
Abstract
Background
The present study was designed to evaluate the immediate consequences that the number of consulting physicians has on length of stay (LOS), in-hospital mortality, 30-day readmission rates, direct health care costs, and contribution margins.
Methods
A retrospective review of administrative databases for the years 2013 and 2014 was performed at the Florida Hospital Adventist Healthcare System.
Results
11 274 patients were included in the analysis. Total and variable costs increased by $1347 and $592, respectively, with each consulting physician service per patient. The contribution margin decreased by $354 per patient/consulting physician. Each consulting physician increased LOS by .72 days and increased odds ratio of mortality and 30-day readmission by 5% and 3%, respectively.
Conclusions
Our research suggests that each consulting physician added to the care of an individual surgical patient negatively affected LOS, readmission rates, in-hospital mortality, and costs.
Keywords
Introduction
Co-management, in which multiple consulting physicians participate in the care of hospitalized patients, is gaining popularity as more patients present with an increasing number of complex comorbidities. Multiple reports published over the last several years have addressed the role of dedicated hospitalist services that share responsibilities in the management of patients admitted to a variety of surgical specialists including vascular, 1 neurosurgery, 2 orthopedics, 3 and pediatric surgery. 4 In general, hospitalist services comprise internists who focus their practice on inpatient management. Hospitalists usually address basic care needs and rely on consultation of specialists for more specific necessities. 5
According to the Society of Hospital Medicine and the American Hospital Association, 6 an estimated 30 000 hospitalists are currently practicing in nearly one-third of hospitals throughout the United States. 7 Although likely multifactorial in nature, increasing numbers of frail elderly patients requiring longer hospitalizations, reimbursement constraints, and current resident work-hour limitations have contributed to the proliferation of these dedicated hospitalist services8,9 both in community and in academic institutions.
Despite the growing phenomenon in which the admitting surgeon relies on an alternative physician for a significant portion of the patient’s care, the available data are unclear as to whether this approach improves perioperative care and expedites discharge of patients postoperatively. Some studies have shown that involvement of a hospitalist may have favorable effects on in-hospital mortality rates, patient safety, and pain scores, 1 while others have found no differences in readmission rates or length of stay (LOS). 10 Some authors have proposed that having a hospitalist service available improves surgeon satisfaction, resource utilization, timeliness of patient care, communication among referring physicians, and house staff supervision. 11 Nonetheless, reports addressing the financial implications of a dedicated hospitalist service have shown mixed results. 12 Finally, the patient’s perception of having several providers managing their care has also been questioned.13,14
To date, the implications of having multiple physicians caring for the same surgical patient have not been evaluated in detail. Thus, the purpose of this study was to examine the consequences that consulting physicians have on patients admitted to surgical services. We focused our research in determining specifically the relationship between the number of consulting physicians involved in patient care and both clinical and financial outcomes including LOS, in-hospital mortality, 30-day readmission rates, costs, and contribution margins.
Methods
After obtaining approval from the AdventHealth Orlando Institutional Review Board, we retrospectively reviewed financial and clinical outcomes of surgical patients available from prospectively maintained administrative databases. Consecutive patients admitted to the Adventist Healthcare System in the Central Florida region for the years 2013 and 2014 were included in the analysis.
Admitting Institution
The Adventist Healthcare system is a not-for-profit health care system with 22 campuses throughout the state of Florida. Seven of these campuses are in the Central Florida region with a hybrid tertiary referral center that shares both traditional community and academic characteristics. The main campus is a 2247-bed acute care medical facility, with 2230 staff physicians where more than 122 729 inpatient admissions occur annually. Approximately 64 552 outpatient and inpatient surgeries are performed yearly.
Study Population
Types and Frequency of Procedures Included.
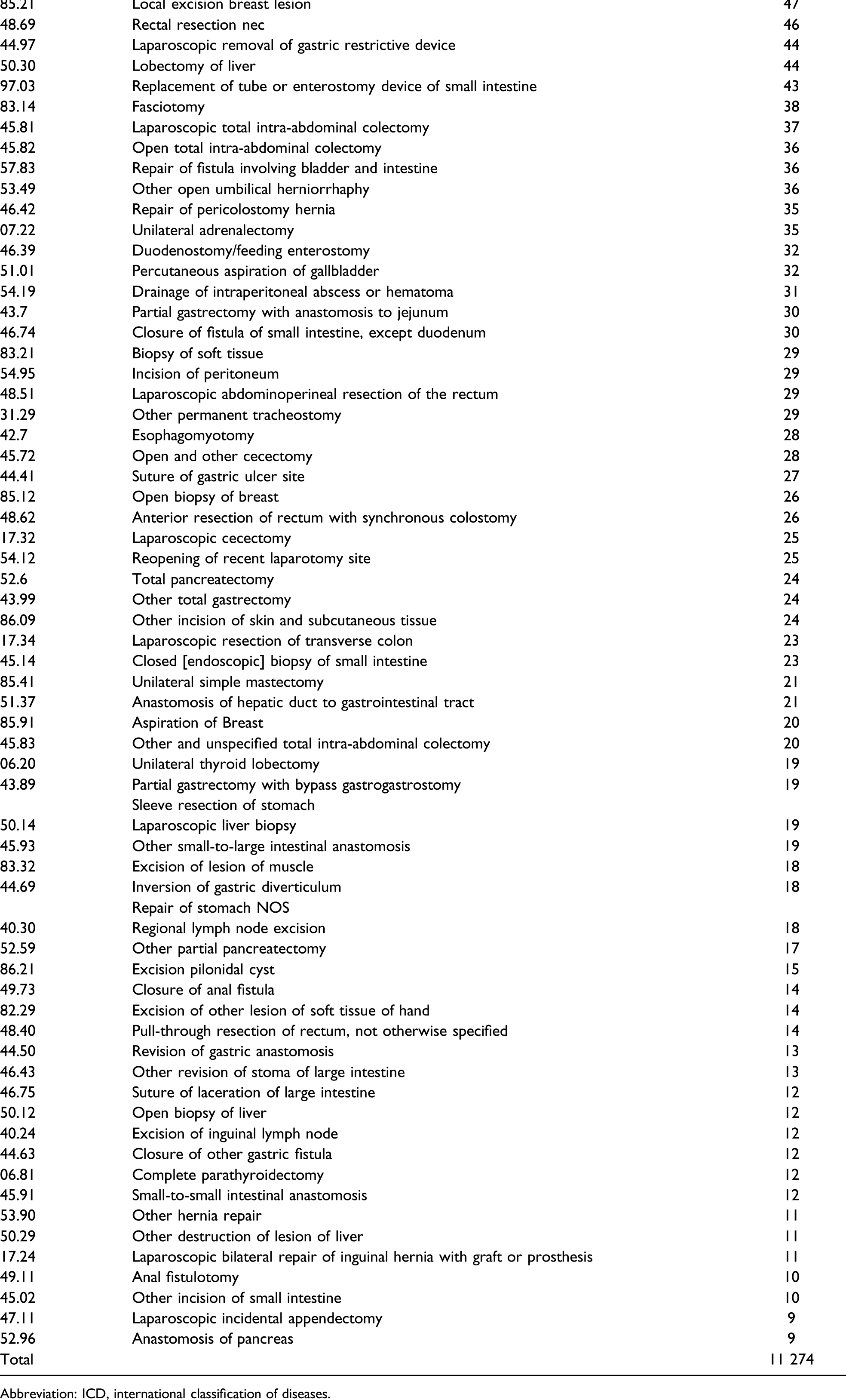
Abbreviation: ICD, international classification of diseases.
Consulting Physician
A consulting physician was defined as one that acted in an advisory capacity to the patient’s primary physician. The number of consulting physicians was matched to each study patient.
Financial Outcomes
This study’s hospital system uses commercially available financial software to categorize actual general ledger expenses as either variable or fixed costs. Total cost included fixed and variable costs and was defined as all variable and fixed hospital expenditures required to provide direct patient care and to operate the facility. Fixed costs were all expenditures that did not change with business volumes. Examples include management salaries, benefits as well as depreciation of equipment and buildings. Variable costs were defined as all expenditures that vary on the basis of changes in business volume including nursing and other direct patient care salaries, benefits, supplies, and drugs.
Each discharged patient was allocated a pro rata portion of the variable costs according to specific charges incurred. Contribution margin, an indicator of a hospital’s profitability, was defined as total actual payments minus variable costs as defined before. 15 Total cost, variable cost, fixed cost, and contribution margin were matched to each study patient. Since our primary focus was the hospital financial impact that the number of consulting physicians had on each patient care episode, we used total cost, variable cost, and contribution margin as outcomes.
Clinical Variables
The clinical variables studied for this research included LOS, mortality, and 30-day readmission rates. Mortality rates reflect only those individuals that expired within our health care system during the index admission. Readmission rates were analyzed using the patient’s unique medical record number that remains constant throughout the patient’s readmission to satellite locations. If one admission occurred within 30 calendar days after the previous discharge, the previous hospital visit was flagged as the one that caused a 30-day readmission event.
Statistical Analysis
We analyzed relationships between the number of consulting physicians during the patient’s hospitalization and financial outcomes including total cost, variable cost, and contribution margin, as well as clinical outcomes including LOS, mortality, and 30-day readmission. Multivariate linear regression was used to estimate continuous outcome measures including costs, contribution margin, and LOS. Multivariate logistic models were used to estimate binary outcome measures including mortality and readmission rates. We included the following covariates in the models in order to adjust for potential confounding factors: DRG relative weight, age, gender, insurance payer, admission source, admission type, APR-DRG risk of mortality and severity of illness, and ICD-9 principal procedure codes. Discrete variables including insurance payer, admission source, admission type, and ICD-9 principal procedure codes were coded as categorical variables; gender was coded as a binary variable. For each coded variable, the value with the largest percentage was utilized as default, so it would not be included in the final models (defaults = female, managed care, non–health care facility admission source, ER admission type, and laparoscopic cholecystectomy ICD-9 principal procedure).
Model evaluation and refinements were also conducted. Multicollinearity was evaluated for each multivariate linear regression model using tolerance and variance inflation factor (VIF), which indicates the degree of multicollinearity of each independent variable with the other independent variables in the model. All independent variables have a VIF < 3, which are less than 10, the value or higher indicating higher multicollinearity. Outliers for total cost, variable cost, contribution margin, and LOS were also checked and excluded from the final models based on outlier identification technique. All tests and 95% confidence intervals (CI) were two-sided. P-values less than .05 were considered statistically significant. For regression analysis, we reported our results in terms of estimated parameters, associated P-values, and adjusted R2 values from each model. For the logistic model, the results were reported in terms of estimated odds ratios, pseudo R2, associated P-values, and c-statistics from each model. All statistical analyses were performed using Stata® 13.1 software.
Results
Demographics.
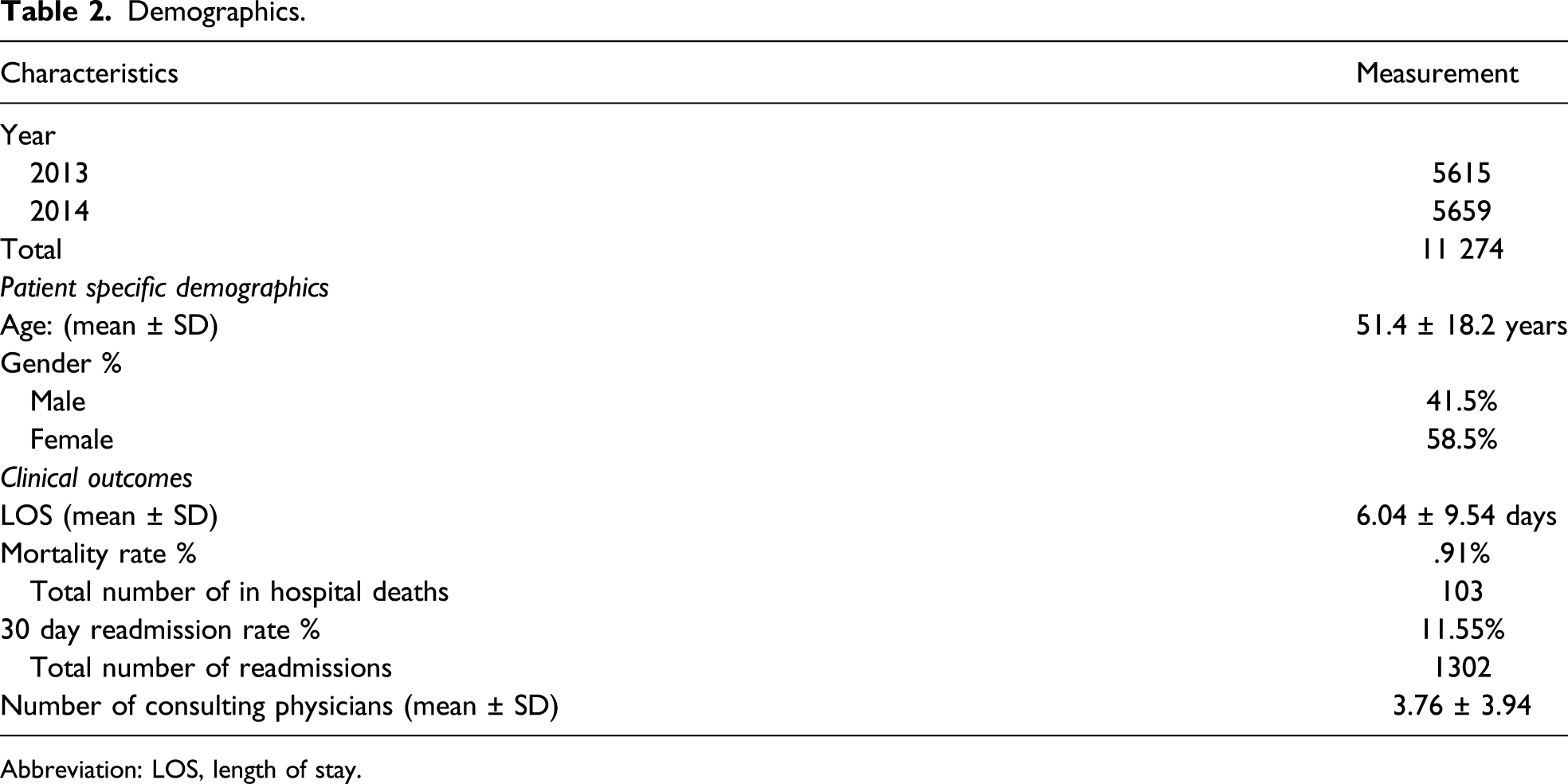
Abbreviation: LOS, length of stay.
Summary of Adjusted Model Parameter Estimate Results
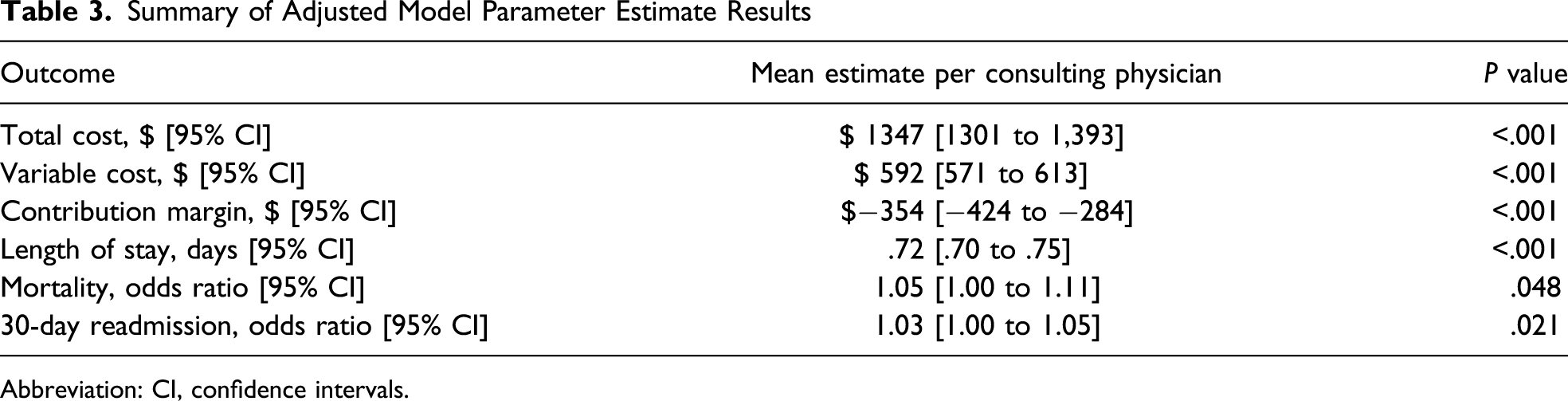
Abbreviation: CI, confidence intervals.
Influence of Payer on Financial Outcome (Mean Estimates)

Adjusted Model Mean Estimates.
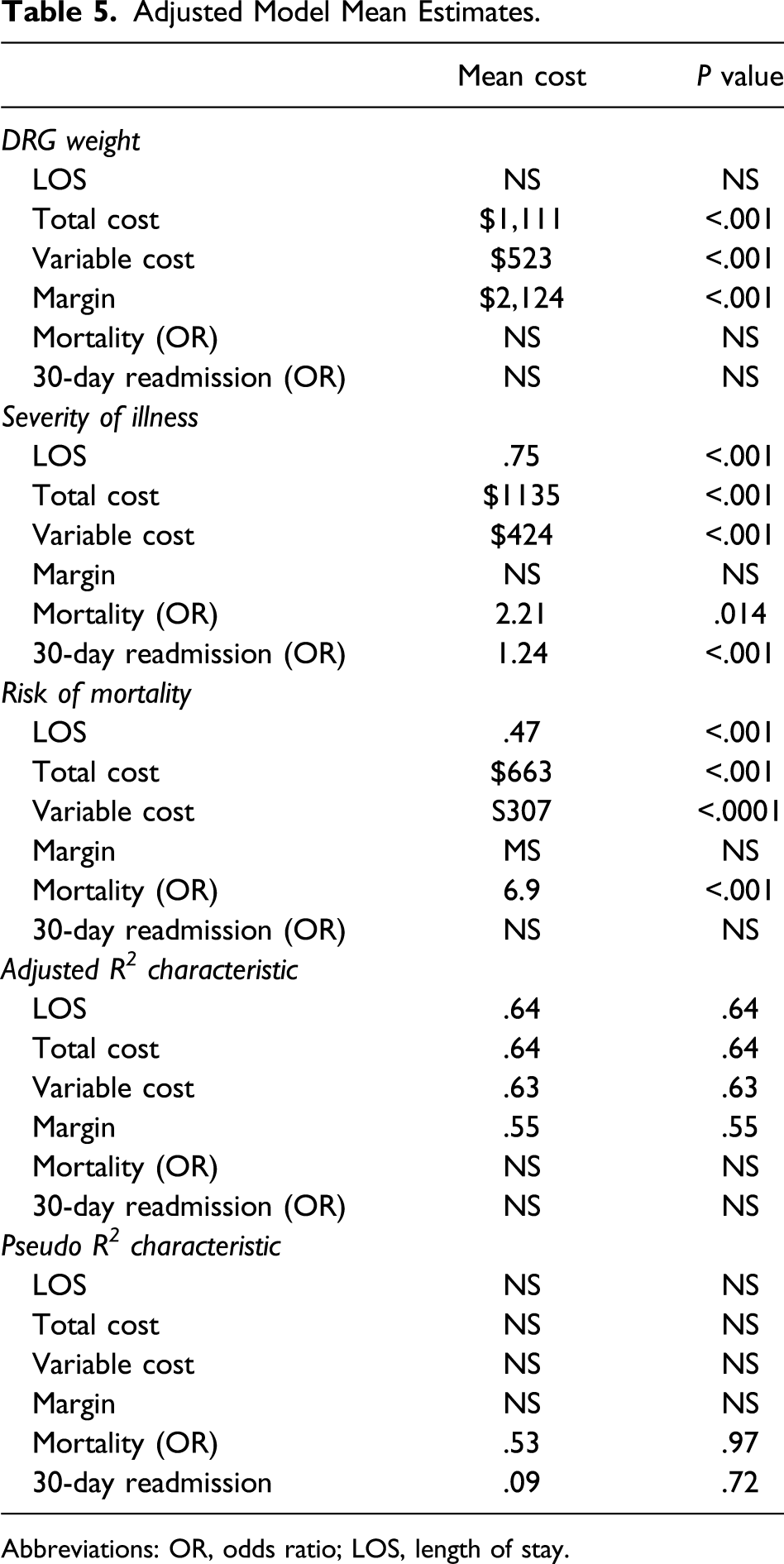
Abbreviations: OR, odds ratio; LOS, length of stay.
Discussion
The present study investigated the relationship between the number of consulting physicians involved in the care of surgical patients and its immediate implications on LOS, mortality, readmission rates, and health care costs. Surgical procedures that required hospitalization for at least one day were incorporated into our analysis. Surgeries examined were interventions frequently performed at both community and academic settings by general surgeons, although other complex surgical procedures such as pancreatic and hepatic resections were also analyzed. Financial variables assessed combined both fixed and variable costs as well as contribution margins per attending consultant. Our research showed that each consulting physician added to the care of an individual surgical patient negatively affected LOS, readmission rates, and in-hospital mortality. Health care costs were also increased with the mounting number of consultants with an average decline in contribution margins of $354 per patient/consultant, although this was more evident with self-paying patients. Even though our study was not designed to evaluate the usefulness and cost-effectiveness of dedicated hospitalist services, adding any type of consultant to the care of patients regardless of the specialty had negative implications on both clinical and financial variables in the present study.
Despite interhospital and geographical disparities in the use of hospitalist services 16 and health care resources 17 in the United States, over the last several years, the participation of general medicine practitioners in the management of surgical patients has risen exponentially.18,19 In one of the largest retrospective studies looking at the impact of co-management services on Medicare patients, Sharma demonstrated an 11% increase per year in the number of generalists involved in the care of surgical patients. 20 Elderly comorbid patients and those receiving care at midsize nonteaching institutions were more likely to have hospitalists involved in their care. General and orthopedic surgical services had the highest number of patients involved with co-management services, although analysis of the dataset was restricted to only 15 of the most common procedures performed on Medicare patients. Despite the lack of outcome data in this study, the authors advocated for training more general practitioners to satisfy the growing demand of hospitalist in the management of surgical patients. In this regard, studies have emphasized the need for curricular changes 21 and training of general medicine practitioners which incorporates conditions and procedures commonly needed in surgical patients. 22
Attributing improvements in clinical results by the addition of dedicated hospitalist services is a challenging task, as the majority of prior retrospective studies have not controlled for other variables affecting outcomes. 23 There are a few quasi-randomized controlled studies that have attempted to answer the question of whether these services truly improve postoperative care and if they are cost effective.3,24-26 Huddleston randomized 526 postoperative orthopedic patients who were at an elevated risk for perioperative complications to a team of a hospitalist plus an orthopedic surgeon or a team composed of an orthopedic surgeon and residents with an internist consulting on an as-needed basis. In this study, minor complications were lower in the hospitalist group, and LOS, after adjusting for discharge delays, was half a day shorter in the hospitalist-based team. Hospital and total costs were similar between groups, but the hospitalist group had higher physician-related expenses.
It is unclear from the available data how the addition of a hospitalist service impacts direct care costs. Some authors have shown benefit and significant reductions in total care costs with the addition of hospitalist services,27-29 but this have not been uniformly reported throughout the literature. 30 Theoretical financial advantages of having co-management services include decreasing postoperative complications rates, decreasing LOSs, and allowing surgeons to increase productivity by spending more time in the operating room. 4 A clear limitation that the majority of published studies have is that most authors have failed to differentiate costs associated with professional services provided by hospitalists vs. costs from additional resources utilized by hospitalists, making it difficult to truly estimate the added financial benefits of co-management services. Evidence-based rationalization of unnecessary testing and medications has the potential to improve some of the economic variables associated with the use of co-management services.31-33
Studies conducted addressing the role of dedicated hospitalist services have not specifically focused on the number of consultants involved in the care of patients. Although unique in such aspect, our study is limited by several factors inherent to the analyses of large retrospective databases. It is not clear from our research how many times a particular consultant was involved in the care of a particular patient nor how this affected the cost and clinical results. It is also difficult to establish if some of the clinical outcomes (for instance, LOS) were biased by uncontrollable elements such as bed availability at rehabilitation centers, social support at the time of discharge, and attending preference. Additionally, patients readmitted following discharge from our system to an alternative institution were not tracked in this study, and therefore, accuracy of readmission rates was dependent on whether the patient was included on the database used. Despite these unavoidable restrictions, the large number of patients analyzed and the wide spectrum of surgical interventions included here strengthen our findings.
In conclusion, this study has shown negative clinical and financial outcomes when multiple consulting physicians are involved in the care of surgical patients. Until dependable research becomes available, a surgeon should consider relinquishing the management of surgical patients to nonsurgical physicians under only exceptional circumstances. 34
Footnotes
Acknowledgment
The authors would like to thank Cathy Stankiewicz, R.N., Director of Clinical Quality at AdventHealth for her support with this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.