
Abstract
This study evaluates the feasibility of retrohepatic inferior vena cava (RHIVC) resection without reconstruction in patients with end-stage hepatic alveolar echinococcosis (AE). Four hundred and fifty-seven patients diagnosed with hepatic AE and who underwent surgical resections between January 2010 and October 2018 were retrospectively analyzed. Nine patients receiving RHIVC resection without reconstruction were included in this study. Among the patients, 5 were male and 4 female. Mean follow-up time was 64.4 months (18-95). In this series, adequate collateral circulation was formed before operation in all patients, and 7 cases underwent ex vivo liver resection and autotransplantation (ELRA) and 2 cases underwent extended right hemi-hepatectomy. Average standard liver volume, graft volume, surgical time, and anhepatic phase in ELRA group patients was 1144 ± 127 cm3, 740 ± 235 cm3, 16.8 ± 4.1 hours, and 337.4 ± 108.65 minutes respectively. Average hospital stay time for all patients was 45 ± 36.4 days. There were no intraoperative deaths. The 30-day mortality rate was 11.1%, and total mortality rate was 22.2%. Postoperative complications occurred in 4 patients. During follow-up, no relapsed AE lesions were found. RHIVC resection without reconstruction is a feasible way for hepatic AE patients with adequate collateral circulation. Careful protection of collateral venous is the key factor for successful operation.
Keywords
Introduction
Human alveolar echinococcosis (AE), caused by the larval stage of Echinococcus multilocularis (E. multilocularis), is a lethal parasitic disease. 1 Northwest China and Tibetan regions are the most prevalent areas of AE. 2 Liver is the most affected organ due to the special life cycle of E. multilocularis. 3 AE lesions can involve the major liver vessels and even more remote organs, behaving like a malignant tumor. 4 The diagnosis of AE mainly depends on epidemiological evidence, clinical presentation, serology test results, and radiological examinations. 5 So far, surgery combined with 1-year albendazole medication has been considered a major radical procedure for clinically diagnosed AE patients. 6 However, due to absence of clinical symptoms in hepatic AE patients at early stages, most of them are at the advanced stage when diagnosed and seeking for treatment. 7
Hepatic AE with inferior vena cava (IVC) invasion is considered a terminal-stage condition, which makes the radical resection more difficult, and IVC usually needs to be excised for the purpose of R0 resection. 8 Thus, reconstructing the defected IVC is a challenge for surgeons. If the defect is large, artificial materials or other grafts are needed. Several types of auto-venous grafts, nonvascular grafts, and prosthetic grafts have been previously reported for IVC reconstruction.9-11 However, IVC reconstruction still does not achieve satisfactory results due to disadvantages of these grafts, including need for additional surgery, sacrifice of major visceral vessels, and risks of infection. 12 When AE lesions invade the retrohepatic inferior vena cava (RHIVC), there still exists controversy over whether IVC repair is always necessary. In this study, we describe nine cases with complicated hepatic AE patients, whose lesions had violated the RHIVC seriously, and all of them received RHIVC resection without reconstruction. Consequently, seven patients recovered well without recurrence of AE lesions. RHIVC resection without reconstruction for end-stage hepatic AE patients can also achieve better clinical results when adequate collateral circulation is formed.
Methods
Ethics
The study design and management of patients and controls were in accordance with the Helsinki Declaration and approved by the Human Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. 13 Written and signed informed consent was obtained from all patients or their legal custodies in their native language. Patients under the age of 18 were not included in this study.
Patients
We conducted a retrospective data analysis of 457 patients diagnosed with hepatic AE and who underwent surgical resections at the First Affiliated Hospital of Xinjiang Medical University From January 2010 to October 2018. Among them, IVC was invaded in 97 patients. Due to relatively serious IVC invasion accompanied by invasion of intrahepatic veins, 88 hepatic AE patients needed ex vivo liver resection and autotransplantation (ELRA), while the other 9 patients underwent partial hepatectomy. Among the 88 hepatic AE patients who underwent ELRA, 81 received IVC resection with reconstruction of proper grafts, while 7 received RHIVC resection without reconstruction. Moreover, invaded IVC was also removed and reconstructed in 7 patients undergoing partial hepatectomy, while IVC was not reconstructed in 2 patients because of their formation of adequate collateral circulation. Thus, 9 patients undergoing RHIVC resection without reconstruction were included in the study to discuss the feasibility of this technique in hepatic AE patients with the formation of adequate collateral circulation. The patients’ medical records were analyzed for demographic data, previous surgical history, clinical symptoms, therapeutic method, postoperative complications, and other follow-up results. All the patients were assessed by a multidisciplinary team (MDT), including hepatobiliary surgeons, hepatologists, interventional therapists, radiologists, and anesthesiologists before operation.
Detailed information of the patients is shown in Table 1. Among the 9 patients identified, 5 were male and 4 were female. Their ages at the time of surgery ranged from 19 years to 54 years, with a median age of 31 years. The mean follow-up time was 64.4 months (18-95). Among the cases, 5 cases were diagnosed during workup for nonspecific abdominal pain, and 4 cases were admitted to our hospital due to severe jaundice. Two patients had a previous history of liver surgery.
Demographic Characteristics and Main Laboratory Test Results of the Patients.
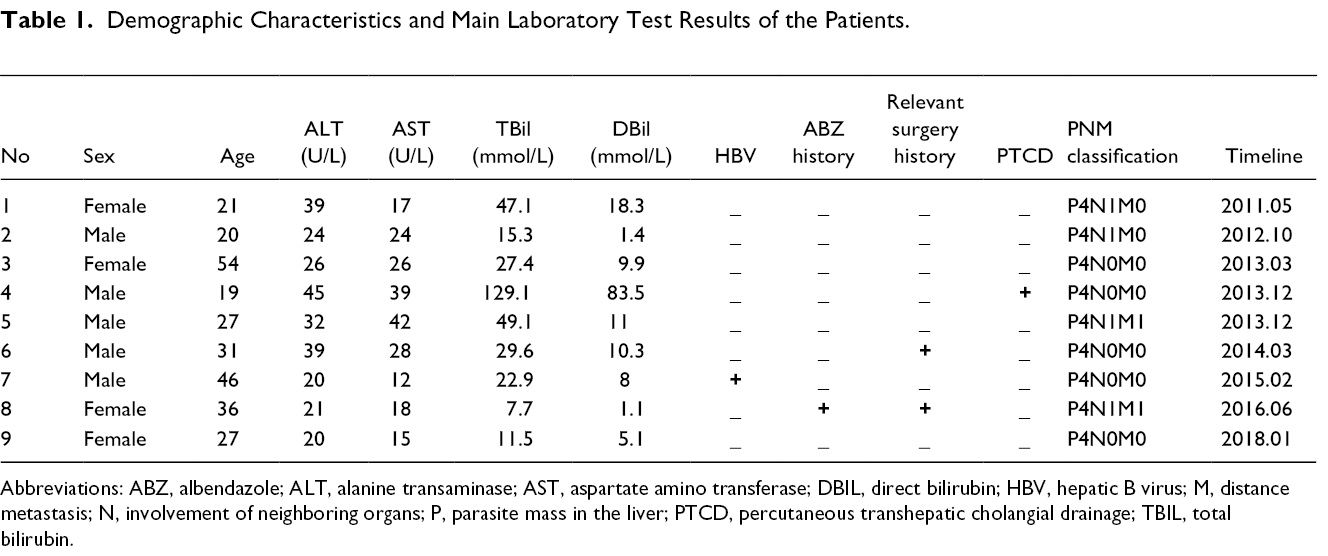
Abbreviations: ABZ, albendazole; ALT, alanine transaminase; AST, aspartate amino transferase; DBIL, direct bilirubin; HBV, hepatic B virus; M, distance metastasis; N, involvement of neighboring organs; P, parasite mass in the liver; PTCD, percutaneous transhepatic cholangial drainage; TBIL, total bilirubin.
Preoperative Assessment and Interventional Therapies
Preoperative computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET) scanning, and 3-dimensional (3D) imaging were used for assessment of lesion locations, extensions, hepato-caval, and portal hilum involvement as well as extra-hepatic metastasis. For all patients diagnosed with hepatic AE invading into RHIVC, a phlebography was carried out to identify the invasion degree of AE lesions and to confirm whether collateral circulation was well established. Preoperative percutaneous transhepatic cholangial drainage (PTCD) was performed in 1 patient, whose total bilirubin level was 129.1 μmol/L. Representative imaging photos are shown in Figure 1.
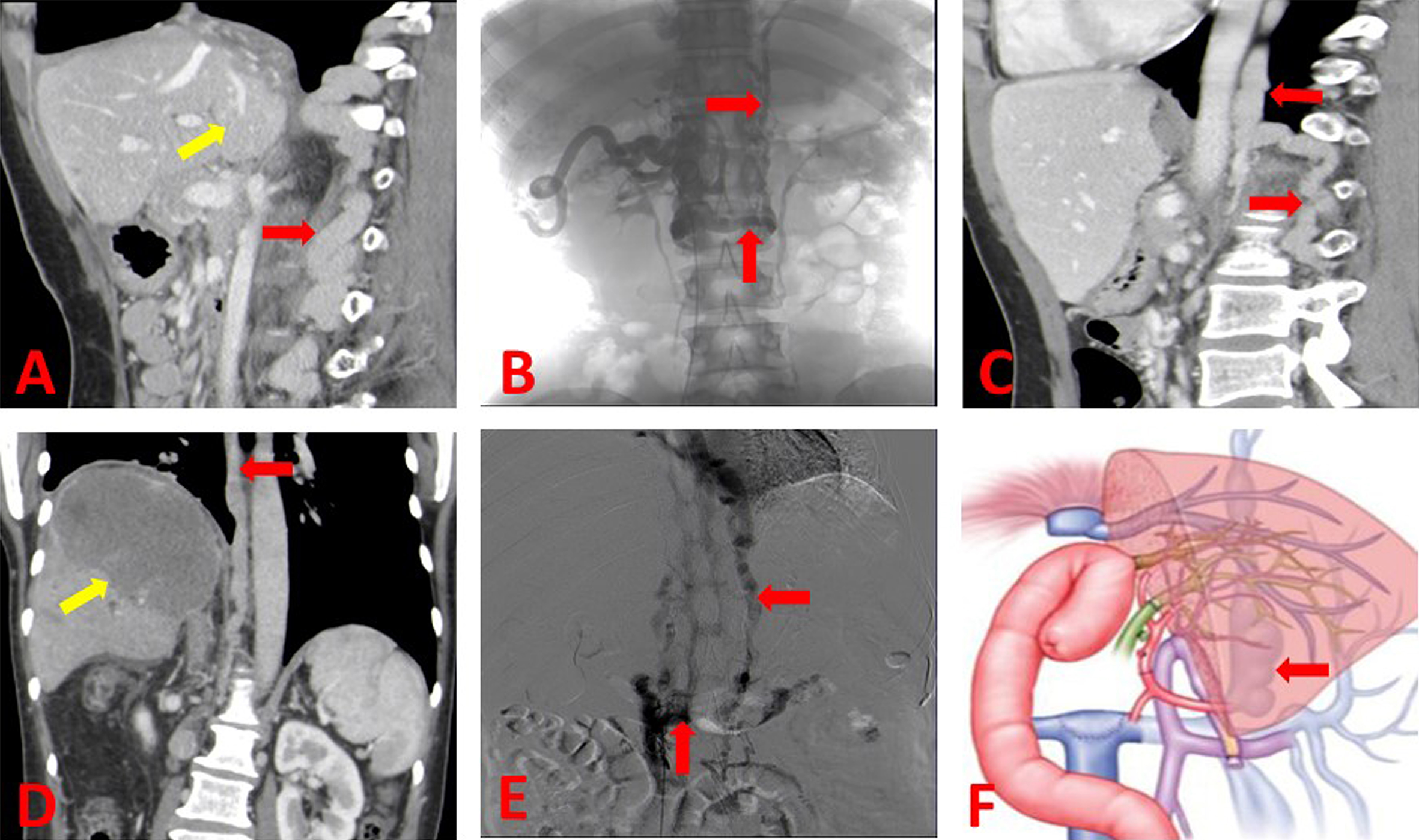
Representative imaging photos. (A) Abdominal CT shows the hepatic AE lesion (yellow arrow) and the formed collateral circulation (red arrow). (B) IVC angiography clearly demonstrates the collateral circulation (red arrow). (C) Abdominal CT shows the existence of collateral circulation after operation (A, B, C imaging photos for patients on whom extended right hemi-hepatectomy was performed). (D) Abdominal CT shows the hepatic AE lesion (yellow arrow) and the formed collateral circulation (red arrow). (E) IVC angiography demonstrates the collateral circulation (red arrow). (F) Diagram shows the collateral circulation after operation (D, E, F photos for ELRA patients). AE, alveolar echinococcosis; CT, computed tomography; ELRA, ex vivo liver resection and autotransplantation; IVC, inferior vena cava.
Surgery Process
Nine patients underwent RHIVC resection without reconstruction, and radical resection was achieved in all patients, among which 7 cases underwent ELRA and 2 cases underwent extended right hemi-hepatectomy. Surgery was carried out under general anesthesia. After careful surgical exploration, the extension of AE lesions was carefully reassessed Detailed surgery data are shown in Table 2. Before liver resection, we closed the IVC above the left renal vein for 5 minutes to observe whether there was an intestinal congestion, and whether the hemodynamic situation was stable, which aimed to further verify whether the collateral circulation was sufficient and it was necessary to reconstruct the posterior inferior hepatic vein. Due to careful assessment of collateral venous establishment through imaging before operation, the above test was successfully undertaken in all patients. Combined with preoperative angiography findings, when the RHIVC was completely blocked and the collateral circulation was adequate for further operation, the resection of the invaded RHIVC without reconstruction can be performed. During surgery, it was further suggested that the formed collateral circulation was fully compensated for hepatic blood flow in all patients. Thus, bypass was not used during the surgical procedure. Detailed surgery process is demonstrated in Figure 2.
Preoperative Lesion Characteristics and Surgical Results of the Patients.
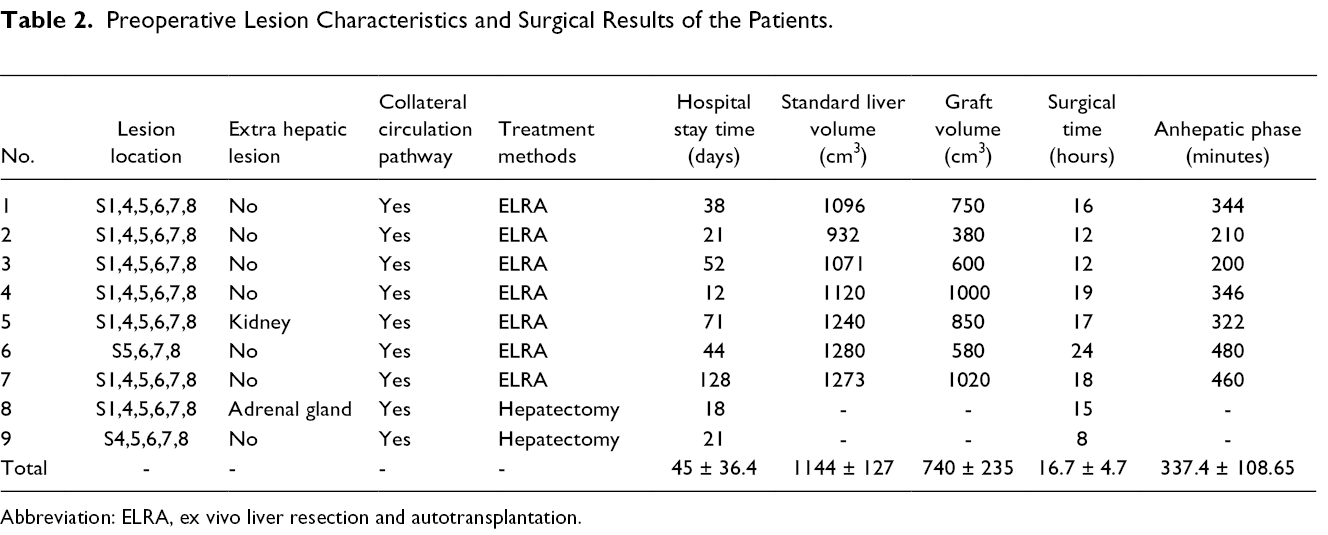
Abbreviation: ELRA, ex vivo liver resection and autotransplantation.
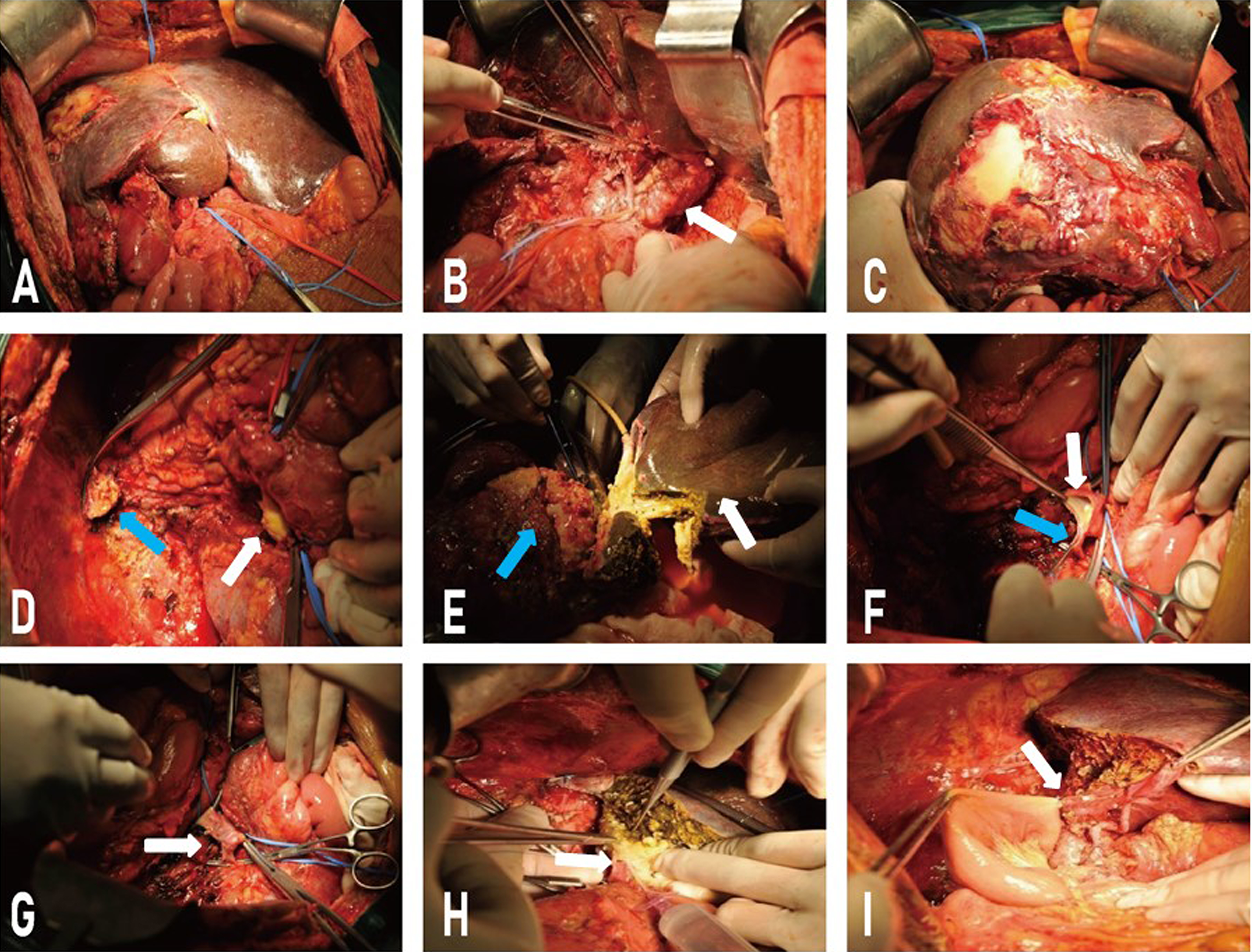
Surgical techniques. (A) Hepatic AE lesion and the hyperplastic liver. (B) Invasion of AE lesion into the caudate lobe (white arrow). (C) Hepatic AE lesion in the right lobe. (D) The suprahepatic IVC (blue arrow) and the infrahepatic IVC. (E) ELRA procedure, showing AE-free liver as the graft (white arrow) and AE lesion (blue arrow). (F, G) Closure of infrahepatic IVC (white arrow) at the level of and renal vein (blue arrow). (H, I) End-to-end anastomosis of left hepatic vein with suprahepatic IVC and infrahepatic IVC as well as end-to-end choledochal anastomosis and hepatointestinal anastomosis. AE, alveolar echinococcosis; IVC, ELRA, ex vivo liver resection and autotransplantation; IVC, inferior vena cava.
Follow-Up
Oral albendazole was administered as long as the patients’ liver functions were returned to the normal level or for at least 2 years as recommended. 14 The abdominal ultrasonography and/or CT, liver functions, and coagulation indexes were reviewed every 3 months within 1 year and every 6 months after 1 year. Postoperative complications were evaluated according to the Clavien classification system. 15
Results
According to the PNM (P: parasite mass in the liver, N: involvement of neighboring organs, M: distance metastasis) classification, 5 patients were P4N0M0, 2 patients P4N1M0, and 2 patients P4N1M1. 16 The AE lesions for all patients were mainly located in the right lobe and caudate lobe. Extra-hepatic lesions were located in the right kidney in 1 patient who received ELRA and in the right adrenal gland in 1 patient on whom hepatectomy was performed. The right hepatic vein and middle hepatic vein were invaded in 5 patients, and all 3 veins were invaded in 4 patients.
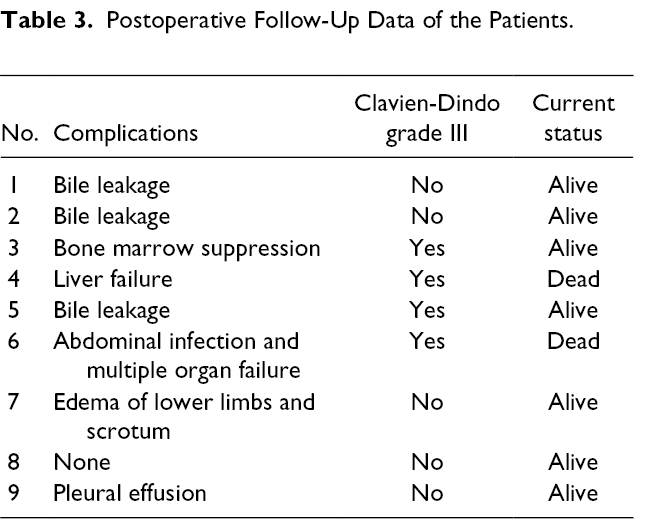
All patients involved in this study were followed up successfully. Median follow-up time was 64.4 months (18-95). There were no intraoperative deaths. One patient died of liver failure on the 14th day after operation, and another patient died on the 38th day after operation from multiple organ failure caused by severe abdominal infection. Postoperative mortality only occurred in patients undergoing ELRA, whose total mortality rate was 22.2% (2/9). Moreover, postoperative complications were mainly seen in patients with ELRA treatment. Complications occurring in patients receiving ELRA were as follows: bone marrow suppression occurred in 1 patient; low-output biliary leakage occurred in 3 cases which spontaneously disappeared within 12-30 days after operation; edema of lower limbs and scrotum appeared in 1 patient which lasted for a month, and the patient was cured by conservative internal medicine treatment. In addition, there was no acute kidney injury or sepsis in all patients during the surgical treatment and follow-up period. It may be due to better compensatory functions of the formed collateral veins. The remaining details are given in Table 3.
Postoperative Follow-Up Data of the Patients.
Discussion
Echinococcosis is a neglected zoonotic disease, causing great morbidity and mortality with wide distribution in its endemic areas, as China has a high disease burden of AE. 17 Due to its tumor-like characteristics with liver infiltration, severe damage to liver parenchyma, and invasion of blood vessels or biliary structures, hepatic AE is also called “worm cancer.”
Hepatic AE patients with the involvement of IVC, represented as advanced stage, require more complex and high risk intervention in spite of worse outcomes. A retrospective study by Aydinli et al has shown that palliative surgical procedures should be avoided due to high mortality rate. 18 They reported that patients with unresectable lesions, liver failure, and recurrent cholangitis were bound for liver transplantation, which accounted for 14% of all cases and lifelong medical therapy was needed. But all of this only had modest efficacy in terms of disease control, suggesting that due to the uncertain efficacy of medications and their possible side effects for patients’ liver functions, surgeons need to seek more radical approaches.19,20 Several centers have reported their previous experience of radical surgery for the treatment of end-stage AE patients, and achieved satisfactory outcomes.14,21 Wang et al recommend radical surgery for end-stage hepatic AE with IVC invasion, and in their report, the survival rate of hepatic AE patients undergoing hepatectomy with retrohepatic IVC resection was 91.55% (65/71) during the median follow-up time of 22 months, demonstrating that radical resection with R0 margin may offer the best chance for AE patients with long-term disease free survival. 22
Symptoms of IVC obstruction mainly depend on the obstruction level, including intravascular hypovolemia, liver damage, kidney damage, edema of lower extremities, and ileus, and so on. 23 In our study, all AE lesions for nine patients seriously violated the RHIVC, but none of them showed signs and symptoms when hospitalized. It was considered that the slow growth nature of AE lesions may display a chronic process of invasion, which offers the body enough time to establish collateral circulation.
In recent years, there have been many reports on IVC resection and reconstruction,24,25 and there are still few reports of IVC resection without reconstruction. 26 Alex et al proposed that resection without reconstruction can be performed after the establishment of collateral circulation for low-grade retroperitoneal sarcoma. In their report, 3 cases (9%) accepted IVC resection without reconstruction, and all these patients recovered well. 26 In addition, Hardwigse et al also reported IVC resection without reconstruction for 6 patients with hepatic carcinoma. 23 From our point of view, the reason that IVC resection without reconstruction was not widely accepted in patients of retroperitoneal tumors may be as follows: (a) retroperitoneal tumors grow rapidly and rarely form sufficient collateral circulation when invading IVC; (b) even if adequate collateral circulation has been established for some low-grade retroperitoneal tumors, it still needs wide retroperitoneal resection, which could destroy the established collateral reflux and cause serious postoperative complications. Fortunately, these above difficulties can be solved in hepatic AE patients. Unlike malignant tumors, the parasite grows very slow, which gives the organism enough time to form collateral circulation. Although most AE lesions invaded the RHIVC, it was relatively limited and required no extensive resection of the retroperitoneum. Therefore, it is feasible to perform IVC resection without reconstruction in hepatic AE patients.
It is crucial to determine whether established collateral circulation was sufficient to resect the RHIVC without reconstruction, and a preoperative IVC angiography was necessary to fully understand the establishment degree of collateral circulation. Besides, intraoperative temporary exclusion of intrahepatic vena cava can also be used to further confirm whether collateral circulation was adequate for operation. Importantly, for patients undergoing ELRA, on-table observation of hemodynamic stability and gastrointestinal venous congestion is the last step for verifying the formations of “rich collateral circulation.” The operation difficulty should be considered carefully to estimate all possibilities and to fully understand the pathological characteristics of AE lesions. For every case in our study, it was fully prepared before operation and offered 3 options to be chosen. If patients had stable hemodynamics, rich collateral circulation, and no intestinal congestion, the RHIVC can be resected without reconstruction. However, when patients had unstable hemodynamic situation, poor intestinal condition, and inadequate collateral circulation, caval reconstruction needed to be performed. Finally, caval reconstruction was still essential for patients who had stable hemodynamic situation and good intestinal condition without adequate collateral circulation.
Conclusions
To sum up, it is demonstrated in this study that RHIVC resection without reconstruction is a safe and feasible treatment for end-stage hepatic AE patients with adequate collateral circulation. Careful assessment of the collateral circulation formation through IVC angiography before operation and intraoperative protection of collateral venous are important factors determining the success of surgical procedures. Thus, the operation methods of RHIVC resection without reconstruction has the potential to achieve less risk and greater success rates when used for the treatment of more complicated hepatic AE patients.
Footnotes
Acknowledgment
The authors would like to acknowledge the technical support from the Department of Liver Hydatid Disease, Digestive and Vascular Surgery Center, The First Affiliated Hospital of Xinjiang Medical University.
Author Contributions
Bo Ran; Conception and design; Acquisition of data; Analysis and interpretation of data. Yusufukadier Maimaitinijiati; Acquisition of data; Analysis and interpretation of data. Aimaiti Yasen; Conception and design; Acquisition of data; Analysis and interpretation of data; Drafting the article. Tieming Jiang, Ruiqing Zhang, Qiang Guo; Data collection. Yingmei Shao; Conception and design; Provision of study material. Hao Wen; Conception and design; Provision of study material. Final approval of the version to be submitted. Tuerganaili Aji. Conception and design; Final approval of the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Design of this study and management of patients and controls were in accordance with the Helsinki Declaration and approved by the Human Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. Written and signed informed consent was obtained from all patients or their legal custodies in their native language. Patients under the age of 18 were not included in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Xinjiang Uyghur Autonomous Region Key Laboratory Open Research Program (Grant No. 2017D04004).