
Abstract
Background
Lung cancer screening (LCS) is broadly accepted. Screening also identifies incidental cardiac findings (S findings) that need follow-up. We report the magnitude of the potential downstream revenue generated by appropriate S finding management after 4 years of our free LCS program.
Materials and Methods
A retrospective database and chart review of a single-center free LCS program in the underserved southeast were performed. All patients who were enrolled in the screening required a primary care physician (PCP) as part of the decision-making model. Referrals to cardiac specialists for S findings found on LCS were recorded. Cost analysis was performed to track potential downstream revenue generated for the institution based upon Medicare allowable or Diagnosis-related group calculations.
Results
One thousand one hundred thirty-two scans were reviewed with 262 (23%) yielding positive S findings for 1 or more organ systems. 181/262 (69%) patients had cardiac findings, only 64/181 (35%) of these patients were referred to cardiology specialists by the PCP. The total Medicare billable amount for all cardiac referrals/interventions was $284 379, representing 35% of the potential billable amount of $804 260. Percutaneous coronary intervention (PCI) was the highest billable amount at $18 568. Eight percent of the patients undergoing appropriate cardiac evaluation required a PCI. If not for the screening and cardiac specialist referral, this patient group may not have received appropriate cardiovascular diagnosis and treatment.
Discussion
Lung cancer screening also identifies patients with significant cardiac disease, many of whom may not be appropriately referred. Identification and treatment of incidentally noted cardiovascular findings may both improve patient care and justify supporting free LCS programs.
Keywords
Introduction
Low-dose computed tomography scanning (LCDT) for lung cancer in high-risk individuals reduces lung cancer and cancer-related mortality. 1 Currently, the US Preventative Task Force (USPTF) recommends LDCT for adults aged 55-80 years who have a 30-pack year smoking history and currently smoke or who have quit within the past 15 years. 2 Our academic institution is located in the southeastern United States and uniquely provides free lung cancer screening (LCS) for a large population with varying and often diminished degrees of health care access. During the 4 years that our program has been active, our screenings of patients who met certain criteria have shown great success in both detection of malignancies and their early treatment. We have previously demonstrated that our geographic location has influenced our ability to detect a 2-fold increase in lung cancer prevalence as compared to national studies. 3 Recent sub-analyses of our data have demonstrated that the free LCS program generates institutional revenue, notably from incidental findings discovered in patients who otherwise had limited or no access to a primary care physician (PCP). 4 We have also previously demonstrated the increased downstream hospital revenue derived from our screening program with regards to surgical management, especially in regard to the detection of earlier stages of lung cancer. 4
Incidental findings (S findings) are often noted during screening and subsequently referred to the appropriate specialist. These referrals have been tracked for cardiology, pulmonology, gastroenterology, hepatology, renal, and thyroid findings. Due to overlapping risk factors within this patient population who have met nationally recognized criteria for LCS, the S findings are primarily cardiac in nature. The aim of this present study was to determine the breakdown of S findings and report the amount of downstream revenue generated with these referrals within our health system.
Materials and Methods
An institutional review board–approved retrospective database and chart review of our free LCS program in the underserved southeastern United States were performed over a 4-year period. Recruitment and eligibility for participation in our free LCS program have been described previously.3,4 Information on our LCS program has been distributed to providers of differing levels throughout our health care system. Our health care system consists of a large academic tertiary care center and multisite primary care and specialist clinics. We additionally have several institutional satellite clinics in rural areas. All patients who were enrolled in the screening required a PCP as part of the decision-making model. Primary care physicians evaluated referred patients for the screening program and performed an overall health assessment.
During the entire process of establishing a PCP visit, undergoing the LDCT, appropriate follow-up with pulmonology or thoracic surgery, any S findings were referred as deemed necessary with an appropriate cardiology referral. Examples of cardiac S findings include severe coronary calcification, valvular calcification, or cardiac hypertrophy. We tracked and recorded referrals made to cardiac specialists for S finding management. A cost analysis was performed to estimate the potential downstream revenue generated for the institution based upon Medicare allowable or Diagnosis-related group calculations. For purposes of this analysis, the end point we focused on was confined to cardiology S finding-related downstream revenues.
Results
One thousand one hundred thirty-two scans were reviewed with 262 (23%) positive S findings for 1 or more organ systems. Of these 181/262 (69%) patients demonstrating cardiac findings, only 64/181 (35%) of these patients were referred to cardiology specialists by the PCP. The total Medicare billable amount for all cardiac referrals/interventions was $284 379, representing approximately 35% of the potential Medicare billable amount of $804 260. If each patient exhibiting positive cardiac and other organ system S findings was appropriately referred, the total estimated Medicare billable amount exceeds $1 000 000, highlighting our findings that the major downstream revenue driver of S findings is cardiac incidental findings. Of the downstream procedures, percutaneous coronary intervention (PCI) was the highest billable amount at $18 569 per procedure followed by diagnostic cardiac catheterization and stress tests. Figure 1 depicts actual vs. total potential Medicare billable amounts for consultation, Electrocardiogram, echocardiography, stress test, cardiac catheterization, PCI, and cardiac rehabilitation. Twenty-seven percent of patients who were referred to a cardiologist and underwent appropriate cardiac evaluation had a cardiac catheterization. Eight percent of these patients received a PCI as a result of their catheterization findings. If not for the screening and cardiac specialist referral, this patient group may not have received appropriate cardiovascular diagnosis and treatment. Potential and actual downstream Medicare billable amounts from cardiac S findings found on lung cancer screening. Accumulative actual and potential billing recorded over 4 years of lung screening in 1132 scans with 181 cardiac S findings. Echo, echocardiogram; Cath, cardiac catheterization; PCI, percutaneous coronary intervention; Rehab, cardiac rehabilitation.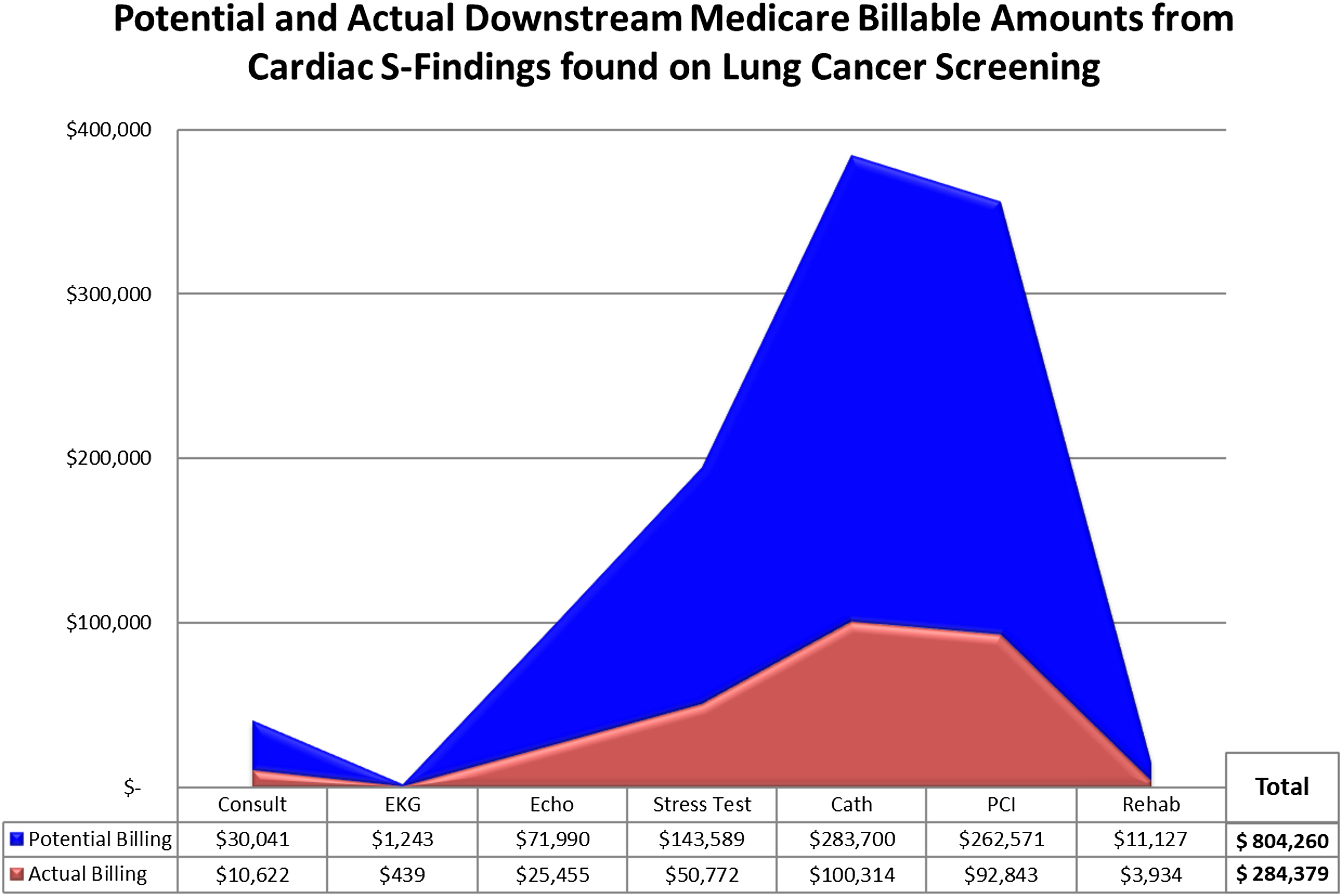
Discussion
Free LCS, particularly in our geographic region, has been shown to be of significant benefit to population health. Our region is characterized by a higher prevalence of patients with a significant smoking history or occupational exposure who meet recognized criteria for LDCT and may have poor access to health care otherwise. A PCP referral and relationship are initiated for the patients in our screening program. These patients are typically medically disadvantaged and are from predominantly rural areas. The ensuing comprehensive medical history and physical performed by PCPs resulted in appropriate referrals placed to other medical subspecialists. In our patient cohort, the overwhelming majority of the PCP referrals were to general cardiology and cardiology subspecialties.
The $284 379 collected by our institution from referred cardiac patients is approximately a 10th of the potential reimbursable income if all patients demonstrating an abnormal cardiac S finding had been referred. One challenge in our patient population is the lack of appropriate referral to a cardiovascular specialist in the vast majority of patients demonstrating abnormal cardiac S findings. Opportunities to enhance appropriate cardiovascular referrals in these patients include PCP education, community awareness programs, and for rural populations, further development of cardiovascular telemedicine programs.
Another benefit of enhanced screening programs would be the continued expansion of LCS programs. At our center, we have demonstrated that our free LCS program generates a net margin of $177 per case within a 3-year time period. 4
Expansion of LCS to those deemed ineligible by the classic USPTF guidelines has been shown to improve 5-year mortality rates after diagnosis. 5 A recently published Lancet article by Luo et al 5 demonstrated that expanding the screening program to those between 50 and 55 years of age as well as those with 30-pack year history but who had quit over 15 years prior led to increased diagnosis of early-stage lung cancer and potential improvement in mortality in high-risk populations. Increasing the volume of screened patients in high-risk populations is known to increase net health system cost. Despite these new expenditures, our data would suggest that the prevalence of cardiac S findings among this high-risk population may generate significant appropriate cardiovascular referrals at the institutional level. Our program’s data indicating that each patient receiving a free lung screening scan generates a positive margin at 3-year follow-up suggest that this influx of new cardiovascular patients may generate a positive financial impact at the health system level.
Limitations
This study’s limitation would include the single-center nature of this program, reflective of our program’s unique free lung cancer screening efforts. We also acknowledge that our tertiary care center serves a large portion of underserved patients who may not have had any health care services prior to enrollment in our LCS program and thus had more under- or untreated comorbidities that were discovered during their evaluations, reflected in the 23% S finding rate in our cohort to the expected rate of 10%-15%. 6 We acknowledge that the increased ordering of diagnostic tests with a subsequent increase in downstream health system revenue may be perceived as a conflict of interest. However, referrals generated by a patient’s PCP are made independently of the lung screening program’s input, and we believe that ensuring and promoting PCP autonomy in the specialist referral process are vital to our program’s success, maintaining compliance with clinically accepted standards of practice.
Beyond its public health benefits, LCS programs represent potential sources of watershed revenue to health systems7-9 via the identification of coexistent cardiovascular disease. Our free LCS program has yielded improvements in early cancer detection in a high-risk population and also identified co-prevalent cardiovascular disease in a significant percentage of screened patients. Enhanced collaboration between LCS programs and referring PCPs may promote appropriate subspecialist consultations. Downstream revenue generated by the clinical care of patients with cardiovascular S findings may further support free screening programs for patients otherwise unable to afford one. Additionally, earlier detection of non-pulmonary disease incidentally detected on CT may allow for earlier intervention and attenuation of disease progression, thereby achieving future cost savings. Further studies examining the impact of free lung screening programs on other medical and surgical subspecialties may aid in further describing the impact of screening programs on the financial performance of sponsoring health systems.
Footnotes
Author’s Note
This article was presented as a mini-oral at the AATS 99th Annual Meeting in Toronto, Canada, May 4th-7th 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
IRB approval Augusta University #775161.