
Abstract

Traumatic hernias are known to occur after both blunt and penetrating mechanisms and are associated with significant concomitant injury risk. 1,2 Traumatic disruptions of the abdominal wall, diaphragm, and chest wall, while well known, are generally considered rarer findings across a spectrum of all injury types and potentials. The incidence of each traumatic hernia occurrence is varied, and ideal management efforts continue to be debated. After a review of the literature, the finding of all 3 traumatic hernias developing concurrently in the same patient has not been described. We report the case of a female trauma patient involved in a motor vehicle collision, presenting with the traumatic abdominal wall, diaphragmatic, and pulmonary hernias, as well as a review of the literature for the incidence of these injuries and their management strategies.
A 40-year-old woman presented to the trauma bay after a motor vehicle collision. The patient was stabilized, and the imaging was obtained. The patient was found to have traumatic disruption of the right lateral abdominal wall, left hemidiaphragm, and left chest wall with resultant acute, visceral herniation. The left-sided diaphragmatic defect contained herniated stomach (Figure 1). The right lateral abdominal wall defect contained small bowel, right colon, and hematoma (Figure 2). The left-sided chest wall defect contained a small component of the lower lobe of the left lung (Figure 3). The patient was taken to the operating room where a laparotomy was performed initially. Small bowel and colonic contusions were noted, but no other solid or hollow viscus injuries were identified. The small bowel and colon were reduced from the abdominal wall defect, and the approximately 14 × 20 cm defect was closed with direct tissue approximation and an underlay with biologic mesh. The left hemidiaphragm was then inspected. The stomach was reduced, determined to be uninjured, and the diaphragm was repaired primarily. A limited left thoracotomy was then performed to explore the intercostal defect. The lung was noted to be viable and easily reduced. The intercostal defect was closed by reapproximating intercostal musculature primarily and closing the ribs of the associated interspace disruption with multiple figures of 8 absorbable sutures. A chest tube was placed and the patient was transferred to the recovery room in stable condition. The patient went on to recover uneventfully.
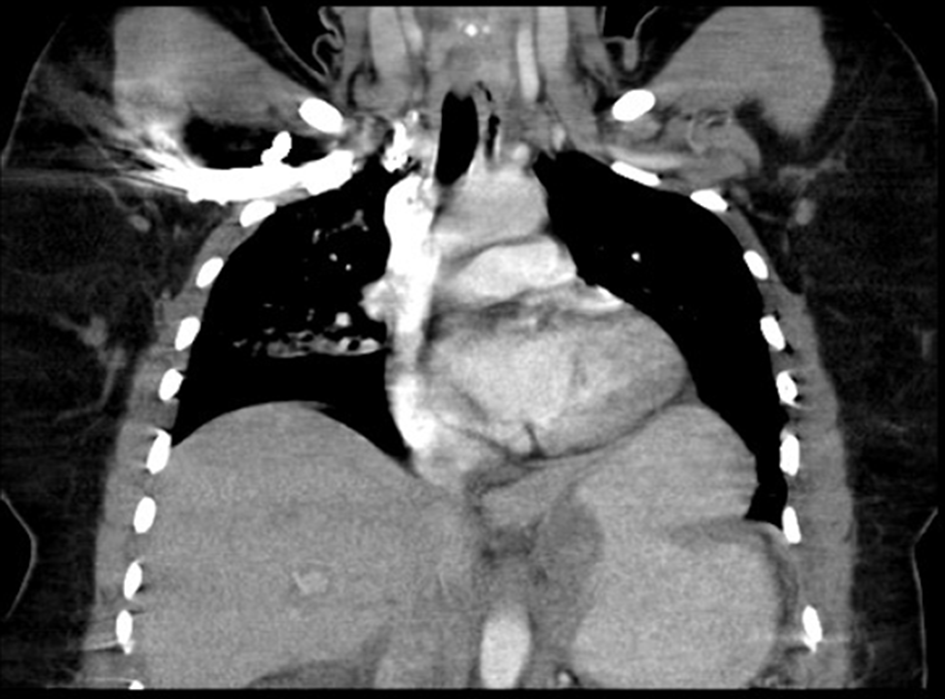
Cross sectional imaging revealing diaphragmatic hernia.
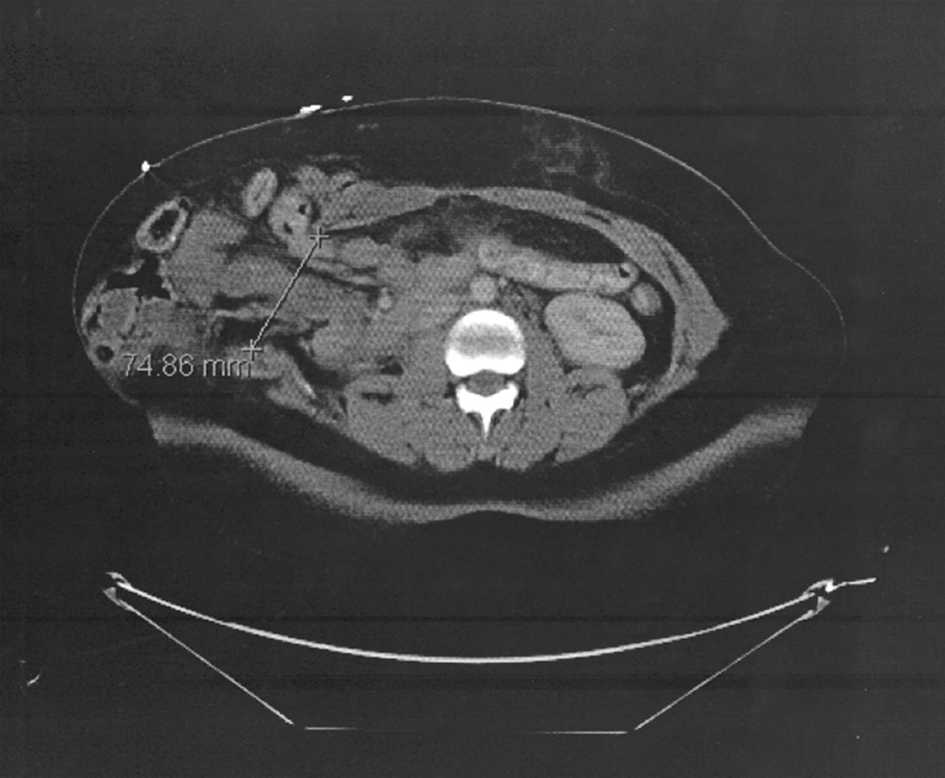
Cross sectional imaging revealing abdominal wall hernia.
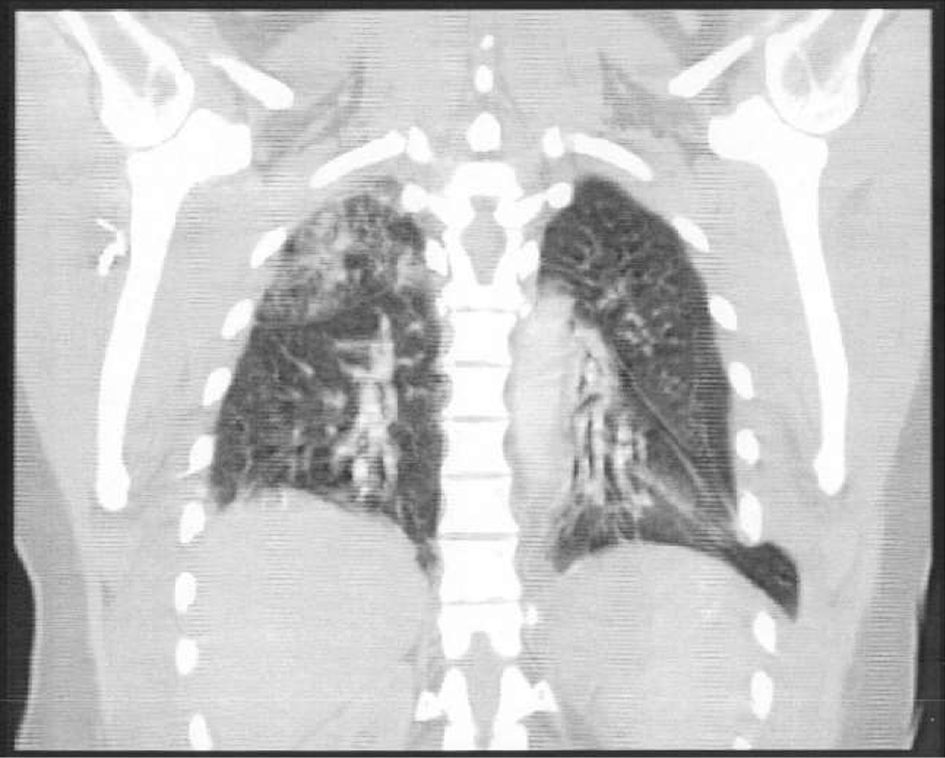
Cross sectional imaging revealing pulmonary hernia.
Traumatic hernias are a recognized complication after both penetrating and blunt injury mechanisms and may be identified acutely or in a delayed fashion. Traumatic hernias are known to have an associated injury risk which makes these findings a harbinger for additional or more serious patient harm after trauma. Roughly half are associated with small bowel injuries that require resection, 1 so timely identification and management are paramount. Disruptions of the abdominal wall, diaphragm, and chest wall are regarded as being rarer entities as propagated by the peer-reviewed literature. However, it is more likely that all 3 types have higher occurrence rates than estimated and are simply under-reported. Nonetheless, the findings of all 3 types of traumatic hernias occurring concurrently in 1 patient are unusual and provide the opportunity to review traumatic abdominal wall hernias (TAWHs), traumatic diaphragm hernias (TDHs), and traumatic lung hernias (TLHs) as well as their management considerations and strategies.
Based on the literature review, TAWH seems rare, but are likely under-reported. 1 TAWHs are estimated to be found in 15 000 patients each year with an incidence of 0.17%-1.5%. 1 TAWHs are most commonly encountered after motor vehicle collisions; however, pedestrian versus auto and motorcycle collisions are other frequent mechanisms of injury. Other causes include bicycle accidents related to handlebar injuries, falls, as well as crush injuries. Most frequently, the diagnosis is made during emergent laparotomy or CT imaging. TAWHs have been reported to occur with concomitant injuries in 95% of cases. 1
The management of TAWH varies substantially and is dependent on patient stability and concomitant injuries but approximately 44% of patients require urgent laparotomy or laparoscopy for additional injuries. 1 In stable patients, laparoscopic management is possible. Depending on patient stability, size of the defect, risk of strangulation, and the presence of abdominal contamination due to hollow viscus injuries, repair of TAWH is a matter of surgeon’s preference; however, a tension-free closure is paramount 2 to help reduce short-term and long-term hernia recurrence risk. In emergency settings, an increased risk of infection may limit the repair to the use of biologic mesh, but if stability permits a delayed repair, synthetic mesh application has shown greater long-term durability. 2
Diaphragmatic rupture with abdominal organ herniation was first described in 1541 by Sennertus. 3 According to Testini et al, roughly 5% of trauma admissions are associated with TDH. 3 The incidence of diaphragm injuries is higher in penetrating trauma than in blunt trauma, at a rate of 10%-19% compared with 5% and is most commonly found on the left side (>80%). 3 Concomitant injuries are frequently identified with TDHs. The diagnosis of diaphragmatic injuries is difficult and frequently delayed. A high index of suspicion should be kept for thoracoabdominal injuries in both penetrating and blunt trauma. TDH is frequently found on the left and should be repaired early when possible. When identified in a delayed fashion, TDHs may result in complications of organ incarnation, strangulation, and increased complexity and morbidity of repair efforts. 3
When diagnosed acutely, emergency surgery is the treatment of choice. The ideal surgical approach is varied and must be individualized to the stability of the patient and concomitant injuries identified preoperatively. Laparotomy and primary repair are more often employed, but TDHs are often identified and successfully repaired during laparoscopic, thoracotomy, or thoracoscopic approaches. 3 When treatment is delayed, a thoracic approach may be required due to viscera-pleural adhesions. 3 Although the type of closure used for diaphragmatic hernias is still a matter of debate, it is generally accepted that most defects can be primarily closed with a nonabsorbable suture. 3 Mesh repair may be required when the defect is too large to allow for primary closure. More recently, the biologic mesh has been introduced as an alternative to synthetic mesh products touting a lower rate of hernia recurrence, higher resistance to infections, and lower risk of displacement 3 ; however, limited evidence in the literature exists supporting biologic meshes long-term superiority.
In 1499, Roland is credited with reporting the first case of TLH, and since that time, approximately 300 cases have been described in the literature. It is estimated that trauma is the cause of 85% of TLHs, 4 with blunt mechanisms more frequently resultant of chest wall disruption and lung herniation than penetrating injury patterns. 4 The most common locations are the anterior intercostal hernias (98%). TLH by itself may not be particularly life-threatening; however, lung strangulation, pneumothorax, and pneumomediastinum may be present or develop. In the acute setting, the lung hernia can be repaired by primarily closing the intercostal muscles and approximating the associated rib space if the defect is small or amenable. With larger defects, intrathoracic coverage with biologic mesh may be needed in addition to chest wall closure.
A triple traumatic hernia is a rare entity and, to our knowledge, has not been reported in previous literature. More importantly, it should be recognized that traumatic abdominal wall, diaphragm, and chest wall disruptions represent the potential for additional injuries that may require urgent surgical intervention. Repair strategies for traumatic abdominal wall, diaphragm, and chest wall disruptions are varied and should be tailored to concomitant injuries, size of hernia defects, amount of contamination, and timeframe of identification of traumatic hernia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.