
Abstract

Obesity is a worldwide epidemic affecting all age groups, ethnicities, and both genders. Bariatric surgery provides an effective sustained weight loss option to those who qualify and improves associated metabolic co-morbidities, functionality, and quality of patients’ lives as well as their psychosocial health. Given the rise of bariatric surgeries performed over the last decade and the potential high risk of morbidity and mortality if done poorly, the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery have established criteria for accreditation as a Center of Excellence with best practices for obesity care for providers and hospitals. These criteria address the structural adjustments, allied health staffing, and training that are necessary for a facility to properly accommodate bariatric surgical patients, as well as evaluate outcome-based standards. 1
The purpose of our study was to examine early complications among bariatric surgery patients undergoing laparoscopic vertical sleeve gastrectomy (LVSG) at a single rural bariatric center. Our aim was to assess safety in a community setting.
We completed a retrospective review of bariatric procedure performed by a single surgeon at a rural community hospital from 2014 to 2017. The primary procedure in each case was an LVSG. An LVSG performed as a conversion procedure after gastric band removal (GBR) was included in this patient population; 24.5% of patients also underwent hiatal hernia (HHR) at the time of their LVSG. Outcomes of interest were complications requiring medical management, hospitalization, operative intervention, and mortality. Patient follow-up was 2 weeks and 6 weeks for the time frame of this study.
One thousand patients (700 LVS, 245 LVSG + HHR, 55 LVSG + GBR) were analyzed, of which 839 (84%) were female. The mean age of the group was 44, with a mean BMI of 45. Patient comorbidities included 207 (20.7%) with diabetes, 525 (52.5%) with obstructive sleep apnea, 479 (47.9%) with gastroesophageal reflux, 535 (53.5%) with hypertension, and 251 (25.1%) with hyperlipidemia. Ten (1%) patients required readmission (within 30 days of the index operation) for complications that did not require procedural or surgical intervention. Only 3 admissions were related to the bariatric procedure: 2 (0.2%) for mesenteric vein thrombosis, at 10 days postop and 20 days postop, respectively, and 1 (0.1%) leak at 25 days postop. Four (0.4%) patients required re-operation for complications (3 resulted in no findings and 1 postop bleed). There were no deaths. (Table 1)
Demographics, Co-morbidities, and Complications. a
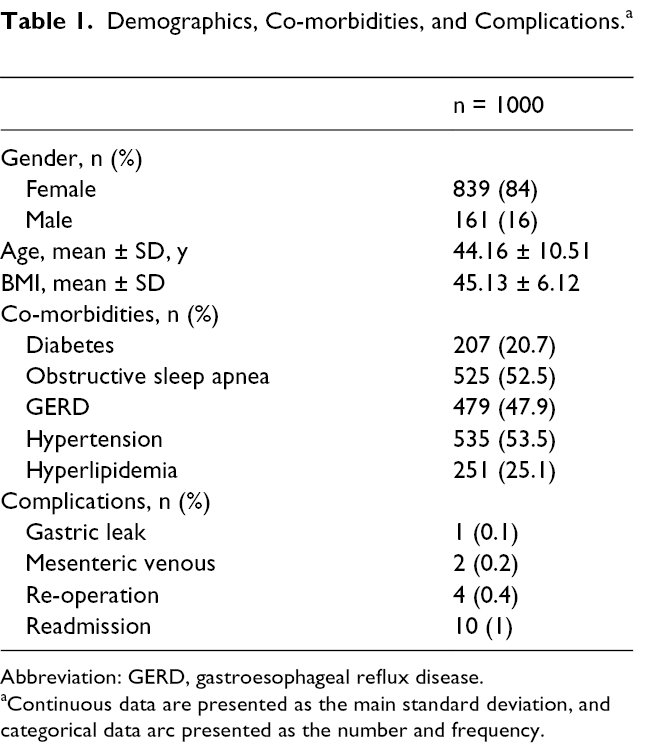
Abbreviation: GERD, gastroesophageal reflux disease.
aContinuous data are presented as the main standard deviation, and categorical data arc presented as the number and frequency.
Accepted overall morbidity and mortality rates after an LVSG range from 0% to 17.5% and from 0% to 1.2%, respectively. 2 The main surgical complications after an LVSG include bleeding, leaks, and portal vein thrombosis. Postoperative bleeding complications range from 0.6% to 1.9%. Our postoperative reintervention rate was only 0.4% with only 0.1% case having an identifiable bleeding cause. Sources of bleeds include the lumen of the stomach, intra-abdominally, or from trocar sites. If bleeding does occur, there are associated higher rates of re-operations, readmissions, and even mortality. Factors that can increase bleeding risk include older age, higher number and degree of comorbid conditions, and operative length. A higher BMI has actually been shown to be protective. Techniques to reduce the risk of bleed include staple line reinforcement and good surgical exposure of the left upper quadrant to prevent intra-abdominal bleeding by splenic tears. 3 The reported rates for leak range from 0% to 5.5%. Our leak rate was 0.1%. The LVSG has been shown to have higher leak rates than Roux-en-Y gastric bypasses despite no anastomosis due to increase intraluminal gastric pressure from the long and narrow staple line. Additionally, leaks after LVSGs are harder to close due this increase intraluminal pressure. Their etiology include ischemia, hematoma formation, and staple misfires. Leaks are managed based on patient stability and time of presentation. Treatment options include immediate re-operation, endoluminal stenting, sleeve revision, or conversion to Roux-en-Y gastric bypass. Porto-mesenteric vein thrombosis is an uncommon complication occurring in less than 1% of patients. 4 In our retrospective review, we found our rate was 0.2%. Patients will present with epigastric abdominal pain and are diagnosed by computed tomography. In stable patients with nonocclusive thrombi, they can be given the standard anticoagulation regimen for a provoked venous thrombus. If the thrombus is occlusive, operative intervention may be required. If an acute occlusive thrombus is present in the portal system, the patient can present with acute pylephlebitis with the presence of fevers, chills, and painful liver. If in the superior mesenteric vein, they may have colicky abdominal pain and associated diarrhea. If the thrombus is present in proximal mesenteric arches, bowel ischemia can develop requiring operative intervention and subsequent anticoagulation treatment.
Complication rates after laparoscopic sleeve gastrectomy continue to decline with improvements in technique. Our rates are comparable and below the reported national standards. Our study shows, in a certified comprehensive bariatric program with a multidisciplinary approach, LVSG can be performed safely in a community hospital setting with low mortality and morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.