
Abstract

Surgical emergencies related to foreign body ingestion are an infrequent but highly morbid condition. In this report, we describe a case of an ingested toothpick causing small bowel perforation and intraabdominal abscess in a diagnostically complex patient.
A 65-year-old man with no past medical or surgical history presented to the emergency department (ED) with 5 days of abdominal pain, bloating, and partial obstipation. He had been seen in an outside ED earlier that week with similar complaints and discharged with diagnosis of enteritis. A recent colonoscopy was normal. His abdomen was soft, nontender, and moderately distended. A CT scan of the abdomen demonstrated a partial small bowel obstruction with transition point at the distal ileum, with associated mesenteric induration/inflammation and tethering of the bowel with traction against the superior right dome of the bladder. Due to the perplexing nature of these clinical and radiographic findings, the patient was taken to the operating room for diagnostic laparoscopy. Diagnostic laparoscopy revealed significant inflammatory changes in the right lower quadrant, with several surrounding loops of bowel, including the cecum, the small bowel, terminal ileum, and the sigmoid colon. Exploration of these loops revealed not appendicitis, but an intra-abdominal toothpick, which was completely walled off by several surrounding loops of bowel. The toothpick was removed, and all structures were carefully explored laparoscopically for an enterotomy, finding no evidence of small bowel, colonic, or appendiceal perforation. The patient had a rapid and uneventful recovery, and did not recall swallowing a toothpick.
Accidental ingestion of a toothpick is a rare cause of a surgical emergency. Intra-abdominal perforation of the ingested toothpick in the abdomen induces changes consistent with appendicitis, diverticulitis, ileitis, or lymphoma of the small bowel. 1 The small bowel and cecum are the most common site for perforation, followed by the cecum, as abrupt physiological luminal narrowing, bowel angulation, and the transition from a mobile to a more fixed portion of the bowel can predispose the rigid, pointed foreign body to infiltrate the bowel wall. 1 Further, the radiolucent nature of an ingested toothpick often impedes preoperative diagnosis through radiography; even with modern imaging techniques, toothpicks were apparent in only 14% of toothpick ingestions, while laparotomy (53%) and endoscopy (19%) are more commonly required for definitive diagnosis. 2 Despite the relative infrequency of toothpick ingestions, some large-scale data are available. A 1-year survey of emergency departments in the United States revealed 8176 toothpick-related injuries. 3 The primary risk factors for toothpick ingestion included impaired palatal sensation (particularly with alcoholics and denture-wearers), elderly patients (particularly those with dementia), children, eating foods containing toothpicks, and habitual toothpick chewing. 3 Toothpick ingestions were more commonly seen in men (88%), with a mean age of 54 years. 2 The most common presenting symptom was abdominal pain (70%), and only 12% of patients recall swallowing a toothpick. 2 Though toothpick ingestion is a rare surgical emergency, it is associated with an overall mortality rate of nearly 20%, 2 making early diagnosis and management an imperative.
Ingested toothpicks, with or without subsequent perforation, represent a rare cause of intra-abdominal surgical emergency. This case reminds physicians of the importance of clinical suspicion for repeated acute care visits for similar complaints in close frequency (Figure 1).
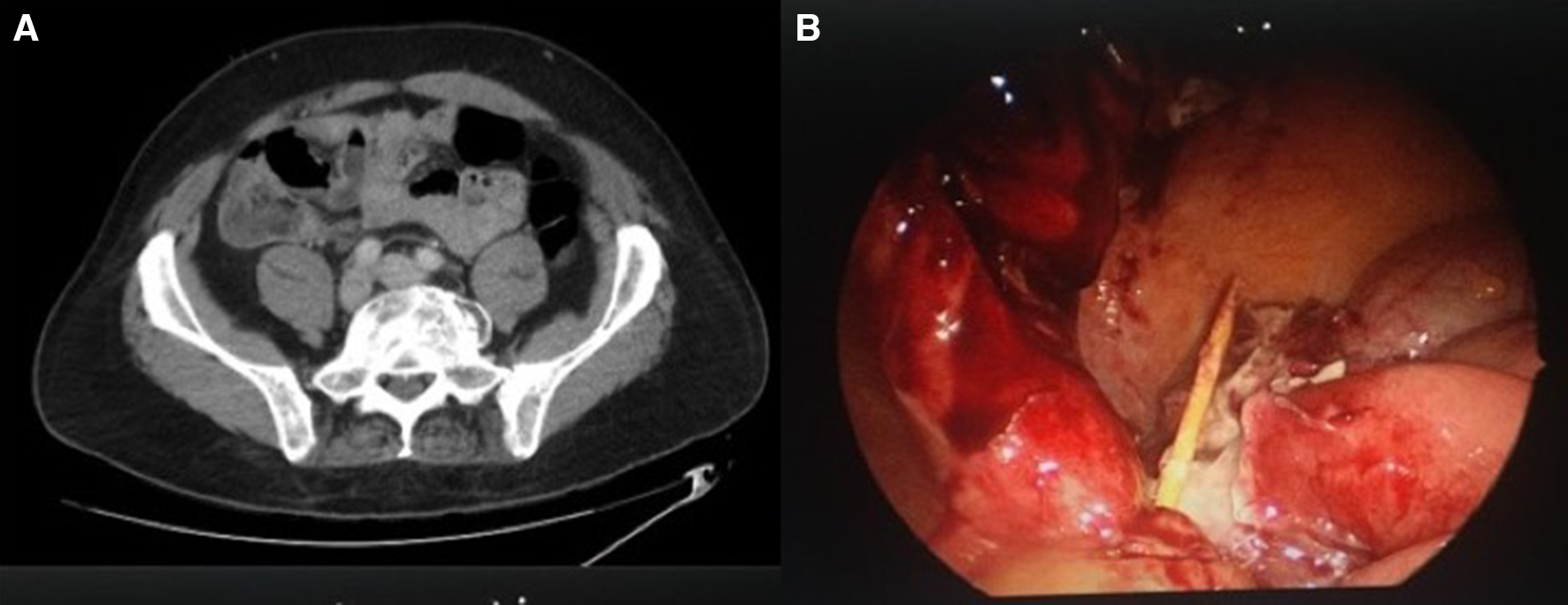
(A) Computed tomography scan demonstrating small bowel obstruction, tethering of the bowel, and induration of the adjcent mesentery. (B) Intra-abdominal foreign body identified on laparoscopy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.