
Abstract
Introduction
Incisional hernias (IH) are iatrogenically created in 400 000 new patients annually. Without repair, IH-associated complications can result in major illness and death. The health disparities literature suggests that under-represented patients present more frequently with surgical emergencies. The health disparities associated with IH remain relatively unstudied.
Methods
Inpatient admission data were obtained from the Healthcare Cost and Utilization Project National Inpatient Sample for 2012-2014. Patients with IH International Classification of Diseases ninth revision were included. Analyses were completed using survey specific procedures (SAS v.9.4). Type of admission within groups was compared via Rao-Scott chi-square tests. The probability of an elective admission was modeled via SurveyLogistic Procedure.
Results
Of 39 296 cases, 38.5% IH admissions were urgent or emergent (nonelective). The proportion of nonelective admission was statistically higher (P < .0001) in patients >65 (40.9%) and females (40.3%). Among insurance types, self-paying patients had the highest proportion of nonelective admissions (64.3%). Racial disparities remained significant after adjusting for age, sex, and insurance. Compared with white patients, the odds of an admission being nonelective were significantly higher for black (odds ratio [OR] [95% CI]: 1.65 [1.53-1.77]], Hispanic (OR [95% CI]: 1.39 [1.28-1.51]), and other (OR [95% CI]: 1.2 [1.06-1.37]) patients.
Discussion
These data show that multiple at-risk patient populations are significantly more likely to require urgent admission for IH-related complications. These include older, female, non-white, and uninsured patients. Systematic efforts to ameliorate these disparities should be developed.
Introduction
Incisional hernia (IH) is a major and common surgical complication, with an incidence of 10%–25% following laparotomy. In the United States, approximately 400 000 IH repairs are performed annually at an estimated recurring cost of $6.3 billion per year. 1 -3 Without repair, IH patients risk developing life-threatening conditions including small bowel obstruction, and intestinal strangulation, and necrosis.
IH repairs may be performed electively or urgently. In general, emergent surgical procedures have worse outcomes. For IH, the patient-level and hospital-level factors that drive elective versus emergent repairs are unstudied. Previous studies of ventral hernias, a diagnosis inclusive of but not restricted to IH, have reported that socioeconomic status (SES), race/ethnicity, age, and comorbidities were independent predictors of emergent ventral hernia repair. 4,5 We therefore hypothesize that SES, race/ethnicity, age, and gender are significant risk factors for emergent IH repair. To test this hypothesis, we analyzed the 2012-2014 Healthcare Cost and Utilization Project National Inpatient Sample (HCUP-NIS).
Methods
Data on inpatient admissions related to IH were obtained from the HCUP-NIS for the years 2012-2014. Inpatient admissions with a principal diagnosis of IH were identified using International Classification of Diseases (ICD-9) codes 551.21, 552.21, and 553.21. Cases with non-IH principal diagnoses were excluded to ensure that the IH was the reason for hospitalization.
The outcomes for the clinical presentation of IH include the type of admission, which is our primary outcome, along with complicated diagnosis and the use of emergency department services. Type of admission is routinely recorded in the HCUP-NIS database. Complicated diagnosis was defined as the primary ICD-9 diagnosis code for IH with gangrene (551.21) or obstruction (552.21). The use of emergency department services is defined in the HCUP NIS using revenue codes, emergency department charges, CPT codes, and condition codes.
The overall frequency and cost of inpatient admissions related to primary IH was reported for the timeframe as the weighted sample sum and mean. Outcomes were analyzed using logistic regression and P values are from chi-squared tests. Adjusted models included patient age, race, sex, and insurance status. Analyses included only records with complete data and were performed using SURVEY procedures in SAS version 9.4 to account for the HCUP NIS survey design. A P value of 0.05 was used to establish statistical significance and report CIs.
Results
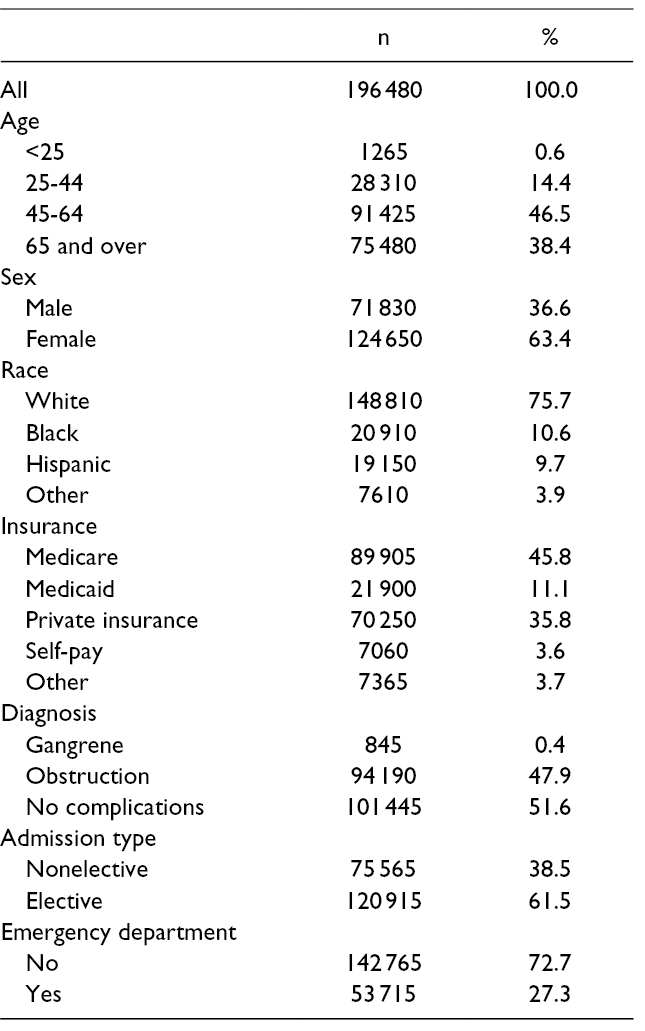
The average annual estimate of inpatient visits with a primary diagnosis of IH was 69 677, incurring an average annual cost of 3.8 billion dollars. In total, 39 296 cases met study eligibility requirements for our analysis of the clinical presentation. Characteristics of the study population are reported in Table 1. The population was majority female (63.4%) and majority white (75.7%). Medicare (45.8%), private insurance (35.8%), and Medicaid (11.1%) were the leading forms of insurance. Regarding patient presentation, the majority of admissions with a primary diagnosis of IH (61.5%) were elective admissions. Most of the admissions did not have an additional complication of gangrene or bowel obstruction (51.6%) and did not use the emergency department (72.7%).
Study Population Characteristics.
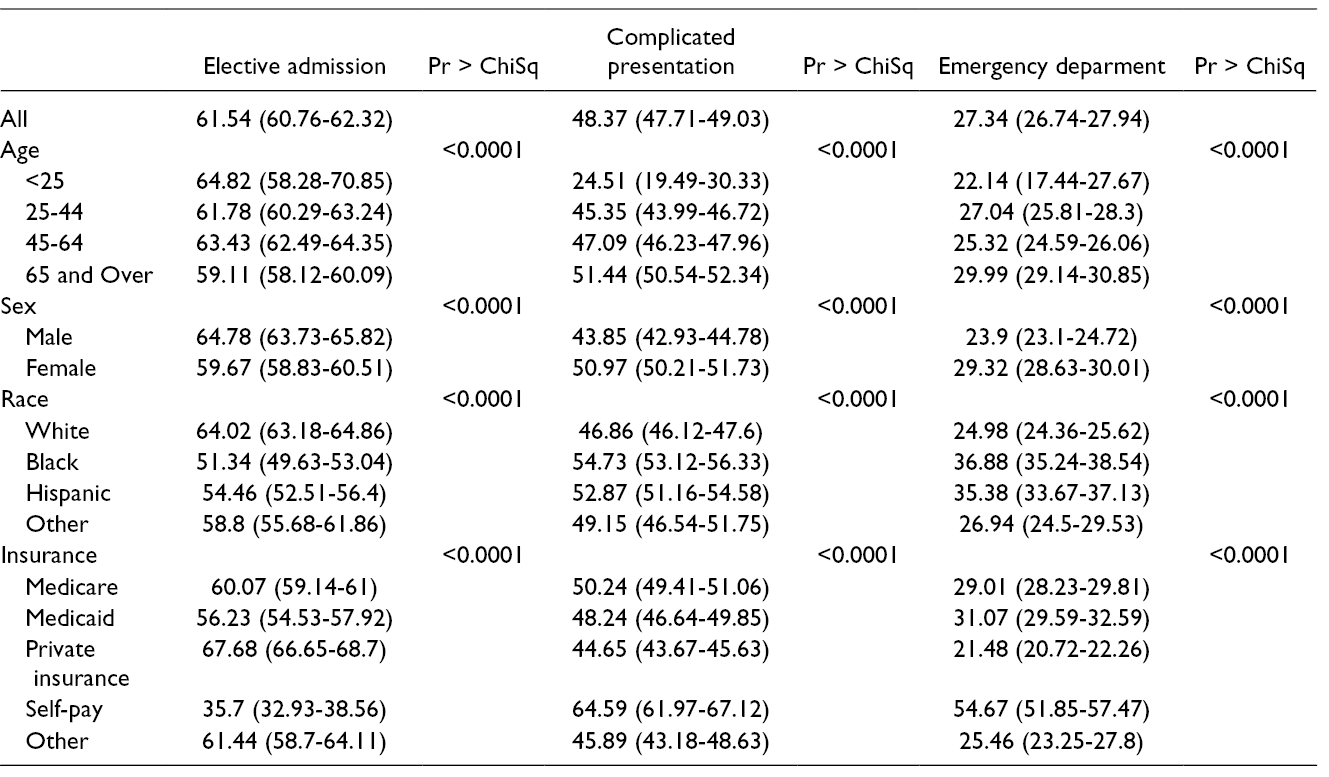
We first performed univariate comparisons between patient characteristics and the clinical presentation of IH (Table 2). The proportion of nonelective admissions varied significantly by age, sex, race, and insurance status, where the highest share of nonelective admissions was seen in patients over the age of 65, females, nonwhites, and self-payers. Similarly, there were significant associations between age, sex, race, and insurance with IH-related complications and the use of emergency department.
Incisional Hernia Presentation by Age, Sex, Race/Ethnicity, and Insurance Status.
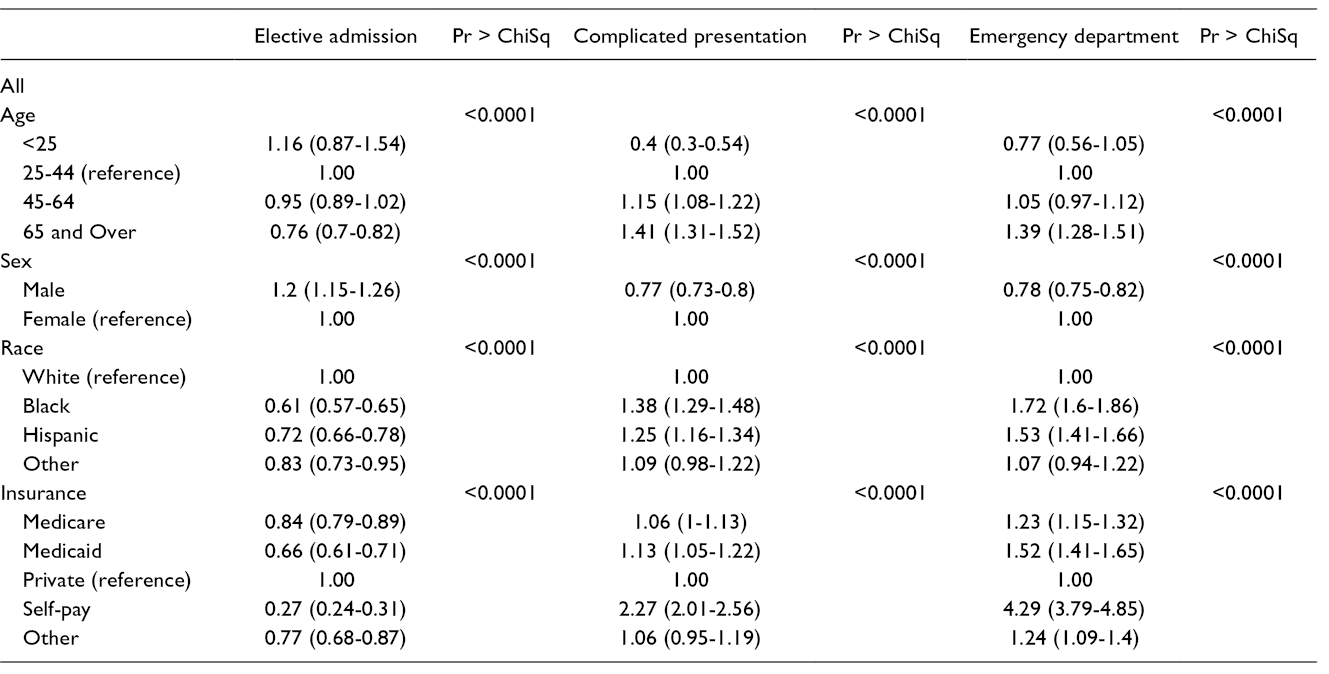
Next, we developed adjusted odds ratios (OR) using multivariable logistic regression models (Table 3). Females were more likely to present for emergent admission (OR [95% CI]: 0.83 [0.8-0.87]). The odds of an admission being emergent were higher for black (OR [95% CI]: 1.65 [1.53-1.77]), Hispanic (OR [95% CI]: 1.39 [1.28-1.51]), and other (OR [95% CI]: 1.2 [1.06-1.37]) when compared with non-Hispanic white patients. The greatest disparity was seen among insurance status, where self-pay patients were most likely to present nonelectively compared with private insurance patients (OR [95% CI]: 3.68 [3.23-4.19]).
Adjusted Odds Ratios From Multivariable Logistic Regression Models.
Discussion
IH is a common surgical problem with approximately 100 000-400 000 cases repaired annually; although many more per year go unrepaired as watchful waiting is an appropriate response to an asymptomatic IH. 1 -3 While many IH patients remain asymptomatic, patients with IH complications such as small bowel obstruction or ischemia secondary to incarcerated or strangulated bowel have worse morbidity and mortality. 6 Early herniorrhaphy would mitigate those risks, but such early intervention requires ease of access to healthcare. Watchful waiting is meant to be a medical decision, rather than an omission of decision.
This study demonstrates that at-risk patient populations with IH were significantly more likely to present for emergent inpatient admission. The at-risk populations included patients over the age of 65, females, nonwhites, and self-payers. The significant racial disparities persisted after controlling for age, sex, and insurance status: racial and ethnic minorities were more likely to have an emergent admission than non-Hispanic whites. Overall, several socially disadvantaged population groups were found to have higher rates of urgent and emergent admissions, indicating that they may not be seeking treatment at all, or delaying treatment and presenting later in the IH disease course. This pattern is concerning because emergent admissions are more expensive and generally riskier than elective admissions and repairs.
Later presentation also carries a heftier financial burden for the patient and the health care system. 7 If social determinants of health affect the presentation type of IH patients, we can expect to see unequal proportions of emergent presentation in at-risk groups. Discrepancies in access and understanding are such social determinants of health and often correlate with membership in minority groups including under-represented racial minorities, advanced age, female sex, and low socioeconomic status.
Patient factors such as transportation, literacy, and health literacy are a potential source for disparities. Similarly, provider factors such as implicit bias, lack of cultural awareness, and technical skill of regionally available surgeons may have an impact. The system factors such as clinic placement and hours of operation are harder to address, but the first 2 domains can and should be actively addressed. Efforts should be made on behalf of the providers to engage at-risk populations; possibly including additional education at the time of laparotomy about the risk of IH and what to look for. Additional follow-up appointments for at-risk patients may ease this disparity as well. Of course, surgeons should always strive for better outcomes and great care should be taken in technique to prevent IH from occurring in the first place.
The limitations of this study stem primarily from inconsistencies with medical coding. We found less than 70 000 cases with a principal diagnosis of IH, yet repairs were coded closer to 100 000 times. Further, this type of study does not allow us to identify which of the social determinants of health are at play in our sample. As this is national data, more regional studies are needed to characterize geographic differences of surgical health disparities and form a relevant plan of action to reduce IH incidence and increase early access to care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.