
Abstract
Introduction
Preinjury alcohol use and older age have independently been associated with poor outcomes. This study examined whether higher levels of blood alcohol concentration (BAC) correlated with an increased likelihood of poor outcomes in older trauma patients.
Methods
This was a retrospective cohort study of injured patients ≥65 years with BAC testing presenting to a Level 1 trauma center between 2015 and 2018. Patients were stratified by BAC at 4 thresholds of intoxication: BAC ≧10 mg/dL, BAC ≧80 mg/dL, BAC ≧150 mg/dL, and BAC ≧200 mg/dL. Propensity score matching using inverse probability of treatment weighting was used to estimate outcomes. Logistic and Poisson regression models were performed for each threshold of the BAC level with the matched cohort to assess clinical outcomes.
Results
Of all older patients (n = 3112), 32.5% (n = 1012) had BAC testing. In the matched cohort of 883 patients (76.7 ± 8.2 years; 48.1% female), 111 (12.5%) had BAC ≧10 mg/dL, 83 (74.8%) had BAC ≧80 mg/dL, 60 (54.1%) had BAC ≧150 mg/dL, and 37 (33.3%) had BAC ≧200 mg/dL. Falls (60.5%) and motor vehicle crashes (28.9%) were the most common mechanisms of injury. Median (IQR) of Injury Severity Score (ISS) was 5 (1-10). The risk of severe injury (ISS ≧15) was similar between alcohol-positive and alcohol-negative patients (9.9% vs 15.0%, P = .151). BAC ≧10 g/dL was not associated with length of stay, intensive care unit admission, or in-hospital complication, nor was any of the other 3 analyzed BAC thresholds.
Conclusion
Overall, any detectable BAC along and increasing thresholds of BAC was not associated with poor in-hospital outcomes of older patients after trauma. Alcohol screening was low in this population, and intoxication may bias injury assessment, leading to mistriage of older trauma patients.
Introduction
Preinjury substance use has been associated with increased morbidity and mortality after traumatic injury. 1 -3 Despite this, substance use disorders among older trauma patients have been largely understudied, unrecognized, and undertreated. 4,5 Due to alterations in cognition and judgment, patients under the influence of nonprescribed drugs or alcohol present with unique physiology and injury patterns. 6,7 The impact of substance use disorders has garnered the attention of the American College of Surgeons, who mandated in 2006 that trauma centers must perform brief interventions for alcohol use for patients positive for alcohol on admission. 8
Substance use disorder has largely been thought of as a disease affecting younger patients. Thus, even though alcohol and drugs may significantly affect outcomes for older trauma, many of these patients are not screened. An Illinois study examining the statewide incidence of substance use revealed that only 5% of older patients (age ≥65) were tested for the presence of alcohol, but of those tested for blood alcohol concentration (BAC), 49.7% tested positive and 71.8% were considered intoxicated. 4 Because older patients frequently have other multiple comorbidities, alcohol intoxication on admission results in increased readmission rates, twice the incidence of falls, and high rates of injury-related mortality. 4,9 Older trauma patients consume one-third of all trauma-related health care expense, with alcohol intoxication further raising these costs. 10
Preinjury alcohol use and older age have both been independently associated with poor outcomes after trauma. 5,11 -13 Due to the limited physiologic reserve of older patients, small amounts of alcohol may result in significant impairment. 14 The purpose of this study is to determine if a dose-dependent relationship existed between increasing levels of BAC and poor clinical outcomes in an older trauma population.
Methods
Study Design and Materials
This retrospective observational cohort study of older adult trauma patients at a single Level 1 trauma center in North Carolina included patients admitted between February 2015 and February 2018. Trauma registry data and electronic medical records of eligible participants were reviewed. The hospital institutional review board approved the study.
Included patients were ≥65 years and had a documented serum blood alcohol concentration within 1 hour of hospital arrival. Transferred patients were only included if a serum BAC obtained within 1 hour of arrival to the outside hospital was available in the records. Within the cohort with a documented 1-hour serum BAC, there were no exclusionary criteria.
Data Collection and Definitions
Based on BAC testing on arrival, patients were stratified into ordinal groups based on detectable (≧10 mg/dL) versus undetectable BAC (<10 mg/dL), BAC ≧80 mg/dL versus <80 mg/dL, BAC ≧150 mg/dL versus <150 mg/dL, BAC ≧200 mg/dL versus <200 mg/dL. A threshold of 10 mg/dL is the laboratory threshold for detectable BAC. The threshold of 80 mg/dL was chosen as this is the legal limit of BAC. The thresholds of 150 mg/dL and 200 mg/dL represent approximately the 50th and 75th percentiles of the BAC distribution.
Remaining clinical data were retrospectively extracted using the institutional trauma registry and electronic medical record. This included demographic information (gender, age at injury), as well as comorbid conditions listed at the time of injury, mechanism of injury, injury severity score (ISS), scene vitals, emergency department vitals, hospital discharge disposition, hospital and intensive care unit (ICU) length of stay, level of trauma activation (trauma one, trauma alert, no activation), insurance provider, and mortality. The primary outcomes were hospital length of stay, any in-hospital complication, inferior disposition, and mortality. Secondary outcomes like the number of in-hospital complications, ICU admission, ICU length of stay were also examined. Inferior disposition included discharge to hospice, skilled nursing facility, long-term care hospital, or mental health facility. In-hospital complications include arrhythmia, pneumonia, alcohol withdrawal, urinary tract infection, unplanned ICU admission, unplanned intubation, malnutrition requiring enteral or parental nutrition, respiratory failure, mortality, cardiac arrest, and stroke.
Statistical Analysis
Comparison of outcomes was estimated using propensity score matching with an inverse probability weighting model to reduce bias between the cohorts. Four different levels of intoxication were evaluated based on minimal BAC for laboratory detection, legal limit of BAC, and quartiles of BAC distribution: BAC ≧10 mg/dL versus <10 mg/dL, BAC ≧80 mg/dL versus <80 mg/dL, BAC ≧150 mg/dL versus <150 mg/dL, BAC ≧200 mg/dL versus <200 mg/dL. Each model examining the primary and secondary outcomes was adjusted for gender, age, ISS, comorbidities (hypertension, diabetes, coronary artery disease, congestive heart failure, mental health condition, chronic obstructive pulmonary disease, tobacco use, chronic kidney disease, stroke), insurance type, mechanism of injury, and anticoagulant use.
Bivariate analysis of demographic and clinical variables was conducted with the matched patients. Chi-square and Wilcoxon rank-sum tests were performed, where appropriate. Logistic and Poisson regression models were utilized to examine each primary and secondary outcome with the matched cohort. Average treatment effect, or the average effect of a binary independent variable on an outcome, and the odds ratios for each outcome were estimated. While crude mortality rates were compared between cohorts, mortality could not be evaluated in the propensity-matched cohorts due to the effect of the inverse probability weighting model leading to a violation of the treatment overlap assumption for that outcome. For all analyses, a P value ≤.05 was considered statistically significant. Analyses were performed using Stata (StataCorp LLC, StataCorp 15.1, College Station, TX, USA).
Results
During the study period, a total of 3112 older adult trauma patients were included in the trauma registry, with 1012 (32.5%) of these patients having BAC testing within 1 hour of hospital arrival. Of those with complete BAC testing, 883 (87.3%) were matched based on inverse probability weighting to comprise the final study population. Included trauma patients were on average 76.7 (SD 8.2) years of age, and 48.1% (n = 425) were female. Alcohol-positive patients composed 12.6% of the cohort (n = 111). The distribution of BAC is depicted in Figure 1. Of alcohol-positive patients, median BAC was 152 mg/dL (IQR 79-229 mg/dL) with 83 patients (74.8%) having a BAC of ≧80 mg/dL, 60 (54.1%) having a BAC of ≧150 mg/dL, and 37 (33.3%) having a BAC of ≧200 mg/dL.
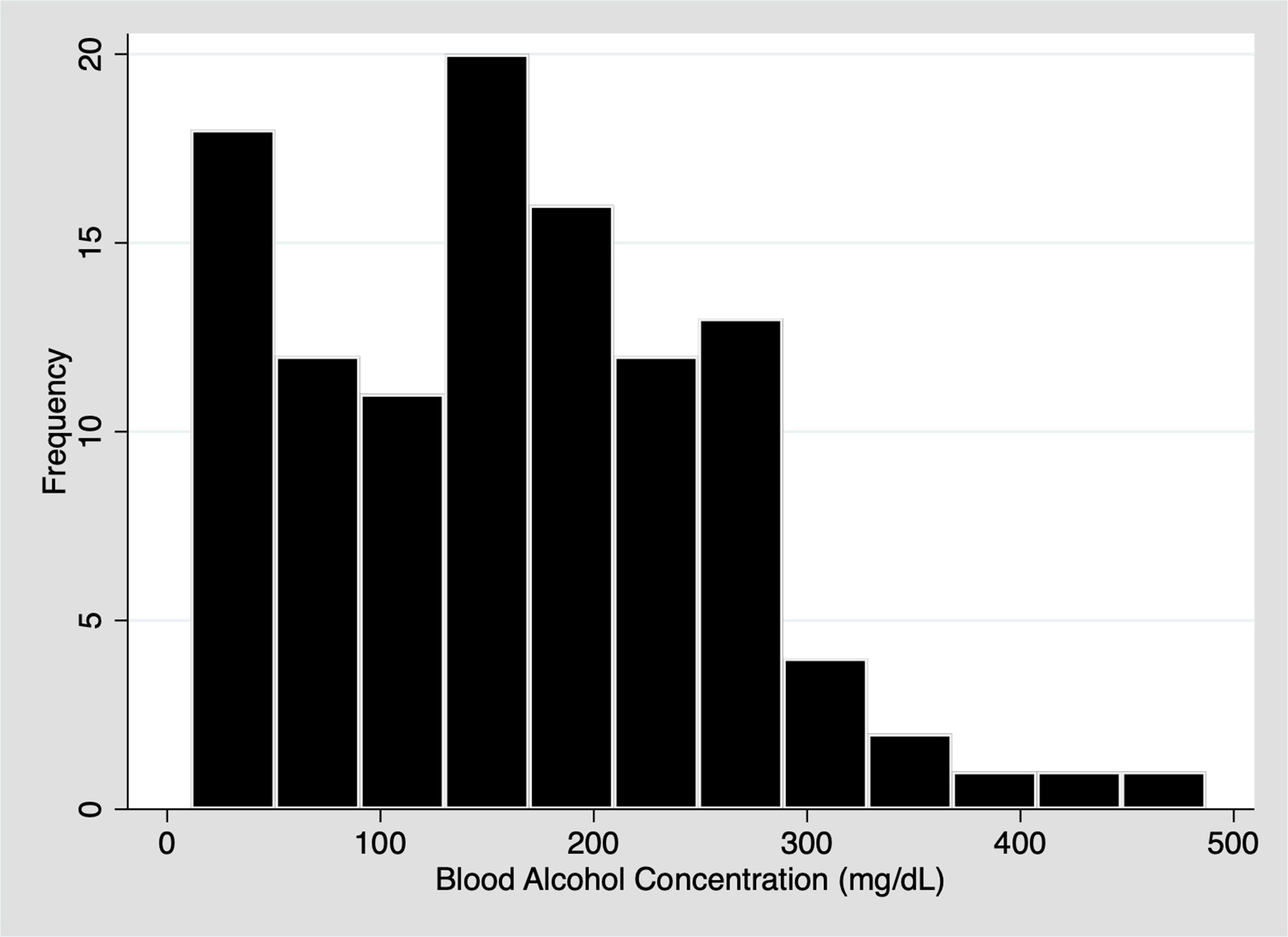
Histogram of initial blood alcohol concentration after injury in a matched cohort of older adult patients (n = 883).
The characteristics associated with alcohol consumption in the matched cohort of BAC-tested older patients included younger age (median 70 years [IQR 67-78] vs 77 years [IQR 70-84]) and male gender (69.4%, n = 77 vs 49.3%, n = 381, P < .001). The following comorbidities were more common in alcohol-positive patients: coronary artery disease/congestive heart failure (34.2% vs 16.2%, P < .001), cardiac arrhythmias (26.1% vs 13.7%, P = .002), stroke (12.6% vs 4.7%, P = .003), alcohol use disorder (81.0% vs 7.8%, P < .001), and tobacco use (48.8% vs 8.0%, P < .001). Of those with a BAC ≧200 mg/dL, 62.2% (n = 23) had a documented alcohol use disorder, compared with 31.6% (n = 24) with an alcohol use disorder in the cohort with a BAC <200 mg/dL. The primary insurance provider for both alcohol-negative and alcohol-positive patients was Medicaid or Medicare, providing coverage (74%, n = 571 vs 79.3%, n = 88) to each cohort, respectively.
Alcohol-positive patients had the highest proportion of nontrauma activations (26.1%, n = 29 vs 12.8%, n = 99, P < .001) and were more likely to be a transfer from an outside hospital (17.1%, n = 19 vs 12.6%, n = 97, P = .18). A higher percentage of falls (64.0% vs 60.0%), assaults (4.5% vs 0.7%), pedestrian-involved motor vehicle crashes (MVC; 4.5% vs 2.8%), and gunshot wounds (2.7% vs 0%) was seen in the alcohol-positive cohort (P < .001). Alcohol-negative patients had a higher frequency of MVC/motorcycle crash (31.6% vs 24.3%, P < .001). However, median ISS did not statistically differ between alcohol-positive and alcohol-negative patients when considering individual mechanisms of injury. Scene vital signs were not statistically different between alcohol-negative and alcohol-positive patients with the exception of scene systolic blood pressures, which were significantly lower in the alcohol-positive cohort (135 mm Hg [SD 31] vs 152 mm Hg [SD 33], P < .001). Alcohol-positive patients had a higher likelihood of presenting during the night shift, between 7:00 PM and 7:00 AM (66.7% in alcohol positive vs 28.1% in alcohol negative, P < .001). Overall, falls (60.5%) and MVCs (28.9%) were the most common mechanism of injury with a median (IQR) ISS of 5 (1-10). Median ISS did not significantly differ between alcohol-positive patients (6 [IQR 2-10]) vs (5 [IQR 1-10]) and alcohol-negative patients (P = .775). While fewer alcohol-positive patients were severely injured (ISS ≧15) versus alcohol-negative patients (9.9% vs 15.0%, P = .151), this difference was not statistically significant.
The proportion of deaths in the alcohol-positive group (2.7%, n = 3) was lower than the alcohol-negative group (6.7%, n = 53), but not statistically different (P = .092). Median hospital length of stay did not differ between cohorts (4 days [IQR 1-8 days] for both cohorts, P = .630), and admission rates were similar (70.3% in alcohol positive versus 71.6% in alcohol negative, P = .766). Bivariate analyses of clinical outcomes are reported in Table 1.
Bivariate Analysis of Clinical Outcomes of Positive BAC a Versus Negative BAC Older Adult Trauma Patients.
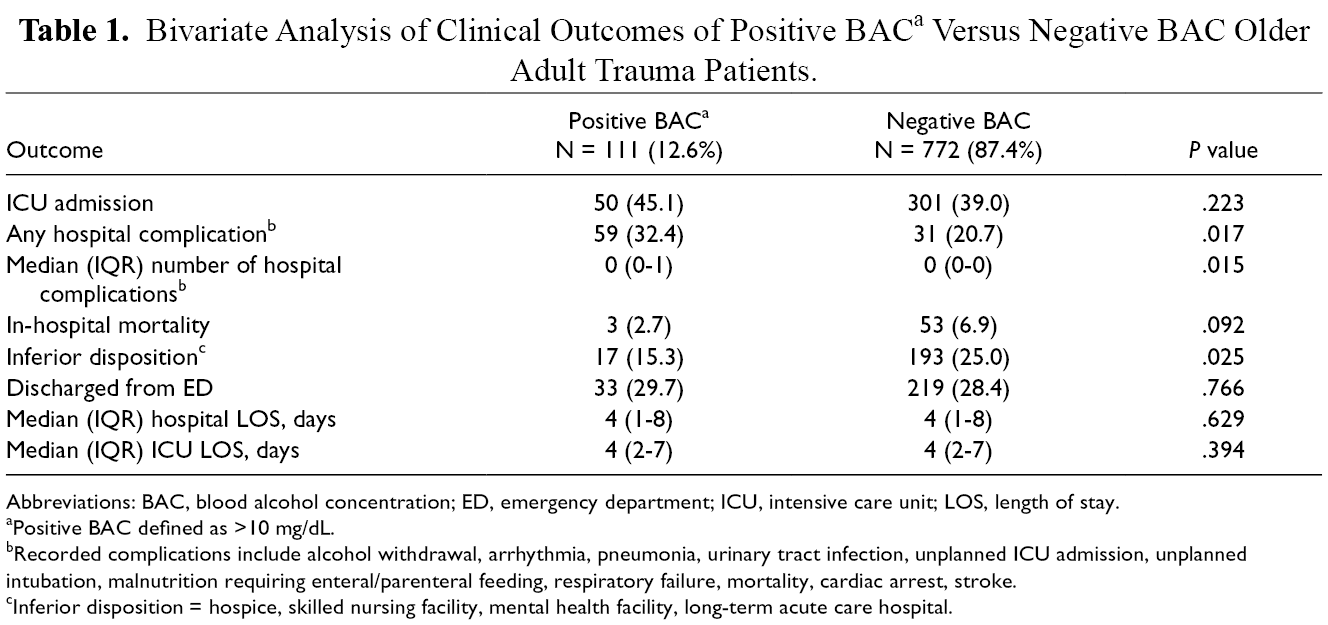
Abbreviations: BAC, blood alcohol concentration; ED, emergency department; ICU, intensive care unit; LOS, length of stay.
aPositive BAC defined as >10 mg/dL.
bRecorded complications include alcohol withdrawal, arrhythmia, pneumonia, urinary tract infection, unplanned ICU admission, unplanned intubation, malnutrition requiring enteral/parenteral feeding, respiratory failure, mortality, cardiac arrest, stroke.
cInferior disposition = hospice, skilled nursing facility, mental health facility, long-term acute care hospital.
In the propensity-matched analysis, positive BAC was not associated with length of hospital stay, ICU admission, length of ICU stay, or suffering a complication, for any of the increasing BAC thresholds (Table 2). The BAC-positive cohort had a lower odds of inferior disposition versus the undetectable BAC cohort (OR 0.52, P = .04) versus the BAC ≤80 (OR 0.43, P = 0.03) cohort. As noted in the Methods section, the outcome of mortality could not be assessed using inverse probability weighting as the model violated the treatment overlap assumption.
Using Inverse Probability Weighting, the Clinical Outcomes of Matched BAC-Positive Patients Versus BAC-Negative Patients Were Compared with Increasing Thresholds of BAC.
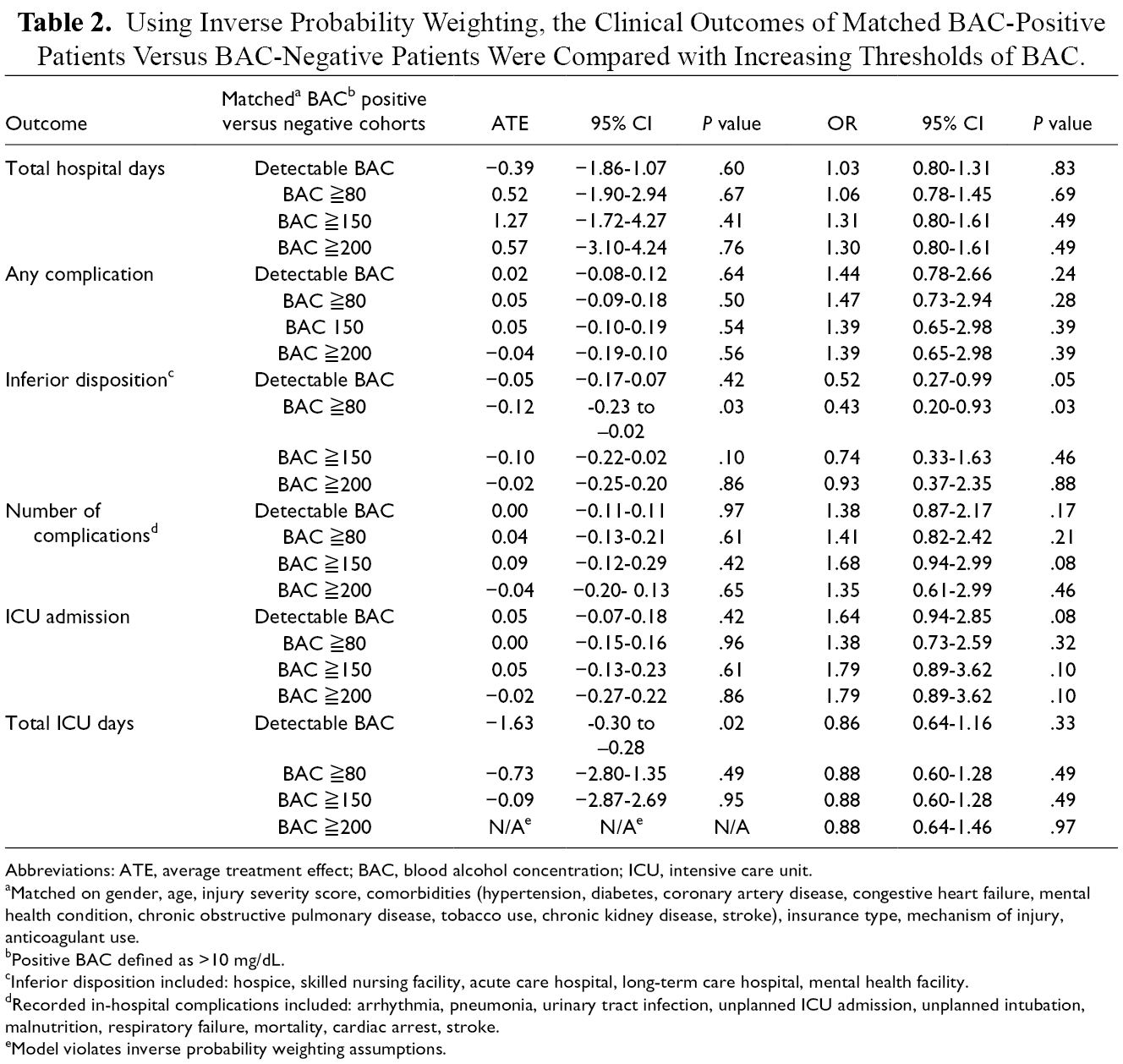
Abbreviations: ATE, average treatment effect; BAC, blood alcohol concentration; ICU, intensive care unit.
aMatched on gender, age, injury severity score, comorbidities (hypertension, diabetes, coronary artery disease, congestive heart failure, mental health condition, chronic obstructive pulmonary disease, tobacco use, chronic kidney disease, stroke), insurance type, mechanism of injury, anticoagulant use.
bPositive BAC defined as >10 mg/dL.
cInferior disposition included: hospice, skilled nursing facility, acute care hospital, long-term care hospital, mental health facility.
dRecorded in-hospital complications included: arrhythmia, pneumonia, urinary tract infection, unplanned ICU admission, unplanned intubation, malnutrition, respiratory failure, mortality, cardiac arrest, stroke.
eModel violates inverse probability weighting assumptions.
Discussion
Overall, there was no association between poor in-hospital outcomes of older patients after trauma and any level of detectable BAC, nor with increasing thresholds of BAC. While patients with any detectable BAC had higher proportions of inferior disposition and in-hospital complications, this relationship weakened substantially for disposition and became insignificant for complications when accounting for other patient-level factors with inverse probability weighting. BAC testing of this population was relatively low at 33%, and only 12% of tested patients were alcohol-positive patients. Nonetheless, one-third of alcohol-exposed patients had high levels of BAC (≧200 mg/dL), and one-third of those did not have a previously diagnosed alcohol misuse disorder.
Alcohol intoxication is a risk factor for injury, but research on how alcohol specifically affects the older trauma patient has been limited. A prior propensity score-matched study of National Trauma Data Bank showed that adult trauma patients testing positive for alcohol (≧80 mg/dL) had lower mortality and no significant difference in hospital length of stay versus their alcohol-negative counterparts. 15 Several other studies have shown similar clinical outcomes of alcohol exposed and unexposed patients when accounting for injury severity. 16 -18 The existing evidence is less consistent in the older trauma patient population. In 1 published study, mortality rates were higher in older patients, although this was an unadjusted estimate in an alcohol-positive cohort with higher ISS than alcohol-negative patients. 19 Small-scale studies of older trauma patients have produced conflicting results likely due to differing methods of controlling for confounders and comorbidities. Differences shown in outcomes previously for older patients are likely multifactorial and highly influenced by preinjury baseline functional status and comorbidities. While we could not control for preinjury frailty or other measures of baseline function, our analysis accounted for many known confounders of outcomes after trauma.
While illicit and nonprescribed drug misuse has increased in recent years, alcohol continues to be the most commonly used substance among older adults. 20 In the 2014 National Survey on Drug Use and Health, 978 000 older adults in the United States were found to have an alcohol use disorder. 21 Yet, as we found in our study, screening rates remain low for older patients. Despite the ACS requirement for counseling for alcohol-positive patients and recommendations from the Institute of Medicine for mandatory alcohol screening of all trauma patients, recent studies still show a testing bias with younger patients more likely to be tested than older patients. 4,22 Our study has a similar alcohol-screening rate in older patients found in a study using NTDB data 23 (31.5%), although other single study statewide data have reported screening rates as low as 5.2%. 4 In comparison, when considering all adult trauma patients, alcohol screening is approximately 50%. 7,23 These low screening rates are likely influenced by physician bias, which is concerning given the clinical sobriety exams and patient self-reporting of alcohol use lack accuracy for a patient’s BAC, 24,25 and there are large numbers of older adults with alcohol misuse disorder.
Alcohol may bias injury assessment and result in mistriage of patients. Despite similar ISS between BAC-positive and BAC-negative patients, a higher proportion of BAC-positive patients were not activated as a trauma alert suggesting alcohol may contribute to the undertriage of older trauma patients. Additionally, a higher percentage of alcohol positive patients initially went to another hospital prior to transfer to our Level 1 trauma center, even though the level of intoxication did not differ between transfers and direct admits. In our study, mechanisms of injury of alcohol-positive patients were unique, with higher incidences of falls and assaults including gunshot wounds. Alcohol use is a known modifiable risk factor for falls and gun violence. 26,27 Hence, alcohol screening and counseling should be incorporated into secondary fall and violence prevention programs, specifically targeting older patients.
To our knowledge, this is the first study to examine if a dose-dependent relationship exists between alcohol and poor outcomes after trauma in an older population. Similar studies have been conducted for traumatic brain injury 13,28 and for a general trauma population, 29 both showing that high levels of BAC actually have a protective effect on mortality and injury severity. Conversely, we did not show a protective effect of alcohol on our older adult population. While these in-hospital outcomes may not be negatively affected by preinjury alcohol intoxication, those with an alcohol use disorder have high rates of trauma recidivism, 30 -32 so their inferior outcomes may only be captured with a longitudinal study. Using an injury hospitalization as an opportunity for screening and intervention for alcohol use disorders in older patients may reduce long-term morbidity and mortality in this at-risk population.
Limitations
Limitations of our study include the inherent error introduced with a retrospective design. While BAC on arrival does not accurately represent BAC at injury, most of the patients arrived at the hospital within an hour of emergency medical services arrival, and thus BAC within an hour of arrival closely mirrors BAC at the time of injury. Furthermore, with only 1 in 3 patients undergoing early BAC screening, there may be a selection bias in our study population. Urine drug screens were also incomplete in this population, and hence we could not analyze the correlation of drug use with alcohol use. While using inverse probability weighting reduced bias in our analysis, it also prevented the investigation of the outcome of mortality as the model violated the treatment overlap assumption, which assumes each individual has a positive probability of being either alcohol positive or alcohol negative with an outcome of mortality. In our study, when controlling for the various confounders, the probability of being alcohol positive with an outcome of mortality was negative, and therefore, the average treatment effect could not be estimated.
Conclusion
Our study, using an inverse probability weighting model, did not show worse outcomes in older trauma patients who presented with alcohol exposure, nor did increasing intoxication correlate with a higher likelihood of inferior outcomes in a dose-dependent manner. Screening rates in this population were low, and all trauma patients, regardless of age, should undergo routine alcohol screening given the reported incidence of alcohol use disorders in this population and the high percentage of patients with very high BAC levels (≧200 mg/dL) in our study. While alcohol can influence a patient’s treatment course after injury, these results suggest that alcohol intoxication may not be the most influential factor in an older adult patient’s prognosis after injury and may not have the protective effect seen in younger patients, although further research is warranted to analyze the relationship between alcohol and trauma outcomes in older patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.