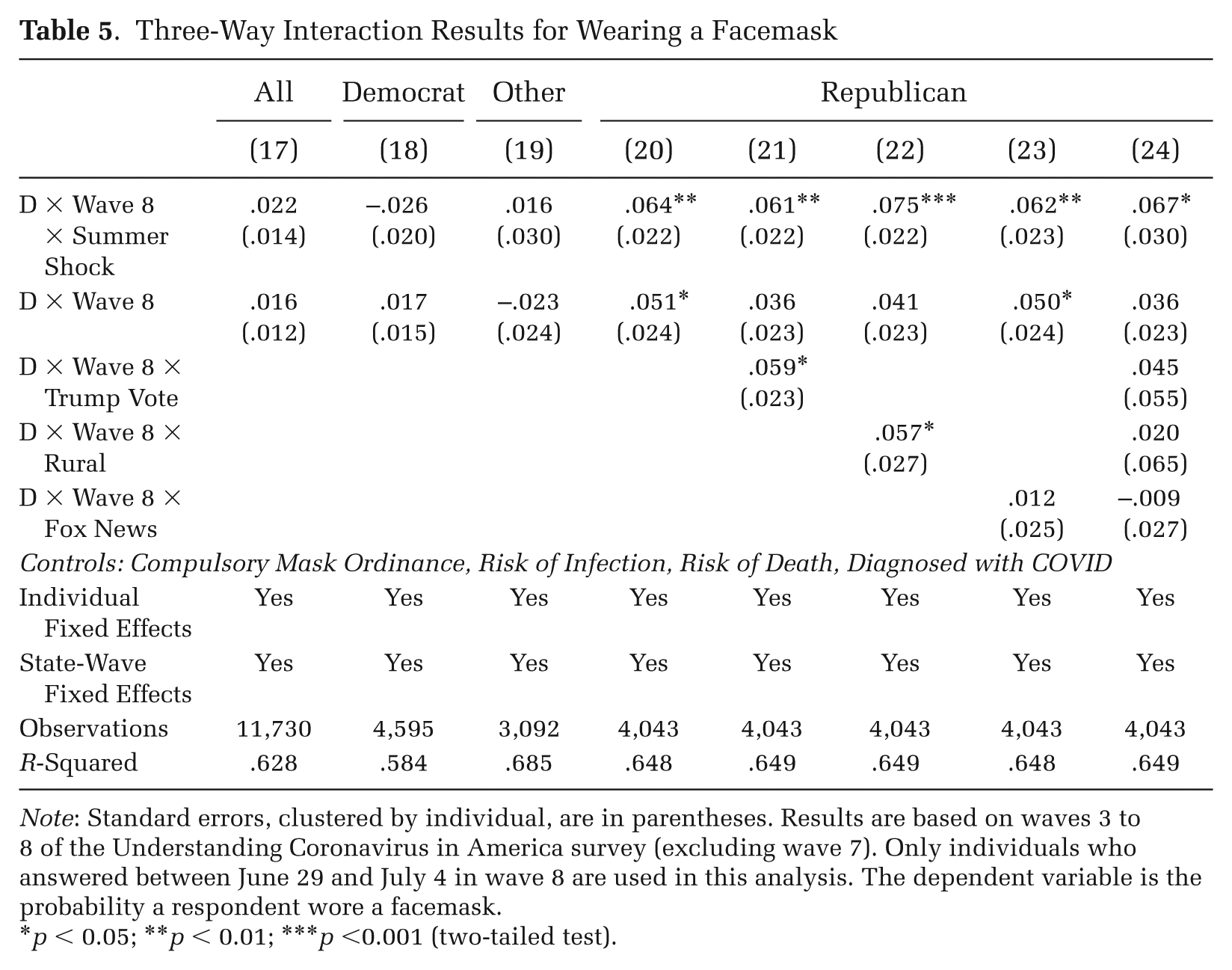
Note: Standard errors, clustered by individual, are in parentheses. Results are based on waves 3 to 8 of the Understanding Coronavirus in America survey (excluding wave 7). Only individuals who answered between June 29 and July 4 in wave 8 are used in this analysis. The dependent variable is the probability a respondent wore a facemask.
p < 0.05; **p < 0.01; ***p <0.001 (two-tailed test).
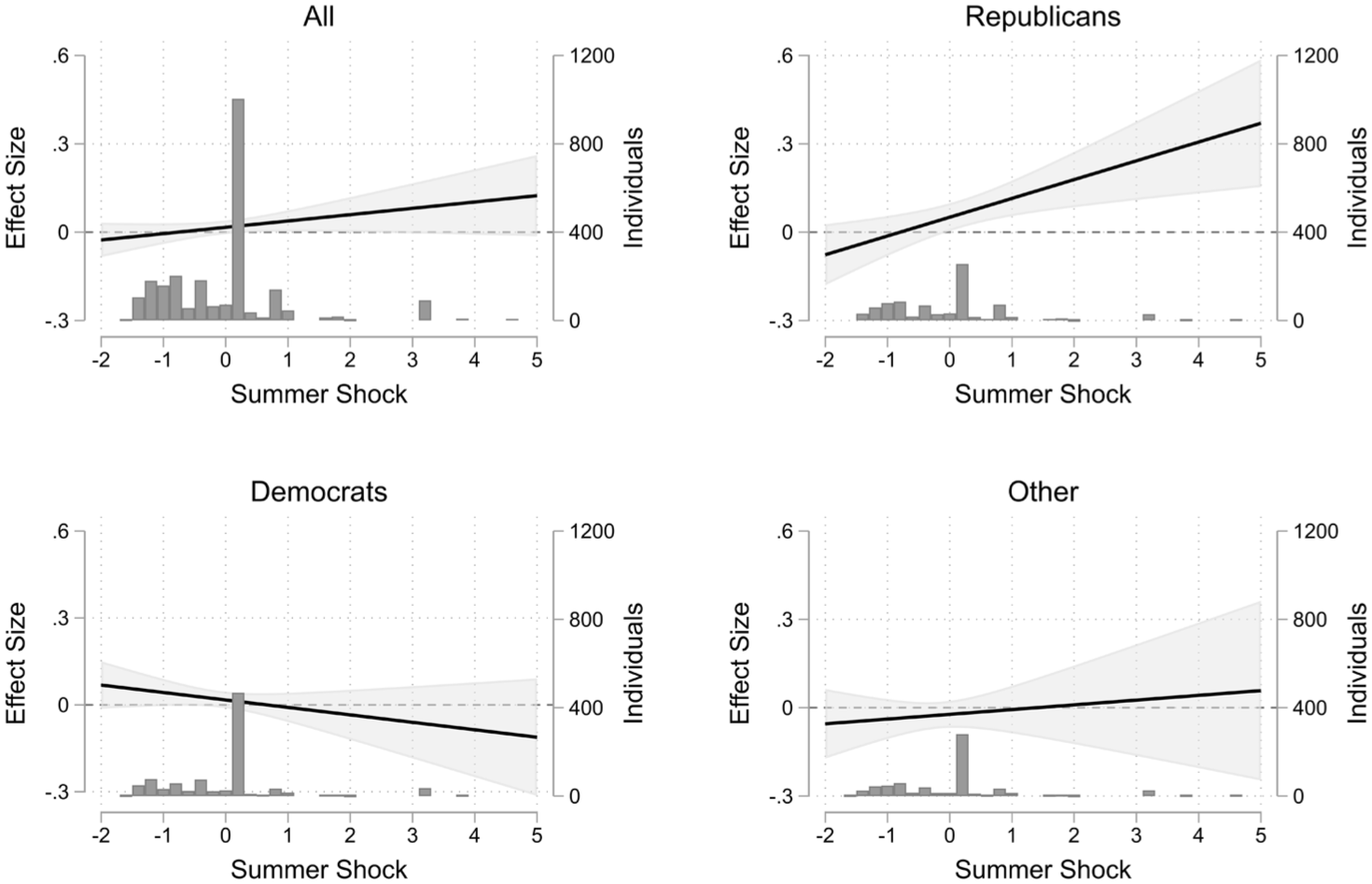
The Moderating Role of Local Epidemiological Conditions
When the summer shock variable is equal to 0 (at the average), we see a 0.05 increase in the probability of wearing a facemask among Republicans associated with Trump’s pivot. Then, for every one-standard-deviation increase of the summer shock variable in a respondent’s state of residence, Trump’s intervention had approximately 0.06 more of an effect among Republicans. For example, these estimates imply that in states where the summer shock variable was one-standard-deviation above the mean, Trump’s pivot led to a 0.11 increase in Republicans’ probability of wearing a facemask (for marginal effects at different values, see Table 5D in the online supplement). This result provides strong initial evidence that Trump’s pivot was substantially more effective in places where there had just been a sharp spike in case numbers.
Potential Confounders
Looking back at state-level variation in rising COVID cases during June 2020 (Figure 4), it seems obvious that states experiencing the most significant rise in cases were more conservative and arguably more rural. To check these results are truly due to the rise in new cases—and not some other confounder varying at the state level—I used additional interactions for the proportion of individuals who voted for Donald Trump in 2016, the proportion of individuals living in rural areas in 2020, and the June 2020 Google Trends Interest Scores for Fox News. None of these checks produce significantly different results.
To ensure this geographic heterogeneity is robust to controlling for more individual-level features, the online supplement shows the specification run using additional interactions for race (being white non-Hispanic versus other groups), gender, having a college degree, self-reported ideology from the 2019 End of Year Survey (on a scale between 0 and 8, where 0 is “extremely liberal” and 8 is “extremely conservative”), and trust in Fox News asked in wave 1 of UCA (on a scale between 0 and 3, where 0 is “do not trust at all” and 3 is “trust completely”). None of these checks change the final results (see Tables 6D to 9D in the online supplement).
Level of Analysis
The subject of individual characteristics raises another important point: at what level should this variation, emerging from epidemiological conditions, be modeled? The main analytic strategy treats rising cases as an ecological factor, applying to everyone in a state regardless of personal exposure. The wisdom of that choice depends on theoretical questions around how individuals interact with crisis. If crisis is experienced predominantly through direct personal channels, that is, getting COVID oneself or knowing someone with COVID, then the current approach might be missing out on substantial variation at the individual-level. If, however, crisis is constructed more collectively (e.g., via media reporting), then it may indeed be local (not personal) conditions that best capture heterogeneity.
To explore this issue empirically, Table 10D in the online supplement presents results with additional interactions for self-reported COVID diagnosis, knowing someone infected with COVID, knowing someone hospitalized for COVID, and knowing someone deceased from COVID. These additional interactions do not substantially alter the summer shock variable’s moderating effects. But they do reveal something unexpected: Republicans who report being diagnosed with COVID are more reactive to Trump’s pivot, but those who report knowing others with varying degrees of exposure are less reactive. Different versions of personal COVID exposure are not my focus here. But these results suggest personal and ecological exposure might function differently depending on the form they take. Consequently, these findings point toward this article’s state-level analysis capturing something distinct from individual-level experiences’ aggregation, which may itself merit further exploration in future work.
Common Support
Beyond concerns about confounders and level of analysis, there may also be cause to believe this three-way interaction is biased by a lack of common support (Hainmueller, Mummolo, and Xu 2019), that is, gaps in the moderator’s value leading to spurious interpolation. In general, the summer shock variable evolves smoothly across states, but there are outlier states with much higher values—notably Florida, Idaho, and Montana (see Figure 4). To ensure the findings are not simply a product of these outliers, I reran the results excluding these three states. These states’ exclusion does not produce substantively different findings (see Table 11D in the online supplement).
Similarly, the three-way interaction’s linear form implies marginal effects are uniform across the distribution. However, conceptually it makes more sense to think that although large increases in case numbers strengthen the pivot’s effect, decreases are unlikely to have an equivalently negative effect. To study this potential asymmetry, I estimated an alternative specification: I compared reactions in the top and bottom tercile of the summer shock variable to those of the middle tercile (see Table 12D in the online supplement). Although numerically the bottom tercile appears to react less positively than the middle tercile—supporting the idea of monotonicity—this difference is not significant. For the top tercile, we do see a large and significant difference in the effect—around 0.15 higher than the middle tercile. These results are robust to excluding the outlier states. Overall, these findings confirm a basic theoretical intuition that deteriorating, rather than improving, conditions exert a more powerful moderating effect.
These findings robustly suggest Trump’s power to change his followers’ behaviors lay, at least partially, in his decision to act at a moment of renewed crisis and was especially effective in parts of the country most affected by the sudden spike in cases during summer 2020. Such a finding is consistent with a view that crisis conditions amplify the potency of leaders’ speech, enabling them to shift behaviors in ways usually not possible.
Discussion
Across Western societies, the fields of health, science, and politics are becoming increasingly intertwined as polarization seeps into individuals’ everyday choices (Gauchat 2012; Lynch 2023), a process only accelerated by the pandemic. In that context, I sought to use Trump’s unexpected pivot on facemasks to understand if a position reversal by a populist leader can lift compliance with important protective behaviors among followers.
This article confirms several empirical findings from extant literature on political communication during the pandemic. Following Trump’s pivot, Republicans were significantly more likely to wear facemasks. Among Democrats, there was no effect. These results reaffirm previous work showing how partisanship moderates the effect of leaders’ cues (Cherry et al. 2021; Pink et al. 2021), contributing to a literature arguing that political speech fed into differentiated uptake of new health behaviors’ adoption along party lines.
However, this article also challenges received wisdom, especially from public health scholarship. Trump’s pivot did not—either among co or opposition partisans—significantly affect individuals’ belief in masks’ efficacy as a protective measure against COVID-19, suggesting he did not change behaviors through rational persuasion. Neither does it seem Trump merely gave permission to those already convinced of facemasks’ efficacy. My analysis (see Figure 7) indicates Trump’s pivot had no more of an effect for individuals already convinced of masks’ efficacy than for those skeptical of their use. Of course, these results should not be taken as a general refutation of the health belief model (Jones et al. 2014; Kasl and Cobb 1966) or other rationally grounded models of behavioral change. But this finding should be read as an indication that some powerful cognitive mechanism operates separately from beliefs.
This article provides clues pointing toward plausible candidates for this alternative mechanism. Consistent with much qualitative work and predictions from AIT (Lasco and Curato 2019; Marcus et al. 2000; Swidler 1986)—but also, importantly, contrasting with SJT’s expectations—I find Republicans living in states worse hit by the early-summer 2020 rise in COVID cases were more affected by Trump’s intervention in terms of mask use. This suggests Trump’s capacity to shape behaviors lay not so much in persuading followers, but in capitalizing on a moment of crisis when individuals were more attentive to such cues, even if they were not rationally convinced.
But any definitive answer as to how Trump apparently bypassed beliefs remains opaque. This article is not the first to uncover such a puzzle (Centola et al. 2005; Kim et al. 2024; Kim and Zuckerman Sivan 2017), and previous work has tried to describe this pathway as emotion (MacKuen et al. 2010), pluralistic ignorance (Sargent and Newman 2021), or even an evolutionary drive to mimicry, often called the culture-gene (Henrich and Muthukrishna 2021).
That this behavioral change was seemingly carried into the long-term—an especially surprising result given that, outside of facemasks, Trump continued to downplay COVID’s seriousness—suggests this shift in practices was, at least after the event, accompanied by some effortful cognitive transformation. My intuition here is that mask use was sustained by sophisticated reasoning reconciling medical skepticism with behavioral compliance, similar to what qualitative medical sociologists have observed (Reich 2020; Tavory and Swidler 2009; Urena 2022). That is, individuals might be negotiating strong personal distrust of public health authorities with powerful support for Trump, resulting in complex ex-post explanations for behaviors better captured in interviews. However, it is also plausible that what changed were perceptions of social norms (Horne and Mollborn 2020)—that is, how respondents imagine others perceive certain behaviors—which this article lacks clear evidence to adjudicate on.
Theoretical concerns apart, there are also empirical limits to this work. First, declarative data may bias results, especially if participants engaged in expressive responding (Schaffner and Luks 2018), that is, misreporting to show allegiance to a political camp. That beliefs and behaviors did not move similarly suggests something beyond expressive responding must have taken place. But setting that aside, this article’s broader position is that such risks are worth taking. Ecological approaches, with more objective behavioral measures, have to make strong cognitive assumptions (Bisbee and Lee 2022; Dickson and Hobolt 2025). This article complements that previous work, supporting many of its conclusions on the interplay between speech and context, but refining the theoretical narrative around what drove partisan gaps in behaviors.
Second, this article’s focus on a single leader and a single behavior restricts external validity. Trump is a president particular in both his personal and situational characteristics: a white man immersed in a peculiar U.S. media landscape. Equally, masks were a novel object, uncomfortable, and more public than other health recommendations. Other actors (Ash et al. 2024), parts of the world (Ajzenman et al. 2023), and behaviors (Petherick et al. 2021) may have functioned differently. Accordingly, this work should be seen as existing in a scholarly tradition focused on consequential black swans (Popper 1959), emphasizing cases able to broaden what is considered theoretically possible and closer epistemologically to positivist qualitative approaches than much quantitative work seeking highly generalizable findings (Findley, Kikuta, and Denly 2021; Seawright 2016).
Third, there may be unidentified sources of heterogeneity in the effect. Although this article illuminates certain sources of variation well, particularly from epidemiological conditions, there are no doubt other ways the effect could have been moderated. There may well be variation among Republicans based on loyalty to Trump. Even more powerfully, it is possible to imagine the pivot might have had more effect among individuals inculcated in dense Trump-supporting networks. Such latent characteristics are hard to operationalize, even with individual-level data. But, given the consequential nature of this president, it is something survey methodologists could consider developing going forward.
Beyond empirical limitations, a larger issue is at play: can these results be considered causal? Inevitably, scholars will draw the line of causality differently (Imbens 2024; Schwartz and Prins 2025). But for this article, the salient concern would seem to be whether these results could have emerged in the absence of Trump’s pivot. If Trump had access to some signal telling him Republicans were about to change behaviors, it is possible these results are victim to misidentification. Indeed, Trump’s capacity to empathize with supporters should not be dismissed, and I encourage investigation into his motives. However, given Republicans’ use of facemasks was, if anything, declining prior to his pivot (see Figure 3)—alongside the study’s tight window of analysis, meaning Trump would have needed to have timed his reaction very precisely—this appears improbable. Therefore, while acknowledging the legitimacy of endogeneity concerns, it nonetheless seems reasonable to conclude that this behavioral shift would have been unlikely to occur without Trump’s pivot.
Despite shortcomings, this work highlights an important moment of behavioral change in the pandemic’s history. Although small in absolute terms—with perhaps only 5 percent of Republicans shifting practices—this effect is substantial relative to the partisan divide in mask use, equivalent to closing about 40 percent of the Republican–Democratic gap. More importantly, for a theory of the leader-follower relationship, this article challenges dominant narratives in public health scholarship about beliefs’ centrality in changing behaviors, pointing not only toward broader explanations found in both sociological and cognitive science literature, but also to such unconventional communication styles’ potential value.
Rather than persuading through reason, it was by leaning into the crisis-driven, performative style of populist leaders (i.e., comparing himself to a cowboy in a facemask when the United States was experiencing a surge in COVID cases) that Trump fostered a change in Republicans’ behaviors. It is impossible to disentangle all the different elements of this one interview, but there is perhaps a crucial lesson here that goes beyond the pandemic. If public health messaging’s aim is to shift behaviors among individuals most skeptical of institutional guidance, it may be important not only to recruit populist politicians to the cause, but also to understand why their performative style works better for difficult-to-reach populations. Issues of rhetoric are beyond this article’s scope, but these findings should encourage further research in that direction.
Supplemental Material
sj-pdf-1-asr-10.1177_00031224251415372 – Supplemental material for When Political Pivots Shift Behaviors but Not Beliefs: Evidence from Trump’s Position Reversal over Facemasks during the COVID-19 Crisis
Supplemental material, sj-pdf-1-asr-10.1177_00031224251415372 for When Political Pivots Shift Behaviors but Not Beliefs: Evidence from Trump’s Position Reversal over Facemasks during the COVID-19 Crisis by Bartholomew A. Konechni in American Sociological Review
Footnotes
Acknowledgements
I am indebted to participants of the CRIS Scientific Seminar at Sciences Po Paris and the session on the Development of Health Policy and its Multifaceted Impacts on People and Political Structures at ASA’s annual conference for their substantial contributions to this manuscript. I would also like to recognize the highly constructive role of the anonymous reviewers who did their upmost to make this the most robust article it could be.
Funding
This research was funded by a public grant overseen by the French National Research Agency as part of the Investissements d’Avenir program LIEPP (ANR-11-LABX-0091, ANR-11-IDEX-0005-02) and the Université de Paris IdEx (ANR-18-IDEX-0001).
Data Note
The analysis conducted in this article relies on the following data sources. For the Understanding Coronavirus in America Study, the data underlying this article cannot be shared publicly due to privacy concerns. However, the data can be accessed upon request by making an application at the following link: https://uasdata.usc.edu/index.php. For the Oxford COVID-19 Government Response Tracker, the data underlying this article are available in GitHub, at https://github.com/OxCGRT/covid-policy-dataset. For the CDC’s Weekly United States COVID-19 Cases and Deaths by State, the underlying data can be accessed at https://data.cdc.gov/Case-Surveillance/Weekly-United-States-COVID-19-Cases-and-Deaths-by-/pwn4-m3yp/about_data. Data on state-level support for Trump at the 2016 presidential election can be obtained from the MIT Election Lab at https://electionlab.mit.edu/data. Data on Google Trends Interest Scores can be obtained at https://trends.google.com/trends/. Data on the proportion of individuals in each state living in rural areas are from the U.S. Census at https://data.census.gov/. All code to reproduce results and non-sensitive data can be found at ![]() .
.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.