
Abstract
In the governance of poverty and marginality, a complex array of frontline workers manages social suffering. Enabled and constrained by vertical and horizontal relations of production, these workers frequently redistribute work across organizational boundaries. Recent scholarship often reduces such redistribution to a single dynamic: “burden shuffling.” This study extends and complicates that framework. Drawing on three case studies—ambulance crews, mandated reporters of child maltreatment, and physicians treating chronic pain—we theorize how frontline workers’ practical and moral judgments structure the form and justification of redistribution. Variation in the extent to which workers feel equipped and see tasks as worthwhile produces three distinct tactics: burden shuffling (when ill-equipped workers offload tasks they do not consider worthwhile), aspirational referrals (when ill-equipped workers seek better-equipped actors for tasks they view as worthwhile), and abandonment (when well-equipped workers disengage from tasks they deem unworthy and leave them to others). By disaggregating redistribution and tracing its relational conditions, this article shows how governance is enacted—and deferred—on the frontlines, and we offer a framework for understanding how workers navigate fragmentation and uneven responsibility in contemporary labor.
Keywords
Introduction
Contemporary work is characterized by segmentation, differentiation, and fragmentation (Braverman 1974; Durkheim [1893] 1984; Kalleberg 2011; Weil 2014). This is evident, among other places, in the governance of poverty and marginality, where a complex array of frontline workers have been tasked with responding to social suffering: teachers (Maynard-Moody and Musheno [2003] 2022), physicians (Sufrin 2017), police (Stuart 2016), welfare workers (Seim 2026; Watkins-Hayes 2009), probation officers (Phelps and Ruhland 2022), building inspectors (Bartram 2022), needle exchange workers (DiMario 2022), and more. These workers do not operate within a coherent regime designed to regulate suffering. In a neoliberal era marked by high levels of marketization and managerialism on the one hand, and state devolution and delegation on the other, they are embedded in a fragmented and contradictory set of organizations (Halushka 2023; Paik 2021; Sered and Norton-Hawk 2014). This produces a complex, and sometimes irrational, division of governance labor (Barnard 2023; Comfort et al. 2015; DiMario 2022; Gong 2024).
Given such fragmentation, much scholarship on relations between workers across organizations has focused on frontline workers managing social marginality and suffering. A key insight from this research is that suffering populations and the tasks and cases associated with them are perpetually redistributed across institutions and organizations (Lara-Millán 2021; Sirois 2023), often through a process of “burden shuffling” (Brooks 2025; Herring 2019; Martino, Dej, and Sanders 2026; Seim 2020). Vertical pressures from above, including budget and policy constraints, limit workers’ capacity. And vertical pressures from below, such as clients whose needs fit poorly with workers’ skills, tools, resources, and sense of vocation, limit opportunities for meaningful labor. Workers respond by transferring clients, responsibilities, and risks horizontally—making these cases someone else’s problem in another department, site, or institution.
Yet, burden shuffling is but one approach to redistribution. How do other work conditions shape the tactics workers use? This article theorizes the significance of workers’ equippedness and their subjective sense of worthwhile labor to show how variation across these features produces different forms of redistribution. These dimensions are analytically distinct. Workers are equipped based on their technical and organizational capacity—their ability to perform certain tasks. Labor is worthwhile based on workers’ moral evaluations of whether a task merits attention.
We analyze three case studies with different combinations of these features: a study of ambulance crews responding to 911 calls, a study of frontline workers mandated to report suspected child maltreatment, and a study of physicians working with pain patients. We affirm that burden shuffling is a common response when ill-equipped workers face client problems they consider unworthy of attention—the condition most prominent in prior literature. The ambulance case best illustrates this. However, there are also instances in which ill-equipped workers confront client problems they consider worthy of intervention. Such conditions motivate “aspirational referrals,” in which workers justify their redistribution to other, purportedly better-equipped workers by emphasizing benefits for the client. The mandated reporter case best illustrates this. Finally, there are cases in which better-equipped workers encounter tasks they see as generally not worthwhile. This can result in redistribution through “abandonment,” especially when workers can reject clients with minimal legal risk to themselves. The case of physicians working with pain patients best illustrates this.
Taken together, our multi-case analysis identifies important variations in the opportunities and interests of frontline workers that shape how clients are sorted across organizations. The redistribution of suffering populations is not uniform but emerges from the particular material and moral conditions of frontline workers. Our analysis speaks to enduring questions in the study of frontline governance specifically and work more generally, with implications for scholarship on boundary-spanning work (Aldrich and Herker 1977), the moral and affective organization of labor (Hodson 2001), and the restructuring of organizational responsibility under increasingly fragmented systems of work (Weil 2014).
Frontline Governance of Suffering and Marginality
Today, the governance of suffering populations is disaggregated across a complex network of organizations, a process intensified by neoliberal reforms that promote devolution, delegation, and discontinuity. Public agencies, nonprofit organizations, and contracted firms collectively implement social policy (Marwell 2004; Marwell and Morrissey 2020), mirroring fragmentation in the private sector through subcontracting, franchising, and outsourcing (Weil 2014). Government—understood as a specific set of state agencies and public employees—has given way to governance, a process of managing populations across public and private entities that blurs the distinction between state and civil society (Rhodes 1996). This fragmentation, in tandem with conditions of austerity, has dispersed responsibility for managing suffering across organizational boundaries (Barnard 2023; Lara-Millán 2021).
Vertical Relations of Frontline Governance
In this context, it is frontline workers across governmental and nongovernmental organizations who directly confront the task of handling suffering populations. Although these workers may not exclusively serve marginalized groups, they collectively bear the weight of responding to social suffering. In his influential book Street-Level Bureaucracy, Michael Lipsky ([1980] 2010) argues that public policy is made most immediately and practically by “street-level bureaucrats,” such as welfare workers, teachers, and police officers, who directly interface with clients. These frontline workers implement, or “materialize,” policy by exercising substantial discretion while distributing public resources, services, and sanctions (Dubois 2012; Lipsky [1980] 2010; Maynard-Moody and Musheno [2003] 2022; Zacka 2017).
A long literature advanced by Lipsky and other scholars of street-level bureaucracy theorizes how frontline workers make decisions. This work highlights the vertical relations between workers and those situated above and below them that shape policy implementation work (Chiarello 2015; DiMario 2022; Hupe and Buffat 2014; Maynard-Moody and Musheno [2003] 2022; Maynard-Moody and Portillo 2010; Seim 2020). Street-level bureaucrats experience pressures from below—from the subjects they are tasked with aiding, punishing, and so on—in the form of clients’ needs, claims, and acts of resistance. These same workers also face pressures from those attempting to control and coordinate their labor from above, including via law and organizational policy, as well as managerial efforts to increase efficiency and effectiveness. In fact, these vertical pressures can constrain frontline discretion so severely that many employees—most notably contemporary welfare workers—become “proletarianized public servants” more so than “street-level bureaucrats” (Seim 2026). Yet verticality is only one dimension of frontline governance. Horizontality matters too.
Horizontal Relations of Frontline Governance
Horizontal relations between institutions, sometimes across the boundaries of distinct fields of governance, are central to contemporary work. Yet historically, scholarship on frontline governance workers has often assumed but rarely examined these relations. The allocation of tasks or people to organizations is not fixed; rather, organizational boundaries are dynamic and negotiated. In the street-level bureaucracy context, Hupe and Hill (2007) note that Lipsky’s ([1980] 2010) classic model details several different occupations in a complex division of labor, but it does not explain the relations between them, despite the organizational fragmentation that suffering populations in the contemporary United States confront. Given the United States’ frayed social safety net, people often fail to get the help they need as they are continually bounced around across organizations. Individuals find themselves sent on a “runaround” (Halushka 2023), traversing an “institutional circuit” (Sered and Norton-Hawk 2014), navigating “multi-institutional mazes” (Paik 2021), and confronting inter-organizational “irrationality” (Comfort et al. 2015). Such complexity and fragmentation characterize bureaucratic work environments more broadly, including in the private sector (Hodson et al. 2013).
This neglect of horizontality has changed in recent years, with sociologists studying frontline workers in different sectors and tracing how they produce the circuitous “runaround” through their inter-institutional relations with one another (Chiarello 2024; DiMario 2022; Herring 2019; Lara-Millán 2021; Seim 2020; Sirois 2023; Stitt 2025; Stuart 2016). While documenting important commonalities across workers such as teachers, cops, doctors, judges, welfare caseworkers, and so on, scholars have increasingly attended to the horizontal relations between these workers—including their sharing of subjects, discourses, tools, technologies, and more, as well as their conflicts with one another over the division of tasks, jurisdictional boundaries, and case classifications. As this research shows, we often cannot understand the behavior of focal workers without understanding their interactions with adjacent horizontal actors. These horizontal relations are fundamental to frontline governance work.
Redistributing the Suffering
Combined, the vertical and horizontal relations of frontline work help explain why suffering populations are sent on runarounds and other similar trajectories. Specifically, workers often redistribute people. Perhaps no text makes this clearer than Lara-Millán’s Redistributing the Poor: Jails, Hospitals, and the Crisis of Law and Fiscal Austerity (2021). This historically-embedded ethnography argues that the poor have been sorted, or “redistributed,” across the penal and medical states by frontline nurses and jailers. These workers are embedded in vertical relations both below them (with patients and people who are incarcerated) and above them (with administrators). The administrators in Lara-Millán’s (2021:164) analysis confront a contradictory mixture of legal demands and austerity that drives horizontal exchanges of clientele in an effort to realize organizational efficiency and “disappear suffering.”
In a manner generally synonymous with redistribution, scholars have theorized how frontline workers under similar vertical pressures seek to “burden shuffle” (Brooks 2025; Herring 2019; Martino et al. 2026; Seim 2020) and “offload” (Sirois 2023) their subjects onto workers at other organizations. Workers confront protocols and managers from above that limit their capacity for intervention, while simultaneously confronting clientele with problems mismatched with their skills, tools, jurisdictions, and overall sense of vocation (Abbott 1988; Seim 2020). Sandwiched in an untenable position, workers construct cases in ways that permit them to move unwanted or risky tasks onto peers in adjacent organizations (Sirois 2023), “largely out of interests of convenience and a general effort to disclaim liability” (Seim 2020:464). Thus, research to date generally portrays frontline workers passing clients and cases off to other workers in other organizations in an effort to offload or shuffle burdensome work.
Beyond a Uniform Model of Redistribution
Prior scholarship underscores redistribution as a key practice of frontline workers in complex fields of governance. This work draws on cases that workers feel ill-equipped to tackle and that they interpret as undeserving of their attention. As such, these studies have conceptualized redistribution as workers passing burdensome tasks off to those in other organizations. However, these conditions are not universal. In other contexts, frontline workers may feel more equipped to handle the task at hand, or they may see the task as more worthy of attention. That is, frontline work has material and moral components that vary in ways that may shape redistribution.
Specifically, subjects’ needs or claims can indeed be a poor fit for workers’ resources and skills, such that the task at hand is misaligned with what frontline workers can offer. But frontline workers may not always see their tools as inadequate. Presumably, there are opportunities for educators to educate, for police officers to make arrests, and for healthcare workers to provide healthcare. Likewise, frontline workers do not necessarily always dismiss the importance of addressing subjects’ needs. The extent to which cases are deemed “bullshit” (Seim 2020; see also Karunakaran 2024) or “crocks” (Becker 1993) may vary. Even in seemingly hyper-rational bureaucracies, moral evaluations are embedded in work (Dubois 2012; Hodson 2001; Maynard-Moody and Musheno [2003] 2022; Seim 2020; Zacka 2017) in ways that may be unrelated to the tools workers have at their disposal. Frontline workers may venerate the importance of some tasks even if they feel poorly equipped to address them.
Given that workers operate in the context of different constraints and opportunities, might they use other tactics—beyond shuffling problems along—to shift subjects across institutional spaces? We examined this possibility by comparatively analyzing three cases that vary along key dimensions. Workers in these cases pursued multiple forms of redistribution, with the tactic used depending on the interplay between workers’ equippedness to perform certain tasks and the extent to which they perceived the tasks as worthwhile. Our analysis illuminates how frontline workers strategically call upon—or decline to call upon—their horizontally-adjacent counterparts, with implications for subjects’ experiences on the runaround (Halushka 2023).
Cases and Methods
Ambulance Crews in a Fragmented Emergency System
Our analysis draws on three distinct case studies. First, we draw on an ethnographic study of ambulance labor. Mixing “participant observation” (i.e., ride-alongs) and “observant participation” (i.e., novice ambulance work) fieldwork across a 21-month period, Seim encountered 566 ambulance cases and shadowed or worked with 48 paramedics, 19 emergency medical technicians (EMTs), and 8 paramedic supervisors. This research was conducted in 2015 and 2016 in an unnamed California county where 911 ambulance operations are contracted to a for-profit firm. Seim took detailed fieldnotes of every shift he shadowed and worked, first by jotting notes in the field and then by elaborating them into detailed narratives.
This was a theory-driven study examining the ambulance labor process that involved, among other things, a focus on the social relations of paramedical production. For the purposes of this article, we analyze the horizontal relations between ambulance crews and the other street-level bureaucrats who tend to share their clientele, namely nurses, firefighters, and cops.
Mandated Reporters in a Fragmented Family Services System
Second, we draw on an interview study of Child Protective Services (CPS) reporting. Many frontline workers are legally mandated to report suspected child maltreatment (abuse and neglect) to CPS, the state agency tasked with investigating such reports. Statutes defining child maltreatment are often vague and subjective, such that frontline professionals have substantial discretion when deciding how to respond to situations that could be labeled (or not) as child maltreatment.
In 2018 and 2019, Fong conducted individual interviews with 38 “mandated reporter” professionals in two regions of Connecticut (New Haven and the northeastern region of the state), including people working in education, healthcare, mental health services, law enforcement, and social services. This interview study was part of a larger study of CPS investigations, so most of these professionals were recruited because they had filed a recent report to CPS that was part of the larger study. Other participants were identified via the researcher contacting local organizations that employed mandated reporters. Interviews lasted approximately 45 minutes and were conducted in person, typically at the interviewee’s workplace. The interview protocol focused primarily on the horizontal relationship between interviewees and CPS, with questions eliciting interviewees’ perceptions of, expectations for, and experiences with their most recent CPS report. For this analysis, Fong reviewed interview transcripts closely to identify and code for themes related to mandated reporters’ decision-making around referring families to CPS and their understandings of the CPS workers to whom they were referring.
Physicians in a Fragmented Healthcare System
Third, we draw on an interview study of physicians who make decisions about opioid provision in the context of an escalating overdose crisis. For the larger study, conducted from 2009 to 2019, Chiarello interviewed three types of physicians: doctors working in general practice, pain management, and emergency medicine in four states (California, Florida, Kentucky, and Missouri). These doctors were selected because they were most likely to work with patients in need of opioids and contend with the challenge of differentiating between patients in pain, patients with substance use disorders, and patients who sell medications through illegal markets. Little variation across states was evident in the results, so we analyzed them together, but the research design was set up to find variation if it occurred.
Physicians were selected using a “nested maximum variation sampling strategy” (Chiarello 2023, 2024) designed to capture the broadest range of experiences across states, counties, organizations, and professions. Chiarello contacted physicians through cold calls, emails, and snowball sampling. She conducted 37 in-person interviews with physicians at locations of the physician’s choosing, most often in their office or a coffee shop. Interviews lasted approximately one hour, on average. Questions focused on how physicians decided whether to provide opioids, the rules they established around their practices, how they communicated with patients they were unwilling to treat, and horizontal relationships between healthcare and criminal justice. Stories about horizontal relationships with other physicians emerged organically over the course of the interviews. For this article, Chiarello analyzed how primary care physicians made sense of what would happen to patients they refused, that is, the stories they told themselves about available resources in other hospitals and clinics.
Cross-Case Analysis
Each study was conducted independently with its own research questions. After learning about one another’s research, we realized our studies examine a common object: frontline workers managing marginal or suffering populations. We reanalyzed our datasets with this shared focus in mind and developed the framework around equipped workers and worthwhile labor. Pseudonyms are used throughout to protect the confidentiality of the people we interviewed and observed.
The heart of our comparative analytic process was a series of analytic meetings—typically biweekly—between summer 2023 and summer 2025. Rather than applying a unified coding scheme retroactively across datasets, we exchanged memos (including memos with lengthy data excerpts for us to read and discuss together), drafted collaborative reflections, and debated conceptual distinctions. We reconciled interpretive disagreements through sustained discussion, which led us to revise and reconstruct our analytic categories. Between meetings, each author returned repeatedly to their own primary data—fieldnotes for the ambulance study and interview transcripts for the mandated reporter and physician studies—to assess their alignment with our evolving theoretical framework. While retrospective comparison across distinct studies introduces constraints, qualitative researchers have shown that cross-case analysis can illuminate shared mechanisms that remain invisible within single-case studies (Brayne and Christin 2021; Lara-Millán and Van Cleve 2017; Seim, Corman, and McCann 2022).
Of course, there are limits to this kind of retrospective comparison. Ethical and practical constraints prevented us from exchanging full sets of fieldnotes or interview transcripts. Instead, we shared selected excerpts that illustrated relevant dynamics and used these as comparative anchors. This approach allowed us to draw on the strengths of each method: the ambulance study provides direct evidence of practice, and the mandated reporter and physician studies offer insight into how workers reason about and justify their decisions. At the same time, we remained attentive to the differences between observational and interview-based data. Rather than treating interview accounts as direct proxies for practice (Jerolmack and Khan 2014), we used interviews to analyze the evaluative logics—perceptions of equippedness and worthwhileness—that workers articulated, and we used those frameworks to analyze observed practices in the ambulance study.
Findings
Frontline workers who are called on to respond to people with substantial needs confront an array of tasks. When they feel equipped to do these tasks and see the tasks as worthwhile, they can use their own resources or the resources of their organization to respond directly. Ambulance crews stabilize critically ill and injured patients while transporting them to the hospital. School personnel counsel parents regarding the challenges their children are experiencing. Doctors diagnose and treat patients’ medical conditions. In instances like these, frontline workers claim tasks as part of their realized vocations, using their skills and resources to do work they find worthwhile.
By contrast, when frontline workers encounter barriers that prevent them from realizing their vocations while doing a given task, they are often driven to redistribute clients to other workers and organizations. We identify two dimensions of variation: (1) workers face tasks for which they are more or less equipped with the skills or resources to respond as needed; and (2) workers encounter client problems that they view as more or less worthy of intervention. By “equipped,” we mean the extent to which workers have, or feel they have, the organizational, legal, or technical capacity to complete a given task, rather than whether the task lies squarely in their specific jurisdiction. 1 By “worthwhile,” we mean workers’ moral evaluations of a task, not whether that task falls within their professional turf or professional code of ethics.
We conceptualize three types of work, beyond realized vocation, that reflect different configurations of these two dimensions. One of our empirical cases represents each type, although there is some crossover. First, ambulance crews frequently encounter tasks for which they are ill-equipped and which they find unworthy of intervention. Most calls for ambulance service are deemed “bullshit,” that is, non-medical emergencies that necessitate little in-depth prehospital intervention. Ambulance crews are legally required to transport patients, but in many cases, meeting their needs is beyond the scope of workers’ medical skills and misaligned with workers’ vocation. Second, mandated reporters feel ill-equipped for certain tasks but generally view these tasks as worthwhile. Mandated reporters want some kind of intervention to improve conditions for the children they encounter, but they often feel they lack the resources and skills to intervene themselves. Third, physicians face tasks they are equipped to do but consider unworthy of intervention. Physicians can prescribe opioids for patients experiencing pain; yet doing so carries legal risks and, moreover, physicians see some patients as undeserving of medication. In each of these cases, workers endeavor to redistribute tasks that do not align with their realized vocation.
We argue that these three configurations and the conditions of work they represent correspond to different approaches embraced by frontline workers to redistribute subjects across organizations. As depicted in Figure 1 and detailed in the sections below, workers turn to burden shuffling, aspirational referrals, or abandonment. When workers confront client problems for which they are ill-equipped and they consider unworthy of their intervention, they are motivated to burden shuffle. This is especially true when forces from above, such as legal requirements, prohibit abandonment. We saw this most clearly in the ambulance study. When workers feel ill-equipped but see client problems as worthy of intervention, they are generally driven to make an aspirational referral. We observed this most clearly in the mandated reporter study. Finally, when workers are equipped but confront client problems they see as unworthy of their attention, they tend to abandon their subjects to unspecified organizations and workers. This is especially true when forces from above do not mandate specific kinds of hand-offs. We observed this most clearly in the physician study. We discuss each of these approaches in turn.
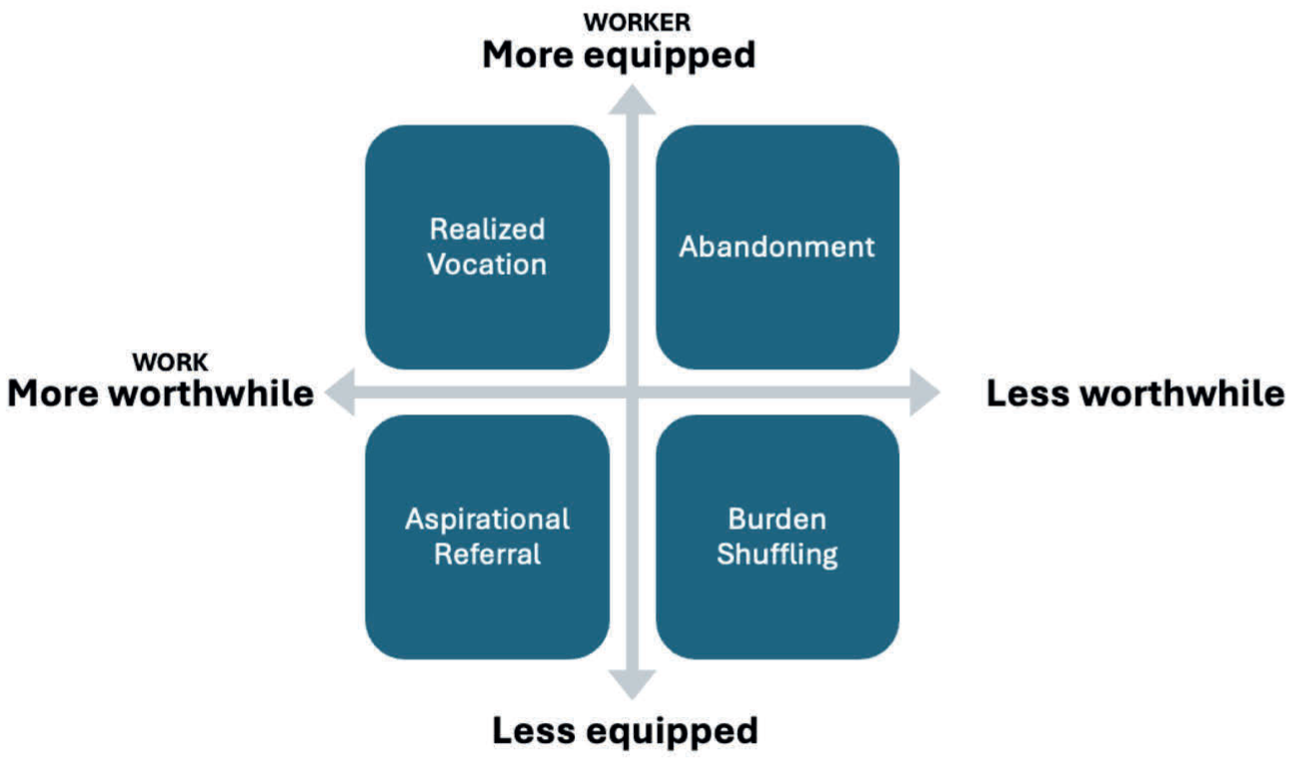
Modes of Redistribution by Frontline Workers.
Burden Shuffling
The first form of horizontal redistribution we discuss, and the one highlighted in past literature, is burden shuffling. In burden shuffling, one party strategically shifts undesirable tasks horizontally onto another to ease their own workload. Prior work (Brooks 2025; Herring 2019; Martino et al. 2026; Seim 2020) emphasizes the vertical structures (e.g., management protocols, client demands) and horizontal linkages (connections across institutions) that enable this strategy. We build on this work by showing that burden shuffling arises most often when workers are ill-equipped to address clients’ needs and when they view the immediate tasks as not worthwhile. Equippedness and worthwhileness together shape how workers judge which responsibilities can, and should, be shifted elsewhere.
This kind of horizontal redistribution was especially common in the ambulance study. Ambulance crews strategically engaged in burden shuffling, most notably through hospital transport decisions. Technically, ambulance crews in the studied county were mandated to transport patients to the closest and most appropriate facility. And per protocols from above, crews had to generally adhere to a policy of “patient choice” in non-urgent cases, which were the vast majority of ambulance calls. In such instances, patients could select, within reason, the hospital to which they were transported.
Crews gamed this policy by coaxing patients into selecting hospitals that would make their shifts easier. Crews preferred hospitals in slower areas of the county, away from busy or otherwise undesirable hospitals, or closer to their sign-out location. Strategic transporting through the “patient choice” policy was especially common during the final hours of ambulance crews’ shifts. Seim observed several shifts where crew members coordinated to persuade patients to choose hospitals closest to their “barn” (headquarters). In these cases, crews were trying to avoid mandatory overtime beyond the required 12-hour shift. Due to lean staffing, crews could only be dismissed if at least eight units were available for new 911 calls. At the end of a shift, after a hospital drop-off, they had to return quickly to headquarters or risk being called out again. To manage this, crews often encouraged patients to pick nearby hospitals, sometimes falsely claiming they had better doctors, food, or wait times.
Burden shuffling took root in a work environment where ambulance crews routinely felt ill-equipped to address the needs of many clients requesting their attention and did not view those tasks as worthwhile. Many calls involved low-acuity psychiatric needs, intoxication, and non-urgent medical problems—issues that were outside the scope of prehospital emergency medicine and therefore tasks that crews felt ill-equipped to treat. Workers often described such cases as “bullshit,” moralizing them as violations of their sense of vocation. These moral framings compounded feelings of futility: even when workers recognized real underlying challenges, they lacked the tools to address them. In response, workers often approached such cases with an eye toward improving their own working conditions. They had to transport the patient somewhere within the boundaries of policy, and they frequently directed low priority patients to facilities they believed would improve their shifts. Policy determined that patients would be transported, but worker discretion shaped how that occurred.
Consider an example of this kind of burden shuffling through strategic transport decisions. One afternoon, toward the end of a 12-hour shift, Seim shadowed paramedics Justin and Max as they responded to a low-priority call for “ETOH” (medical abbreviation for alcohol). “[Hospital X] here we come!” said Justin, signaling to Max that they should steer the patient toward selecting that hospital because it was closest to their sign-off location. They arrived at a corner store to find Frank, a Black man around 60 years of age, sitting and leaning against the exterior wall of the store. His eyes were glazed as he slowly ate some saltine crackers and lunch meat gifted to him by a customer, presumably the person who called 911. Justin and Max both reasoned, out loud, that Frank was too drunk to refuse services because he could not bear his own weight.
Frank’s more sober acquaintance was nearby and chastised him: “See what you started? Now you’re just wasting people’s time because you’re dumb and drunk. These are life savers; they don’t have time for your drunk ass.” Justin and Max were too polite to engage the bystander, but a later conversation confirmed their general agreement. Both considered this to be a “bullshit” call and not one of the “legit” emergencies to which they hoped to respond. Frank’s problem was doubly mismatched with the crew’s intervention toolkit and overall sense of vocation. They were trained and equipped to stabilize and transport bodies in crises that aligned with the relatively narrow framework of emergency medicine. They were not given the tools to connect Frank to substance use treatment services or shelter. Additionally, they were generally disinterested in such non-urgent cases and saw the work of giving simple taxi rides to the hospital as unworthy of time and attention.
Justin and Max turned lemons into lemonade. Protocols required a hospital transport, but the crew was able to bend the rules of “patient choice” to direct Frank toward the hospital closest to their sign-off location. “How about we go to [Hospital X]?” Justin asked. “It’s a great hospital.” Frank seemed genuinely ambivalent about the destination and agreed, much to the benefit of the crew. The selected hospital was technically the third-closest, but close enough that it would be easy to justify under the scrutiny of ambulance supervisors or hospital staff.
When they arrived, the crew met a frustrated nurse. “Where’s he from?” Justin admitted they picked Frank up from a corner store in a neighboring city. “Why did you bring him here?” asked the nurse. “He wanted to come here.” The nurse shook her head in disapproval and then continued with the intake procedures. Frank was triaged to the waiting room following a quick assessment by a physician assistant. After moving Frank to a waiting room chair and completing some paperwork, Justin and Max were cleared from duty and quickly drove to their sign-out location a couple of miles down the road, without being “pulled back” into 911 service.
A similar dynamic unfolded in another case involving involuntary psychiatric transport. While working as an EMT for the same organization, Seim was called to a parking lot where police placed Bill, a middle-aged Black man, on a 72-hour involuntary psychiatric hold. Bill mumbled incomprehensibly in response to Seim’s questions; Seim did not smell alcohol and Bill passed a stroke test. Seim and his partner, EMT Dana, deemed this case not “real ambulance work” because it did not involve a “legit” emergency. Like most of the ambulance workers encountered in the field, they did not consider low-acuity psychiatric calls to be cases they were appropriately equipped to handle or generally worthy of their time and attention.
Protocols required them to transport the patient to a hospital, but the crew exercised discretion over which location: either a psychiatric emergency department or the nearest regular emergency department. Because this case involved an involuntary psychiatric hold, this was done independent of patient choice. As Seim wrote in his fieldnotes, “‘Fuck it,’ I thought to myself, ‘Let’s go to the hospital [for medical clearance]. They [nurses] will get mad, but at least they can’t turn me away [unlike the psychiatric facility, which can turn crews away from bringing ‘medical’ cases].’” The ambulance crew shuffled the case to the emergency department, where a nurse scolded Seim for the transport decision. Still, he and his partner concluded this was the least troublesome choice. The alternative transport to the psychiatric facility might have involved resistance, or outright rejection, from nursing staff. It was easier and safer to shuffle the burden onto the emergency department, and the EMTs did precisely that.
Burden shuffling also appeared in our other two cases, although not as prominently. A police officer in the mandated reporter study described calling CPS regarding a toddler who wandered into the street, explaining: “I can’t sit there and babysit a 2-year-old.” Here, CPS became the horizontal recipient of a task the officer wanted to shuffle off to someone else. In the physician study, general practitioners shifted opioid prescribing to pain specialists, framing referrals as necessary to avoid legal risk or undesirable patients. Yet, as we will discuss, pain specialists often tried to avoid these cases as well, creating referral loops more akin to burden displacement than problem resolution.
Although we saw examples of burden shuffling across all three cases, it was most evident in the ambulance case, where the conditions of work make this mechanism of redistribution especially likely. Protocols from above require ambulance crews to transport patients, creating the structural conditions for redistribution. Ambulance crews typically have some discretion, though, as most cases are not medically urgent. In a context of ill-equipped workers confronting tasks they do not consider worthwhile, crews turn to burden shuffling, redistributing patients to hospitals based on ambulance crews’ interest in improving the conditions of their own work.
Aspirational Referrals
In the mandated reporting case, like the ambulance case, frontline workers felt ill-equipped to perform particular tasks—in this case, responding to children in families facing adversity. Unlike the ambulance case, however, mandated reporters saw this work as worthwhile: important for someone (even if not them) to do. This combination of factors leads to horizontal redistribution in the form of aspirational referrals. In aspirational referrals, workers shift people to adjacent systems and presume these other systems will be helpful, or at least more helpful than the focal worker can be. Like burden shuffling, aspirational referrals involve frontline workers actively transferring subjects across organizations. But unlike burden shuffling, frontline workers pursuing aspirational referrals justify their decisions as beneficial for clients. Whereas burden shuffling tends to emphasize the interests and conditions of workers, aspirational referrals emphasize the interests and conditions of clients, as frontline workers invoke hope that a worker in another organization will be better suited to address the problem.
Like ambulance workers, mandated reporters identified multiple constraints that left them poorly equipped to improve families’ conditions: extensive demands on their time, lack of knowledge about social service options, and bounded scopes of work (both practical, e.g., when workers do not visit homes, and jurisdictional, e.g., when workers do not focus on child or family issues). As in the ambulance case, laws place vertical pressures from above on frontline workers to respond. However, unlike the “bullshit” work of ambulance crews, mandated reporters viewed the task of responding to children whose families faced adversity as important and worthwhile, regardless of legal pressures.
For example, a state trooper named Thomas said he would call CPS regarding children exposed to domestic violence even absent any legal or departmental policy requirement. He explained this by referencing his role on the local juvenile review board, where, he said, “I see the aftermath on these kids . . . the kids that you want to reach out and just say, ‘Okay, it’s gonna be okay,’ and I can’t.” Based on this experience, Thomas viewed intervention with families experiencing domestic violence as worthwhile—a means of preventing intergenerational violence and police contact. Thomas said, “I want to be able to give them the services that they need, so maybe somehow I won’t be dealing with them, or the next generation of cops or troopers will not have to arrest little Mikey because all he’s seen is Dad abuse Mom.”
However, Thomas also described feeling stretched thin in his job, with substantial demand on five troopers covering a large geographic area. Thomas rattled off a litany of tasks that necessitated his response: car accidents, speed enforcement, synagogue safety, mental health breakdowns, alarms going off, house checks, and more. Although he wanted families experiencing domestic violence to get counseling, he did not feel equipped to make this connection himself, and he was eager to redistribute what he could:
What if someone said, “Well, why can’t you all talk to the parents and have them get into a place where they can receive counseling?”
I could, but I know I’m gonna say this, I know it’s gonna come out wrong. They have the ability to focus on just this portion of the whole thing. If they can focus on this, I can focus on that. I can’t focus on the needs of the children and be able to have resources dedicated to here [i.e., to police work]. Like I said, we don’t have enough resources here. We have to mix and match and patchwork everything.
Feeling ill-equipped for a task he saw as worthwhile, Thomas turned to CPS as an aspirational resource, one he hoped would be able to intervene with families in ways he could not.
Legal mandates in Connecticut do not categorically require CPS reports when children are exposed to domestic violence; mandated reporters must decide whether they feel children are at risk of serious harm. Mandated reporters have substantial latitude as they interpret broad legal definitions of child abuse and neglect. They described using their discretion to leverage CPS referrals aspirationally, calling on CPS to improve conditions for families as much as (or even more than) to investigate child maltreatment. When Fong asked Thomas about discretionary cases, he invoked the resources he believed CPS could offer families, resources he felt ill-equipped to provide:
What’s an example of a situation like that where you could go either way in terms of making a call?
It’s your feeling. To say that, hey, Mom and Dad may or may not have enough food, have enough services. Let’s call CPS and say, “Hey, I know you don’t have unlimited services, but you have more services that you can give to this person than I can. You have more stuff . . .” If I say, hey, let’s call CPS and see if we can get—even maybe Mom gets counseling. That’s more than I can do. . . . So sometimes we’ll call just to maybe help the family out in the long run, because CPS can do more for them.
Thomas acknowledged that CPS did not have “unlimited” resources, but he believed CPS had more help to offer, so he described reporting based on expectations of CPS assistance. Mandated reporters commonly presumed CPS had greater access to or knowledge of local social services that they could use to assist families. Based on this presumption, mandated reporters framed their referrals in terms of aspirations to improve families’ conditions, rather than shuffling burdensome work.
Frontline workers in more support-oriented organizations also called on CPS as an aspirational resource. For example, Shannon, a middle-school-based mental health clinician, described calling CPS regarding a 14-year-old student, Adela. Shannon told CPS that Adela’s adult brother was making Adela feel uncomfortable by looking at pictures of topless women on his phone and engaging in sexual behavior with his girlfriend in front of Adela. Adela also said her 5-year-old brother had reached up her skirt and tried to touch her multiple times; when Adela told her parents, her parents brushed it off. Shannon had recommended outside counseling for Adela, “’cause I really think she needs it.” In the interview, Shannon discussed at length her concerns about the family, including estranged relationships, past traumas, and other family dynamics Shannon felt were being pushed under the rug: “Those dynamics concern me because I feel like [Adela] feels caught in the middle of that.” Additionally, Shannon said, Adela was “parentified,” taking on substantial family responsibility and stress. Shannon concluded, “She’s just this floating lost girl when she’s in school who really doesn’t have many friends, who’s depressed, anxious. I just feel if she had an outside therapist, some of this trauma might be able to be addressed more intensely.”
Even though Shannon was a clinician who counseled students, she did not feel equipped to provide this support. Shannon explained, “It’s really hard in the school because I can only capture her for 30 minutes here, or 35. I’m lucky if I get 45 minutes because I can only pull them during certain classes.” Shannon could not give each student the attention they needed: “I have had to cap my caseload because there’s just not enough hours in the day for me to see them all.” A student dropped in during our interview, which she said was typical. As we wrapped up, she sighed, “I wish there was three of me.” In Adela’s case in particular, Shannon felt it would be helpful to talk with Adela’s parents, but transportation and other barriers precluded the parents from coming to the school, and Shannon did not do home visits in her role.
In this context, Shannon turned to CPS: “I know CPS can put in place in-home family therapy—[a psychiatric treatment program], for example. They can ask for that. I think that would be very beneficial, just so the family can learn how to communicate better and be on the same page more and be a little bit more open and give support to Mom and Dad. It sounds like they’re both extremely stressed. They have a lot of, as you know, socioeconomic issues.” Like almost all other interview participants, Shannon said she would have reported the case even without the legal mandate. Shannon clarified that she did not want Adela to be removed from her home; rather, she sought to “get the family some outside services.” Labeling Adela’s experiences as suspected child maltreatment is not necessarily self-evident. Frontline workers draw on racialized, classed perceptions of low-income families of color, like Adela’s, as they weigh their options (Fong 2023). Clinicians might reasonably make different judgments in similar cases, and an emerging movement encourages professionals like Shannon to offer support to families themselves, rather than immediately calling CPS (Prax 2025). Shannon, however, emphasized how Adela would benefit from her choice to redistribute this task to CPS.
Like Thomas and Shannon, almost all mandated reporters interviewed referenced the services and referrals CPS could offer. Notably, CPS can also remove children from the home, a power that is front of mind for parents (Fong 2023). However, when mandated reporters invoked CPS’s coercive authority, they portrayed it as a useful tool they could call on to help children and their families. From this perspective, calling CPS was in line with, not in tension with, their aspirations. Pressure from CPS, they reasoned, could nudge parents to change their behavior by giving them a “wake-up call,” which they hoped would ultimately improve conditions for the children. There were a few exceptions in the data—mandated reporters who framed CPS’s coercive power as detrimental to children if deployed unnecessarily, due to the stress imposed on families—and these workers expressed more hesitation regarding referring families to CPS.
Although aspirational referrals were most prevalent in the mandated reporting case, this model emerged in our other cases as well. Ambulance crews, for example, did not always see non-urgent patients as burdensome. Seim observed several incidents in which crews reimagined themselves as ill-equipped social workers and strategically transported patients to hospitals they thought had better social services. For example, in one case, a crew transported a patient to a less convenient hospital because they believed it was the only facility that had a social worker available to aid their patient who needed social services beyond emergency medicine. Many crews understood their patients were structurally excluded from primary care, and they imagined the county’s flagship public emergency department could potentially refer them to specialists covered by Medicaid. Crews often believed that this hospital would be an ideal place to transfer patients for their own good. In line with the mandated reporting case, such incidents happened when patients, for whatever reason, appealed to workers’ sympathy and empathy. Transportation destinations were reimagined not as spaces to dump burdensome cases, but as spaces better equipped to relieve patient suffering.
Likewise, general practitioners sometimes highlighted skills and resources that pain specialists had that general practitioners lacked. When asked how he managed chronic pain with opioids, a family medicine physician responded, “It depends on the patient. If the patient says, ‘Doc, I’ve been getting my Percocet every day three times a day for the last 25 years, you’re not going to change it, I don’t care what you say,’ then that patient should probably go to pain management. Because that’s what pain management docs do. They deal with those patients all day, every day. Perhaps there are better, longer-acting interventions that they can do, as opposed to just pills.” This physician imagined a more robust toolkit at the pain specialist’s disposal that included resources other than opioids, and he used that assumption to justify the aspirational referral. Like mandated reporters who assume CPS workers have more or better resources to help clients, general practitioners assume—largely erroneously in this case—that pain specialists are better equipped to deal with chronic pain.
Aspirational referrals as a mechanism of redistribution are especially prominent when frontline workers feel ill-equipped to address people’s needs yet see the work of doing so as worthwhile. Aspirational referrals help resolve this dilemma, as frontline workers can send clients to another organization they hope can improve conditions. Even if workers recognize that the receiving agency may not actually be able to remedy the problem, this hope drives redistribution.
Abandonment
In the ambulance case, workers burden shuffled because they were ill-equipped to do a task they did not perceive as worthwhile. In the mandated reporter case, workers made aspirational referrals because they were ill-equipped to do a task they perceived as worthwhile. What happens when workers are equipped to do a task that they do not perceive as worthwhile? If law allows, they can deploy a third strategy: abandonment. Abandonment is declining to do the task and leaving clients without resources or support. Of the workers in this study, only physicians engaged in abandonment: they were capable of prescribing opioids, but refused. In the physician case, abandonment means firing a patient without directly handing them off to another provider, or purportedly handing them over to another provider who is unlikely to take them. Often, physicians justified their choice by citing patients’ behavior, such as failure to follow rules the clinic set for them. We argue that physicians abandon patients on opioids because they do not see the task of prescribing opioids to these patients as desirable or worthwhile. Two vertical conditions shape this perception: from above, the legal risks of prescribing opioids, and from below, pain patients whose treatments have been stigmatized. Moreover, unlike the other two cases in this study, horizontal opportunities enable physicians to abandon patients despite being equipped to help them.
Legal pressures make the task of prescribing opioids to pain patients undesirable. Physicians can prescribe opioids, but guidelines from the Centers for Disease Control and Prevention (2016) and enforcement actions against over-prescribers by medical boards and the Drug Enforcement Administration make opioid prescribing legally risky (Chiarello 2024). Physicians would be free to turn patients away outright instead of (ostensibly) handing them off were it not for a different set of pressures from above: the ethical obligations that prohibit abandonment and require physicians to care for patients (American Medical Association n.d.). Conflicting pressures from above to prescribe conservatively and to care for patients, paired with pressures from below from struggling patients seeking relief, put physicians in a bind. Physicians allay these ethical concerns by invoking an “imagined remedy,” another doctor who will care for their patients. What sets abandonment apart from burden shuffling and aspirational referrals is that the horizontally-adjacent professional who will purportedly take cases that are not deemed worthwhile may not accept these cases or may not even exist. In the other two cases, a specific organization is obligated to respond to client problems (an ambulance or CPS). No law requires that patients receive access to opioids.
Unlike typical medical referrals, physicians are disinterested in engaging in warm hand-offs for opioid provision, largely because most physicians do not see prescribing opioids as important or worthwhile, and they would feel that way even absent the legal risks. Many physicians claimed that evidence to support opioids for chronic pain was weak at best, so they focused on getting patients off of opioids instead of ensuring they could stay on their current dose. Doctors who do prescribe opioids set strict boundaries, such as requiring patients to sign a pain contract, submit to urine drug screens, and acknowledge surveillance in a statewide database called the prescription drug monitoring program (Chiarello 2024). Physicians highlighted how patients fail to adhere to the “rules” prescribers set for opioid use. They also blamed patients for their own plight in a form of responsibilization, placing responsibility on the patient’s shoulders (see Hannah-Moffat 2013). Patients who present as “undeserving” (Pryma 2017; Radcliffe 2011), as measured by prescription surveillance technology, find themselves cut off opioids or fired from the practice (Chiarello 2024).
For example, Blake, a pain specialist, fires patients when they test positive for illegal drugs. The scenario is this: “They’ve had some positive drug screens, and they do nothing else to help themselves and are not a part of the program and they’re not, you know, being productive. Or they’re staying at home and just lying in bed and doing nothing and taking opioids.” When this happens, Blake says, “you’re done,” and he quickly tapers the patient’s opioid prescription to zero. Even though Blake is equipped to prescribe opioids, when he no longer sees this task as worthwhile—when he believes patients are not taking responsibility for their lives—he abandons it, cutting patients off from medication. Whereas workers in the mandated reporter case believe it is important for someone to do the task, in this case, physicians like Blake are not especially interested in ensuring that “undeserving” patients are prescribed opioids. Physicians constructed patients as less deserving for failing to take responsibility for their own care or failing to follow the rules created by their physicians.
Ethics temper how Blake justified his choice. He used the language of redistribution to point to another provider who might care for the patients he cast off: “I’ll offer them phone numbers for either methadone clinics or other places that can help with coming off of opioids or any kind of addiction, but you know, let’s be honest. Most of those places are either full or expensive. And not all those patients have the resources to do that . . . but I can’t conscientiously keep prescribing when I know somebody’s taking a medication the way it’s not prescribed or they’re taking other things at the same time that put them at risk for overdose.” Blake did not want to continue prescribing to these patients, nor did he think it was essential for another provider to do so. Blake imagined somewhere else that would provide care while acknowledging that those places are usually unavailable or inaccessible.
As we see in Blake’s case, physicians are essentially abandoning patients, even though their profession forbids it. Chiarello asked Neil, a general practitioner, whether he considered cutting patients off a form of abandonment. Neil replied, “abandoning seems a little bit of an exaggeration when the contract is violated, because that’s the very nature of the contract.” Neil framed the patient as guilty for violating the rules established by the pain contract: “I mean, that’s written in the rules, that you do this.” Patients who disobey “have to go elsewhere and it’s harder for you to get what you want.” Neil thought patients deserved those challenges if they were “not willing to play by the rules that make [him] feel comfortable prescribing narcotics.” He did not believe it was essential for these patients to be prescribed opioids. When asked if he was sympathetic to the idea that pain patients might be suffering because they cannot get access to their medications, he countered, “I think there’s always another doctor. There’s always another doctor.” Neil further explained, “I think that their inconvenience by having to find one would make them less likely to breach contracts in the future.” Not only does Neil imagine a mythic elsewhere where another doctor will provide care, but he considers the difficulty of finding a new provider a suitable punishment for patients who fail to obey the contract.
Beyond presenting tasks that workers are equipped to do but feel are not worthwhile, specific contours of medical work make abandonment more likely in this case than in others. First, the stakes of action versus inaction are flipped. For doctors, the legal risk largely lies in providing legally inappropriate care, that is, prescribing opioids for non-medical use. By contrast, in the other cases, failing to act (failing to transport a patient or report child maltreatment) poses the greater legal risk. Unsurprisingly, then, we see inaction from physicians. Second, no physician must ultimately take responsibility for prescribing opioids. Unlike the ambulance case, in which the hospital is the ultimate (if impermanent) endpoint, and the mandated reporter case, in which CPS must investigate referrals that meet statutory criteria, for pain patients on opioids, there is no physician who must ultimately provide care, so each physician can abandon without consequence. Physicians’ discretion over which patients they treat reflects their outsized professional power compared to other workers who exercise discretion in more constrained conditions. Finally, physicians operate in a looser interprofessional network than the workers in the other two cases. Most doctors work in large medical systems where they communicate through charts and referrals instead of face-to-face interaction, or they work in separate organizations where they may have no interaction at all. Unlike ambulance workers, doctors rarely see in real time how others react to having the burden shuffled onto them, and unlike mandated reporters, they do not talk with agency workers who can spur CPS investigators into action or inform them a case does not meet criteria for investigation. Without seeing or hearing pushback, physicians can imagine it does not exist.
Where vertical structures enabled abandonment in the physician case, they prohibited abandonment in the ambulance case. As noted above, strong legal restrictions prohibit paramedics and EMTs from abandoning patients. Anyone who calls 911 and articulates a medical response is entitled to a hospital transport in the studied county. Some jurisdictions allow for “paramedic-initiated refusals,” where ambulance crews can reject a transport based on the non-severity of a case, but focal county regulations explicitly prohibited this practice. In rare incidents, ambulance crews reported coaxing and coercing patients into rejecting hospital transports by having them sign an “against medical advice” (AMA) form. We might interpret these cases as efforts to abandon. There was one “frequent flyer” patient, for example, that some paramedics said they occasionally paid $5 or gave food to in exchange for having him sign an AMA form, but Seim never saw this directly. In fact, he observed two failed attempts to use this strategy. And because refusing to provide ambulance services was seen as a major professional and organizational sin, with consequences that were assumed to be severe (e.g., job loss), he never witnessed outright abandonment during his two-year field study.
We likewise did not observe examples of abandonment in the mandated reporter case, although our research design may have precluded us from identifying them. Mandated reporters may not wish to disclose instances of abandonment in an interview because those actions may violate legal reporting requirements. Moreover, in this study, most interview participants were selected because they had recently reported a case to CPS, so individuals who were more likely to abandon may not have been included in the sample. In the mandated reporting context, abandonment might look like a police officer seeing a child with bruises and suggesting the parent request social services or medical help, without directly referring the family to another system. Media coverage of child fatalities or near-fatalities have described instances like this, in which mandated reporters declined to pass cases to CPS or any other entity. For example, during Fong’s fieldwork, a state review panel wrote that a service provider had been working with the parents of a 2-month-old. This provider “reported having concerns about the parents due to inquiries made about shaken baby syndrome and reports that one of the parents was ‘rough’ with the child. No call was made to the [CPS] Hotline until the child’s admission to the [pediatric intensive care unit]” for extensive injuries (RI Office of the Child Advocate 2017:15). Beyond these examples that come to public attention, instances of abandonment may be occurring in cases that do not end tragically.
In the physician case, horizontal redistribution takes the form of abandonment that is reframed as an imagined remedy or a mythic elsewhere where other doctors will care for patients they refuse to see. This symbolic construction of other workers who will pick up the slack serves a similar function to the material hand-offs evident in the other two cases. Doctors can protect their vocation without (in their minds) compromising their ethical commitments by placing blame on the patient. This strategy is made possible by the lack of legal requirements, present in the other two cases, that create higher stakes of action versus inaction for doctors.
Discussion and Conclusions
Patterns of Redistribution
Frontline workers shape the distribution and flow of resources, services, and sanctions. Under vertical pressures, workers seek horizontal release valves. Previous scholarship examining horizontal redistribution has centered on workers’ efforts to “shuffle” or “offload” burdensome work (Brooks 2025; Herring 2019; Lara-Millán 2021; Seim 2020; Sirois 2023). However, we conclude that burden shuffling is the product of specific conditions: when workers are ill-equipped to perform tasks they do not consider worthwhile. Past research leaves open questions: What happens when workers are equipped? What happens when tasks are seen as worthwhile?
Our study reveals that the nexus of the extent to which workers feel equipped to perform tasks and the extent to which they consider tasks worthwhile shapes how and why workers use different tactics across institutional contexts. The significance of these factors becomes clear when comparing cases to one another and to the ideal case of realized vocation. Realized vocation is what workers strive for; it occurs when people bring their skills and resources to bear on tasks they consider worthwhile. Workers eagerly perform these tasks and shield them from other workers who might encroach on their domain (Abbott 1988). However, when faced with tasks beyond their realized vocations, workers redistribute them: they shuffle burdens, refer aspirationally, or abandon tasks. All three tactics rely on other workers (real or imagined) to pick up, often reluctantly, the tasks the focal worker rejected. Across our cases, burden shuffling was the most common form of redistribution, but aspirational referrals were relatively common in the mandated reporter case, and abandonment was relatively common in the physician case.
In some cases, workers lack the training, resources, or skills necessary to perform a task. For example, ambulance workers are poorly equipped to care for patients long-term and to handle social suffering that is not medical in nature; mandated reporters feel poorly equipped to intervene with families as thoroughly as they believe is necessary (e.g., through repeated home visits or by ensuring that families participate in therapeutic services). By contrast, physicians are well-equipped to prescribe opioids. If equippedness were all that mattered, we would expect physicians to perform the task and the other workers to refer. Only when we view tasks through the lens of worthwhileness can we understand why all three workers refer. Doctors refer tasks for which they are equipped when they do not consider the task worthwhile: in the context of an opioid crisis that has demonized painkillers and the people who use them, doctors have begun to see long-term opioid prescribing for chronic pain as unnecessary and harmful.
By contrast, ill-equipped ambulance workers and mandated reporters refer cases to adjacent workers (hospitals and CPS, respectively) but differ in how and why they refer because of how worthwhile they consider the task. Mandated reporters encounter problems that affect children, considered innocent and deserving, a sharp contrast to the problems ambulance crews conceive as “bullshit,” brought by patients who are often looked on unfavorably as either “stupid” or “selfish” (see also Seim 2020). Mandated reporters explain their referrals using the language of connecting families with more and better resources. Ambulance workers, in turn, refer patients invoking the language of “burden” that suggests they are protecting their own vocations from “bullshit” work. Varying perceptions of tasks as worthwhile help explain why mandated reporters refer by invoking clients’ needs, whereas ambulance crews refer with an eye to their own needs.
The broader legal context also structures workers’ tactics by creating vertical constraints and horizontal opportunities. Law imposes different risks across our cases. For ambulance crews and mandated reporters, inaction poses the greatest legal risk. Workers who fail to transport patients or report child maltreatment violate the law. Those who perform these tasks recognize the legal pressure bearing down on them. At the same time, the law has created horizontal opportunities for ill-equipped workers to hand off cases to designated agencies like hospitals and CPS that are legally required to do certain work (medical intervention and child maltreatment investigations, respectively). In these contexts, workers rarely abandon clients. In the physician case, intervention poses the greatest legal risk. Physicians are equipped to prescribe opioids, but they can face severe legal consequences, such as losing their medical license or incarceration, if they provide them to patients who use them non-medically or sell them. The prohibition against abandoning patients is an ethical rather than a legal requirement. Doctors skirt this requirement by espousing narratives that invoke another doctor willing to treat, or that blame the patient for denial of care. Some physicians will continue to treat the patient for other conditions but will no longer provide opioids for pain. In this case, silent law and toothless ethics combine to create a scenario in which as long as doctors frame their actions as something other than complete desertion, they can put the burden down and leave in a way that other workers in this study cannot.
What happens after workers redistribute tasks? Although this was not a primary focus of the present analysis, our data suggest variation along this line as well. Workers on the receiving end can, to varying degrees, resist the tasks that come to them, reanimating horizontal pressures on the workers who send them. Ambulance workers who come face-to-face with nurses at the hospital experience resistance in real time. The nurse who scoffs or yells at the ambulance crew sends a clear message that the crew should think twice before bringing unwanted cases to her hospital again. Nevertheless, hospitals must accept most ambulance transports, so patients get redistributed to the hospital. Likewise, CPS is supposed to accept referrals that meet statutory criteria to investigate. Hand-offs to CPS are typically mediated by phone, and mandated reporters do not necessarily speak directly to CPS investigators. If investigators are frustrated by the cases handed off to them, this frustration may be largely invisible to mandated reporters, so families get redistributed to CPS. In the physician case, referrals take the form of a “cold handoff,” and the receiving entity—the pain specialist—is not required to see patients who are referred. Pain specialists may refuse to take patients long-term, or primary care physicians may refer patients and refuse to take them back even if the specialist refuses to treat. General practitioners’ referrals to pain specialists often manifest as referrals to nowhere.
In a context of fragmentation in which workers feel inadequate or disinterested in addressing the problems at hand, referrals do not solve problems so much as move them, at least temporarily. All three of the processes we describe—burden shuffling, aspirational referrals, and abandonment—fail to meaningfully resolve people’s challenges. Referrals to punitive institutions may even increase precarity and stress (Fong 2023; Herring 2019). Frontline workers themselves may not know what others can do, and they sometimes recognize that the destinations to which they are referring cannot fully meet clients’ needs. But, facing tasks beyond their realized vocations, they push clients onto other workers. These horizontal redistribution processes are often grounded in the presumption that some worker somewhere will take care of the problem, but viewed holistically, they likely will not. Clients are given the runaround without finding relief.
Implications for Scholarship on Frontline Governance
Our cross-case comparison affirms that responses to social suffering are not simply the aggregation of individual frontline decisions made within siloed institutions. Rather, they are the product of a dynamic circulation process in which frontline labor is divided across fragmented and often contradictory organizations (Barnard 2023; Comfort et al. 2015; Gong 2024). In this regard, we extend a growing recognition that the redistribution of clients merits examination as a governance practice in its own right. We advance this conversation by moving beyond the assumption that redistribution primarily takes the form of burden shuffling (Brooks 2025; Herring 2019; Lara-Millán 2021; Seim 2020; Sirois 2023). While burden shuffling is indeed important and common, we show it is only one of several strategies. In our framework, patterns of redistribution hinge on two conditions shaped in large part by the material and moral dimensions of work: whether workers feel equipped to handle a task and whether they see that task as worthwhile.
Research on street-level bureaucrats has focused on the discretion these workers exercise as they materialize public policy. Frontline workers use discretion to differentially dispense resources and interventions (Dubois 2012; Lipsky [1980] 2010; Maynard-Moody and Musheno [2003] 2022; Zacka 2017). Beyond distributing resources to clients, frontline workers also (re)distribute clients horizontally across organizations (Lara-Millán 2021; Sirois 2023), yet we have had little insight into how they exercise discretion in this redistribution. All the workers we study have some degree of discretion: ambulance crews decide which hospital to transport a patient to, mandated reporters use their judgment to determine whether a situation constitutes suspected child maltreatment, and physicians decide which patients to accept and which patients to fire. We use these cases to theorize factors that structure how frontline workers use discretion as they redistribute tasks. Ultimately, our framework illuminates how frontline workers shed, transfer, or redirect tasks in structured and predictable ways.
Implications for Scholarship on Organizational Fragmentation
This article also speaks to broader organizational scholarship on fragmentation, boundary-spanning, and the restructuring of responsibility in contemporary workplaces. In a neoliberal era marked by privatization, financialization, and the diffusion of market logics, organizational systems increasingly operate not through cohesive bureaucratic hierarchies, but through fragmented and contradictory fields in which tasks, authority, and risk are distributed across multiple organizations. This dynamic has been observed across several strands of research: in classic studies of boundary-spanning roles that connect otherwise distinct organizations (Aldrich and Herker 1977); in analyses of dignity, conflict, and coordination within complex work systems (Hodson 2001); in accounts of how financialization restructures firms and redefines managerial priorities (Lin 2016); and in research on the “fissuring” of employment through outsourcing, subcontracting, and other forms of organizational disaggregation (Weil 2014). Taken together, this literature underscores that fragmentation is not merely an empirical condition but a defining feature of the political economy of work, shaping how institutions coordinate labor, distribute risk, and assign moral responsibility.
Our analysis contributes to this literature by specifying how frontline workers in a devolved, delegated, and discontinuous governance system navigate fragmentation through horizontal redistribution strategies. This redistribution is not uniform; rather, the material and moral conditions of work structure the form of, and justifications for, redistribution. Specifically, perceptions of equippedness and worthwhileness shape whether workers push tasks across boundaries as burdens, refer them aspirationally in the client’s assumed interest, or abandon them altogether. Rather than treating fragmentation as a structural backdrop, our framework shows how everyday labor practices reproduce fragmentation at the ground level, as workers, constrained and enabled by both vertical and horizonal relations of production, continually reallocate responsibilities across organizational lines.
Limitations and Directions for Future Research
There are, no doubt, limits to the research presented here. First, as previously noted, there are important methodological differences across the three cases. The ambulance study is based on ethnographic observation, while the mandated reporter and physician studies rely on interviews. Observations are generally best suited for capturing practice (what people do), whereas interviews are typically best for capturing perception (what people say they think). Our analysis draws on both forms, but Seim did not conduct in-depth interviews with ambulance workers about how they made sense of their work, and neither Chiarello nor Fong directly observed the redistribution practices they describe. Each method carries limitations: interviews do not directly reveal practice, and observations do not always reveal workers’ interpretations. But together they can help reveal critical dynamics of frontline work.
Second, although we worked diligently to analyze similarities and differences across our cases, we collected all data before beginning this collaborative project. This meant we were limited by the notes taken in the field and the questions asked prior to our collaborative analysis. This retrospective analytic strategy introduces constraints—our original data were gathered under different orienting questions and theoretical lenses, although each project included processes of redistribution as a central focus—but it also offered an opportunity to build comparative insights from independent projects that converged on related patterns.
Third, our focus on workers necessarily limits what we can conclude about the downstream effects of redistribution for clients themselves. We infer that these practices contribute to the “mazes,” “runarounds,” and institutional loops documented in prior research (Comfort et al. 2015; Halushka 2023; Paik 2021; Sered and Norton-Hawk 2014), but the data we analyze here do not allow us to directly observe clients’ longitudinal experiences as they are moved between organizations. Understanding how different forms of redistribution shape clients’ trajectories remains an important direction for future work.
These limitations call for additional inquiries into how frontline workers redistribute work, not only within a fragmented system of state governance, but also across private, nonprofit, and hybrid organizational sectors. As noted above, future research could examine the consequences of redistribution for clients themselves, helping to better connect the research on redistribution with scholarship on client “runarounds” and institutional churn. It would also be fruitful to identify the conditions under which redistribution fails so completely that clients fall through the cracks. Given the notoriously fragmented U.S. welfare state, comparative work, both within the United States and across national contexts, may further illuminate how different governance regimes and degrees of organizational integration shape the redistribution strategies workers pursue. For example, we might see less abandonment in more comprehensive healthcare systems, such as Veterans Affairs, integrated managed care consortia (e.g., Kaiser Permanente), and Federally Qualified Health Centers. Finally, as new technologies—including AI-driven triage systems and decision-support tools—begin to reorient frontline work and reshape inter-organizational linkages (Benjamin 2019; Brayne 2020; Chiarello 2023; Eubanks 2018), research should investigate whether such systems mitigate, displace, or amplify the horizontal redistribution patterns identified here. We see these paths not simply as opportunities to extend our framework, but as possibilities to complicate and reconstruct it in light of additional empirical cases that will emerge in research beyond our three study sites and contribute to studies of work writ large.
Footnotes
Acknowledgements
We thank the American Sociological Review reviewers and editors for their thoughtful critiques and recommendations. We also gratefully acknowledge Kathleen Griesbach, whose detailed comments on an earlier draft helped us clarify and articulate our contribution. Our manuscript benefited from feedback received at the 2024 American Sociological Association annual meeting.
Authors’ Note
Authors are presented in alphabetical order to reflect equal contributions to the article.
Data Note
The data for this study are not publicly available due to Institutional Review Board (IRB) restrictions and participant confidentiality protections.
Funding
The NSF CAREER Award #1753308 supported Chiarello’s work, and the Doris Duke Fellowship for the Promotion of Child Well-Being supported Fong’s data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.