
Abstract
Background
Injury to the celiac artery secondary to a blunt mechanism of trauma is an extremely rare injury that accounts for only 1%-2% of all visceral vascular lesions. Although rare, this injury is associated with significant mortality. Despite this high mortality, there are currently only a few published case series of blunt celiac artery injuries in the literature. This study sought to review all cases of blunt celiac artery injuries that presented to our Level I trauma center over a 5-year period.
Methods
This was a retrospective chart review of all patients who presented with a traumatic blunt celiac artery injury between January 2012 and March 2017.
Results
A total of 10 patients met the inclusion criteria for this study. The majority of patients were male (7/10, 70%), the average age was 38.3 ± 16.1 years, and overall mortality was 20% (2/10). On average, patients spent 10.2 ± 6.5 days in the hospital, 4.4 ± 4.5 days in the ICU, and 1.6 ± 2.0 days on the ventilator. The majority of patients presented with either an intimal dissection (3/10, 30%) or an intraluminal thrombus (3/10, 30%). Other injuries included pseudoaneurysms (2/10, 20%), complete avulsion (1/10, 10%), and an intimal dissection with thrombus (1/10, 10%). Of these injuries, 2 (20%) were noted to have retrograde flow on imaging studies including computed tomography angiography and a visceral angiogram. The majority of patients (8/10, 80%) were managed nonoperatively, and 5 (50%) patients were discharged home on aspirin. One patient who was initially managed nonoperatively required an unplanned return to the operating room for ischemic bowel, liver, and stomach. There were no other complications noted.
Discussion
Traumatic blunt injury to the celiac artery is rare. Although there are multiple treatment options, there is currently no consensus in regard to management guidelines. In this case series, the majority of patients were successfully managed nonoperatively suggesting that a selective approach for intervention on patients with a blunt celiac artery injury should be considered.
Introduction
Vascular injuries account for around 3% of all trauma-related injuries. 1 Of these injuries, the vast majority involve the extremities and are mostly secondary to penetrating trauma. Abdominal vascular injuries, in particular, account for only 5%-30% of all traumatic vascular injuries, and, again, are most often secondary to penetrating trauma. 2,3 These injuries represent a challenging injury pattern, as patients frequently present in profound shock secondary to intra-abdominal blood loss. Furthermore, trauma to the intra-abdominal and mesenteric blood vessels is oftentimes associated with multiple concomitant visceral injuries. 2,4,5
Within the named abdominal vessels, injury to the celiac artery is extremely rare, especially from a blunt mechanism of trauma. Though rare, these injuries are highly lethal with reported mortality rates of anywhere from 38% to 62%. 6 Injury patterns also vary and can include complete avulsion, intimal flaps, thrombosis, or pseudoaneurysms. Given the wide variety of the type of injury that is seen, management strategies are also varied and can range from medical management with antiplatelet therapy and therapeutic anticoagulation to endovascular therapy and open ligation. 6
Currently, there are only a total of 11 reported cases of blunt celiac artery injury in the literature. 2,3,7,8 The most recent series published by Asensio et al, included a total of 13 celiac axis injuries, only one of which was secondary to a blunt mechanism of trauma. 8 Given both the rarity and complexity of this injury complex, this study sought to review all cases of blunt celiac artery injuries that presented to our Level I trauma center over a 5-year period.
Methods
This was a single-center, retrospective review of all patients who presented to Grady Memorial Hospital with a traumatic blunt celiac artery injury between January 2012 and March 2017. Following approval from the Emory University Institutional Review Board, patients were identified using the Trauma Registry of the American College of Surgeons. Blunt celiac artery injuries were diagnosed based on initial imaging findings at the time of patient presentation or through a review of the operative report. Data were then collected by thoroughly reviewing each patient’s medical record including their entire hospital course and operative log. Statistical analysis was then performed using both Microsoft Excel and GraphPad Prism version 6.0 for Mac OS X (GraphPad Software, San Diego, CA, USA).
Results
A total of 10 patients with traumatic blunt celiac artery injuries met the inclusion criteria for this study. The vast majority of patients were male (7/10, 70%) with an average age of 38.3 ± 16.1 years. Overall mortality for this study group was found to be 20% (2/10). The most common mechanisms of injury were motor vehicle crashes (8/10, 80%) followed by motorcycle crashes (2/10, 20%). Patients spent on average 10.2 ± 6.5 total days in the hospital, 4.4 ± 4.5 days in the intensive care unit, and 1.6 ± 2.8 days on the ventilator. Notably, this cohort of patients appeared to be relatively hemodynamically stable upon arrival with an average initial heart rate of 94 ± 33.3 beats per minute and an average initial systolic blood pressure of 118 ± 23 mmHg. The average injury severity score for the cohort was found to be 27.5 ± 14.1 and the average total number of injuries for the cohort was 5.1 ± 2.7 (Table 1).
Demographic Data for the Entire Cohort.
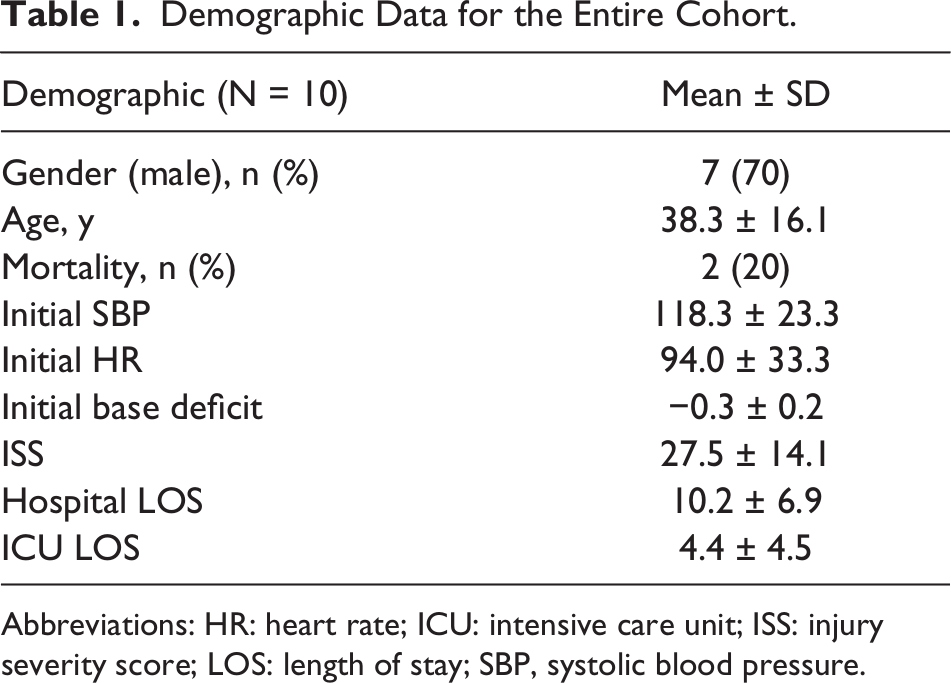
Abbreviations: HR: heart rate; ICU: intensive care unit; ISS: injury severity score; LOS: length of stay; SBP, systolic blood pressure.
The majority of patients presented with either an intimal dissection (3/10, 30%) (Figure 1) or an intraluminal thrombus (3/10, 30%) (Figure 2). Other injuries seen included pseudoaneurysms (2/10, 20%) (Figure 3), an avulsion injury (1/10, 10%), and a dissection with an intraluminal thrombus (1/10, 10%). One patient with a diagnosed pseudoaneurysm had follow-up imaging. Only 2 patients out of the cohort (20%) were noted to have retrograde flow on imaging studies. Of these 2 patients, 1 underwent a computed tomography angiography study which noted retrograde flow primarily through the gastroduodenal artery, while the other patient underwent a visceral angiogram which noted retrograde filling of the gastroduodenal, hepatic, and splenic arteries.

Computed tomography scan demonstrating focal dissection of the celiac artery.

Computed tomography scan showing intraluminal thrombus of the celiac artery.

Computed tomography scan demonstrating pseudoaneurysm of the celiac artery.
When examining how these patients were managed, the vast majority were managed nonoperatively (8/10, 80%). Of the 2 patients managed surgically, 1 patient underwent endovascular stenting of the celiac artery on hospital day one. This patient was also found to have a concomitant traumatic aortic dissection that required endovascular stent placement. The second patient underwent open ligation via an exploratory laparotomy shortly after the presentation to the trauma bay (Table 2). In regard to medical management that was utilized, 1 patient (10%) was started on a heparin drip during their admission and was transitioned to aspirin at the time of discharge. Four additional patients (40%) were also discharged home on aspirin therapy.
Patient Presentation, Management, and Outcomes.
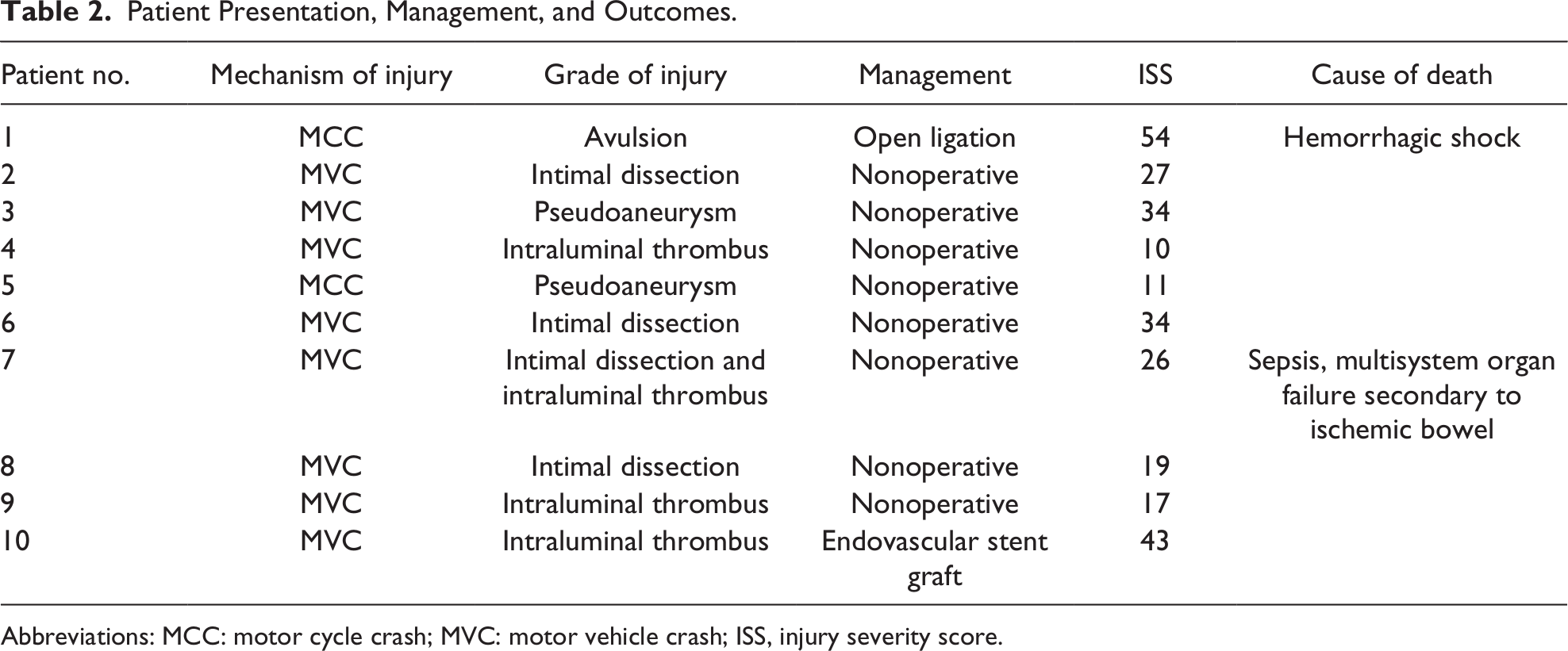
Abbreviations: MCC: motor cycle crash; MVC: motor vehicle crash; ISS, injury severity score.
In regard to the 2 mortalities in this cohort, 1 patient presented to the trauma bay after a motor vehicle crash. He was found to be hypotensive with a negative focused assessment with sonography for trauma study. He continued to be hypotensive after chest tube placement, and thus, a diagnostic peritoneal lavage was performed in the trauma bay which was nondiagnostic secondary to intra-abdominal adhesions. He then underwent a pericardial window which was also negative. Following this procedure, he was taken for imaging which noted a celiac artery dissection with an associated thrombus. His hemodynamic status improved after a blood transfusion and he was, thus, admitted to the intensive care unit. On the morning of hospital day 1, he was noted to become peritonitic on abdominal examination with rising lactate. Given these findings, he was taken emergently to the operating room where he was found to have an ischemic transverse colon and a splenic laceration. Simultaneously, a transesophageal echocardiogram demonstrated an ejection fraction of 10% with a left atrial thrombus raising the concern for a low flow state. He underwent an extended right hemicolectomy and splenectomy and was left in discontinuity with a planned second look. On hospital day 2, he was taken back to the operating room where he was noted to have necrotic stomach, liver, and patchy ischemia of the small bowel. As these findings were thought to be incompatible with survival, the patient’s family elected to proceed with comfort care measures.
The second mortality presented after a motorcycle crash. He lost pulse in the trauma bay, and an emergent thoracotomy was performed. Shortly thereafter, he was taken to the operating room where he underwent an exploratory laparotomy. Upon exploration, he was noted to have avulsion of the celiac and superior mesenteric arteries (SMAs) in addition to an aortic injury, an avulsion of the left kidney, and an avulsion of the pancreas. Given the significant blood loss, the patient progressed to asystole and was unable to be resuscitated.
Discussion
Traumatic celiac artery injuries are rare, and when present, are most often secondary to a penetrating mechanism of trauma. 8 When focusing on blunt celiac artery injuries, in particular, there are only 11 cases reported in the literature. 6,8 The most common mechanism of injury described was motor vehicle crashes followed by falls from height and crush injuries. Injury patterns also varied and included 4 disruptions (3 complete and 1 partial), 4 dissections, 1 pseudoaneurysm, and 1 intimal flap. Of the cases described, a total of 4 patients underwent open surgery. Within these cases, 3 patients underwent an open ligation and 1 patient underwent an attempted bypass. This case was complicated by an intraoperative death that was likely secondary to a concomitant SMA disruption. 6 Of the patients managed nonoperatively, 2 patients underwent endovascular stent placement, 2 patients were managed with therapeutic anticoagulation, and 1 patient was managed with aspirin. One patient in the literature was noted to have a delayed presentation of a dissection and eventually died later in their hospital course from fulminant liver failure. 6
When discussing management options, nonoperative management with therapeutic anticoagulation or antiplatelet agents has been described for isolated dissections. Endovascular intervention in the form of stenting has also been shown to be a viable option, even in the setting of more significant injuries. 9,10 Open surgical ligation has typically been reserved for injuries with associated hemorrhagic shock in the setting of damage control surgery. 6 If this is performed, one must confirm collateral arterial flow to the common hepatic artery to avoid the risk of liver failure.
In this case series, which represents the largest single-institution study in the literature, the majority of patients were successfully managed nonoperatively. This data suggest that intervention can be reserved for those patients who are hemodynamically unstable at the time of initial presentation or for those patients who fail medical management with anticoagulation. Patients who present in extremis with intra-abdominal hemorrhage will typically undergo laparotomy with ligation of the celiac axis and to treat any concomitant abdominal injuries. This treatment strategy relies on collateral flow through the gastroduodenal artery to the retrograde filling of the common and proper hepatic arteries to decrease the risk of liver failure. Concomitant SMA injury will require emergent revascularization of the SMA with ligation of the celiac artery as an option. With the advent of endovascular therapies, flow-limiting dissections or pseudoaneurysms not involving the origin of the celiac artery may be treated utilizing a covered stent graft. Although there are multiple treatment options available, there is currently no consensus or protocols in regard to strict management guidelines. Due to the low frequency of celiac artery injuries, a multicenter consortium is necessary to develop a grading system and treatment recommendations for this rare injury.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.