
Abstract
Introduction
Administration of chemotherapeutic regimens such as FOLFOX or CAPEOX with chemoradiation in the neoadjuvant setting, termed total neoadjuvant treatment (TNT), was introduced in recent years. By increasing the complete pathologic and clinical responses, patients with locally advanced rectal cancer may have better oncologic outcomes and potentially abstain from undergoing a proctectomy.
Methods
All patients who underwent TNT at a single National Accreditation Program for Rectal Cancer accredited referral center were included. A retrospective analysis was performed using a computerized Institutional Review Board-approved database. Patient demographics, diagnostic workup, treatment regimens, and surgical and pathological reports were reviewed. Complete pathological response was the primary outcome. Univariable and multivariable logistic regression analyses were performed to identify potential factors predisposing to complete pathological response.
Results
Thirty patients met the inclusion criteria, 14(46.6%) of whom had complete pathologic response. There was no difference in baseline demographic characteristics between patients who achieved complete pathological response and those who did not. Pathology revealed a 92% intact mesorectum rate in the complete pathologic response group and a mean of 24 harvested lymph nodes in the entire study cohort. Both univariable and multivariable logistic regression analyses failed to demonstrate statistically significant factors predicting complete pathologic response, magnetic resonance imaging (MRI) tumor size, and posttreatment MRI lymph node positivity.
Conclusion
TNT is safe and efficient for patients with locally advanced rectal cancer. It increases complete pathological and clinical response rates and may more widely evolve to be the treatment of choice in this group of patients in the near future.
Introduction
The treatment of rectal cancer has undergone tremendous change during the past several decades. Total mesorectal excision, introduced by Heald et al, 1 decreased local recurrence rates from approximately 20%2-5 to ≤5%.4,6-8 Other important improvements occurred with the introduction of neoadjuvant chemoradiation 5 and the implementation of preoperative magnetic resonance imaging (MRI) assessment. 9 A more recent advance in the treatment of rectal cancer was the introduction of total neoadjuvant treatment (TNT). The idea of administering the full chemotherapeutic regimens consisting of modified 5 fluorouracil and oxaliplatin (mFOLFOX6) or capecitabine and Oxaliplatin (CAPEOX) upfront with radiation in the preoperative setting is gaining popularity with emerging data on its efficacy.10,11 Administering TNT prior to surgery obviates the need for postoperative adjuvant therapy, which can be occasionally delayed by the presence of a stoma and/or by postoperative complications. However, a longer interval between neoadjuvant therapy and surgery increases the rates of complete pathological response, which has shown to be associated with better disease-free survival. 12 This method of administration of chemotherapy and radiotherapy potentially affords the patient the highest possibility of achieving a complete response. 10 Thus, in some patients with complete clinical response, rectal resections may be eliminated and can be followed in a “watch-and-wait” protocol. 13 We sought to review the initial results of the implementation of a TNT strategy for patients with rectal cancer in a high-volume National Accreditation Program for Rectal Cancer accredited referral center 14 .
Methods
A retrospective cohort analysis was performed using our computerized Institutional Review Board-approved database. All patients treated with TNT since its implementation in 2017 were included. TNT at our institution consists of neoadjuvant FOLFOX or CAPEOX followed by long-course chemoradiation therapy. Patient demographic information, including pre- and posttreatment MRIs, physical examinations, and chemotherapy regimens, along with operative and pathology reports, were reviewed. Complete pathological response was the primary outcome of this study and was defined as no tumor seen in the final surgical pathology specimen. Demographic variables, including pre- and posttreatment staging and surgical and pathological factors, were compared between the complete and incomplete pathologic response cohorts. A chi-square analysis was used for binary and categorical variables and a Wilcoxon rank sum test for continuous variables. A secondary outcome was the identification of potential factors predisposing to complete pathological response using univariable and multivariable logistic regression analyses. Factors to include in the multivariable analysis were determined by previous literature showing a significant relationship between posttreatment MRI staging and complete pathologic response.
Results
Demographics and Surgical Factors (Entire Cohort).
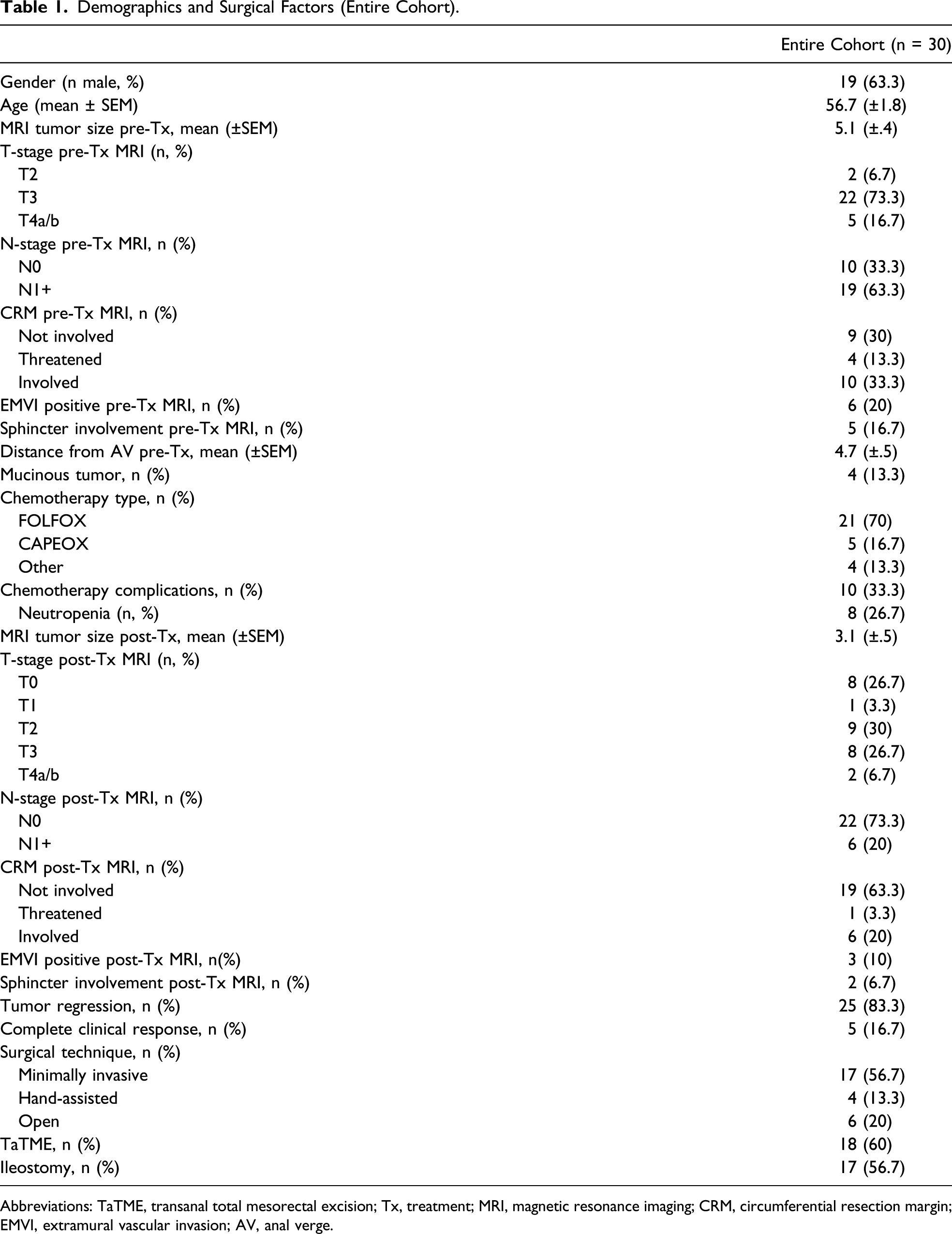
Abbreviations: TaTME, transanal total mesorectal excision; Tx, treatment; MRI, magnetic resonance imaging; CRM, circumferential resection margin; EMVI, extramural vascular invasion; AV, anal verge.
Demographic and Surgical Factors Noncomplete Pathologic Response vs. Complete Pathologic Response.
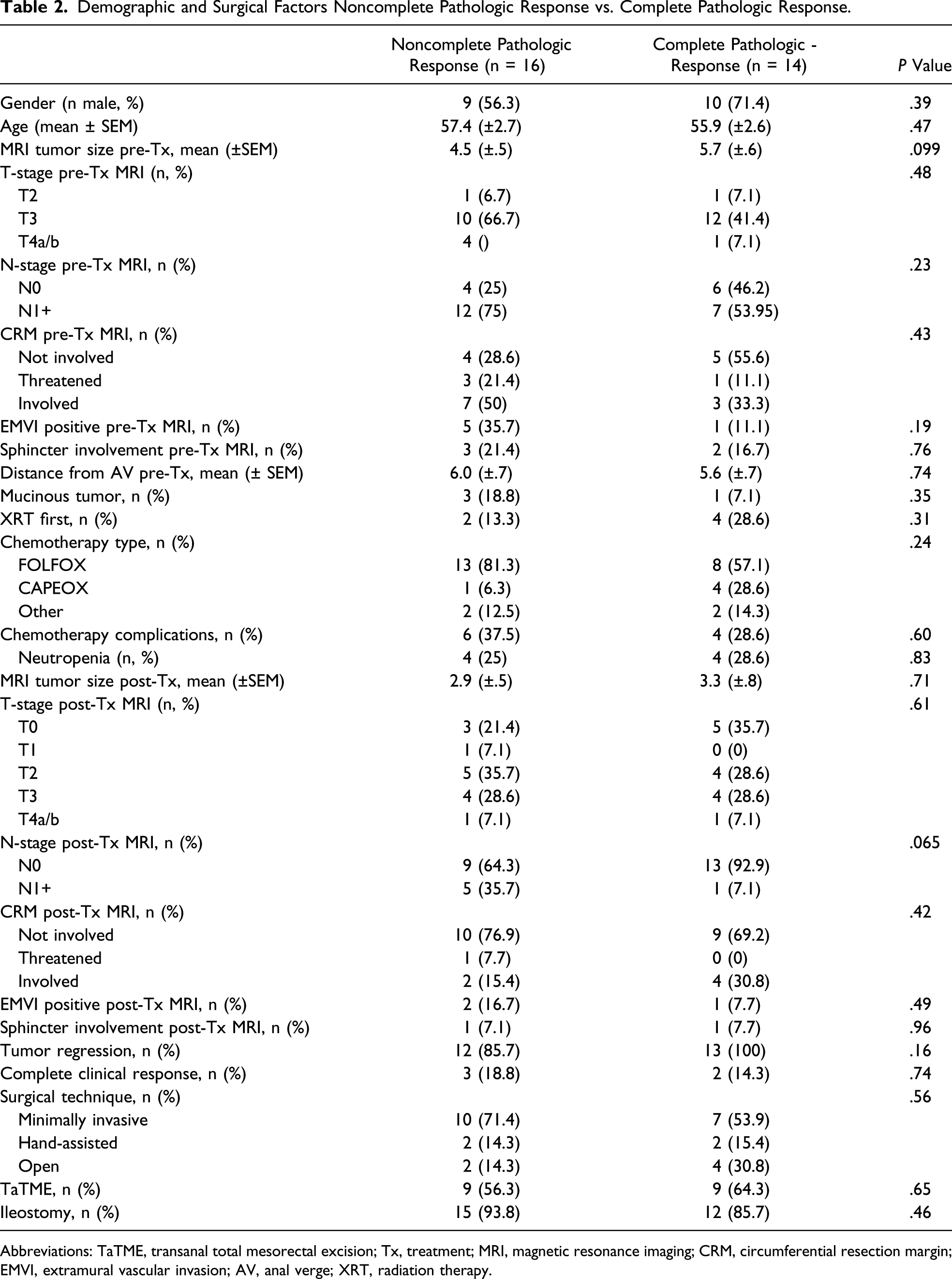
Abbreviations: TaTME, transanal total mesorectal excision; Tx, treatment; MRI, magnetic resonance imaging; CRM, circumferential resection margin; EMVI, extramural vascular invasion; AV, anal verge; XRT, radiation therapy.
Pathology Factors.
Abbreviation: LN, lymph node.
On multivariate logistic regression, none of the factors compared were found to be statistically significant in predicting complete pathologic response. However, positive lymph node status on posttreatment MRI showed a trend toward a worse pathologic outcome (Table 4).
Multivariable Logistic Regression Analysis.

Abbreviations: MRI, magnetic resonance imaging; Tx, treatment.
Discussion
The introduction of TNT for patients with locally advanced rectal cancer holds great promise as has been demonstrated in several studies.10,11 Thus, it has also been incorporated as a viable treatment strategy in the recent National Comprehensive Cancer Network guidelines. 15
In our initial experience, the complete pathological response rate of close to 50% is considerably higher than the rate with traditional chemoradiation therapy. We have been unable to identify factors that were able to predict complete pathologic response. A higher T-stage and larger tumor size on pretreatment MRI were shown to have a detrimental pathological outcome; however, due to the small cohort size, these results were not statistically significant. We did not find any difference in outcomes with administration of different chemotherapeutic regimens or with sequence of long-course radiation therapy (XRT) administration such as before or after chemotherapy. It has become our practice of choice to treat our patients with FOLFOX or CAPEOX followed by long-course chemoradiation therapy.
The administration of TNT did not have any negative impact on the surgical outcomes with a high rate of minimally invasive procedures (70%), good mean lymph node harvest (24.2), and a very high rate of mesorectal completeness (77%). The rate of postoperative complications was low, and most of them were minor. In this cohort, 93% of patients completed TNT; the incidence of treatable neutropenia was less than 30%.
In retrospect, some patients in this study who had complete clinical response (3 patients in the incomplete pathologic response cohort and 2 patients in the complete pathologic response cohort) were potential candidates for the “watch-and-wait” strategy. However, with the growing literature showing safety and benefit for a “watch-and-wait” strategy, we are now offering it to eligible patients. Thus, in our TNT cohort, patients with complete response on both MRI and sigmoidoscopy went ahead with surgery as planned at their initial presentation.
Our results present good short-term surgical and oncological outcomes. Due to its efficacy, favorable outcomes, and a low complication rate, TNT has become the mainstay of treatment for locally advanced rectal cancer at our institution. Longer follow-up is required to determine its impact on local recurrence and survival. In addition to the lack of a long-term follow-up, other limitations of this study are the small number of patients and its retrospective design.
A larger cohort is needed to identify potential factors predicting favorable pathologic outcomes and, thus, potentially selecting patients for a “watch-and-wait” path and deferring proctectomy.
In summary, TNT is a viable therapeutic option for patients with locally advanced rectal cancer. It may more widely evolve into the treatment of choice for the majority of these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential financial conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.