
Abstract
This historical retrospective explores the history of the gastric pyloroplasty through the lives of the 4 surgeons whose eponymous procedures have defined the operative management of pyloric strictures: Heineke, Mikulicz, Jaboulay, and Finney. Today’s gastrointestinal surgeons employ a combination of techniques that highlight the rich and colorful history of their field.
“Historical studies, always of interest, are profitable in proportion to the open-mindedness of the student.” - John M. T. Finney, 1 1929
Surgical approaches to gastric pathologies have a long, tumultuous, and storied history. The earliest descriptions of gastric surgery were approaches to gastrointestinal trauma. Notable physicians and surgeons Hippocrates, Galen, Fallopius, Ambrose Paré, and Guy de Chauliac described approaches to gastrointestinal trauma.1,2 However, the outcomes of these operations were, expectedly, poor. The first elective gastric operation in the modern surgical canon was performed in 1602 by Florian Mathis, who removed a knife from the stomach of a sword swallower in Prussia. 1 Advances in the understanding of gastric physiology in the early 19th century, including the studies of American surgeon William Beaumont and Nobel Prize–winning Russian physiologist Ivan Pavlov, 3 allowed for later advances in surgical management of gastric pathologies. The first gastric resection was performed by Jules-Émile Péan in 1879 for a large cancerous mass; this was followed by Ludwik Rydygier in 1880 and Theodor Billroth in 1881.1,2 Until the 1960s, the management of peptic ulcer disease was primarily surgical. However, prior to the advent of acid-reducing procedures by Latarjet, Wertheimer, and Dragstedt in the mid-20th century, 3 the primary management was the symptomatic control of gastric outlet obstructions cause by chronic, fibrosing strictures of the pylorus. In this historical retrospective, we trace the development of the gastric pyloroplasty through the 4 surgeons whose eponymous procedures have become the foundation of pyloroplasty surgery.
Heineke-Mikulicz Pyloroplasty: Walter Hermann von Heineke (1834-1901) and Johannes Mikulicz-Radecki (1850-1905)
The first surgical approaches to treating gastric outlet obstruction from peptic ulcerative disease in adults were independently described by Heineke in 1886
4
and Johannes Mikulicz-Radecki in 1887
5
. In the Heineke-Mikulicz procedure, a longitudinal, full-thickness incision centered over the pyloroduodenal channel is made, which is then closed transversely using interrupted sutures (Figure 1). This is the most commonly utilized pyloroplasty technique in the modern era. Walter Hermann von Heineke (1834-1901), Johannes Mikulicz-Radecki (1850-1905), and the Heineke-Mikulicz pyloroplasty.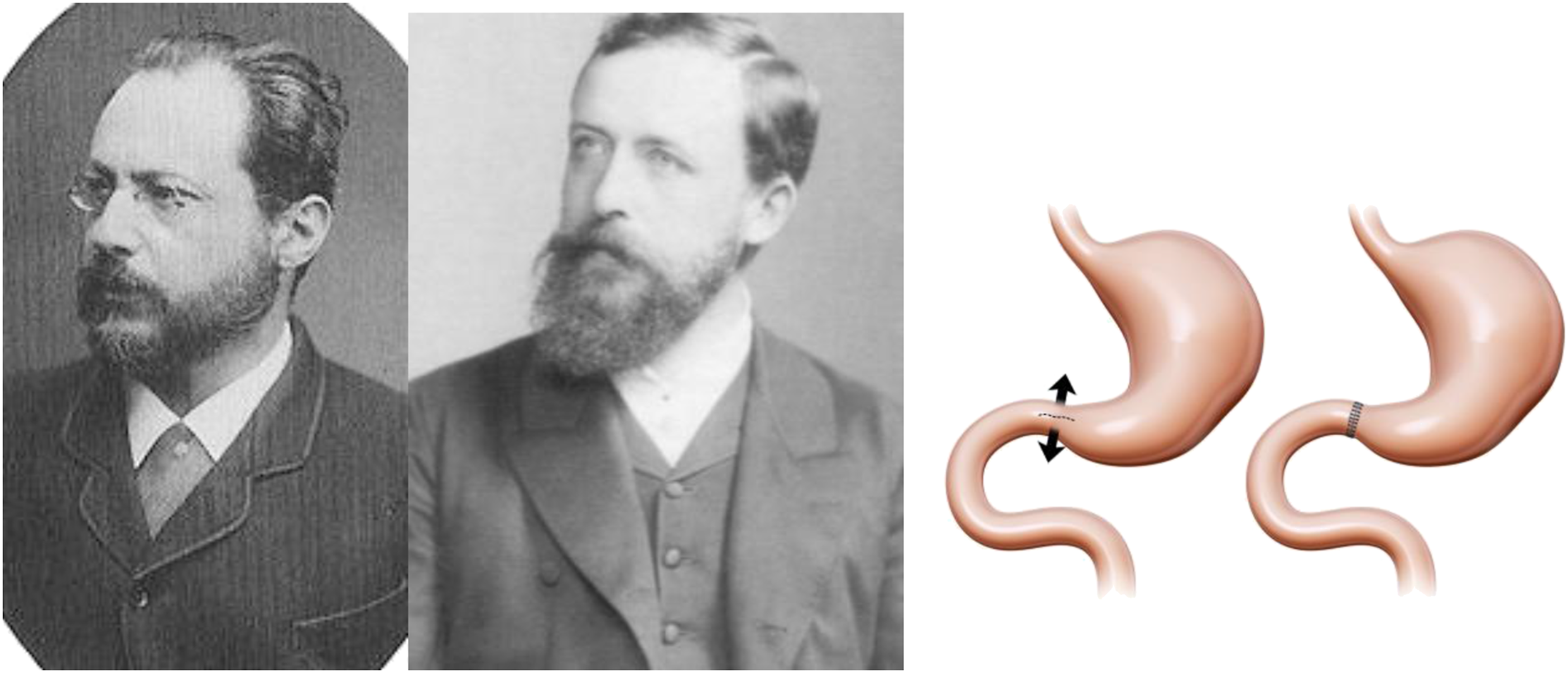
Walter Hermann von Heineke was born in Shönebeck, Prussia in 1834 and was the son of a physician. He completed his medical studies at the University of Greifswald in 1859. He began his surgical career as a member of the faculty at Greifswald, until ascending to Chair of Surgery at the University of Erlangen in 1867. 6 In addition to his pioneering work in gastric surgery, he described an early extraperitoneal approach to the resection of rectal cancer. 7 He served as the Chair at Erlangen until his death in 1901.
Johannes von Mikulicz-Radecki first performed his pyloroplasty procedure in 1887, a year after Heineke. Mikulicz was born in 1850 in Czerniowce, Austrian Empire, in 1850. He completed his medical degree at the University of Vienna in 1875, studying surgery under Theodor Billroth. 8 He joined Billroth’s surgical faculty from 1875-1880, 8 where he would develop the first esophagogastroscope (1881) in collaboration with optical engineer Josef Leiter.9-11 He then ascended to Chair of Surgery at Jagiellonian University in Krakow (1882-1887); in Krakow, he described the repair of a perforated peptic ulcer (1885) and first esophagectomy for esophageal cancer (1886).8,12 During his years in Krakow, Mikulicz was influenced by Joseph Lister’s principles of asepsis 13 and developed a passion for aseptic surgery. Opportunities to study asepsis would lead Mikulicz to become the Chair of Surgery at Konigsberg (1887-1890) before finishing his career as the Chair of Surgery in Breslau (1890-1905). 8 In Breslau, Mikulicz would construct the first aseptic operating room in the world. 12 Ironically, Mikulicz died of advanced gastric cancer in 1905. Among Mikulicz’s most famous pupils was Ferdinand Sauerbruch, who would become a renowned thoracic surgeon.
The early experience with the Heineke-Mikulicz pyloroplasty showed good results, though with some admitted technical limitations. William Mayo 14 reported his series of pyloroplasty using the Heineke-Mikulicz technique to the American Surgical Association in 1905, with a 0% mortality rate; however, one-third of his patients required a secondary operation. Mayo 14 credited this high rate of secondary operations due to the limited enlargement of the pylorus due to extensive adhesions and “degenerated muscle fibres […] incapable of the muscular effort.”
Jaboulay Gastroduodenostomy: Mathieu Jaboulay (1860-1913)
Mathieu Jaboulay was born in 1860 near Lyon, France. He completed his medical education in Lyon in 1884. 15 He joined the surgical faculty at Lyon and ascended to the Chair of Surgery at Lyon in 1892. Inspired by the 1894 assassination of French President Marie François Sadi Carnot, Jaboulay devised one of the earliest vascular anastomoses, using interrupted U-shaped sutures with intimal eversion. 16 His impact was felt throughout several fields in surgery, including suture-free intestinal anastomoses (“Jaboulay Button”), treatment of hydrocele (“Jaboulay’s Procedure”), and hemipelvectomy for cancer (“Jaboulay’s Amputation”). 15 He also pioneered xenotransplantation, using porcine and caprine kidneys to treat end-stage renal disease in 1906. 17 Jaboulay was unfortunately killed in a train derailment in 1913. Among Jaboulay’s most famous pupils were René Leriche and Alexis Carrell, both renowned vascular surgeons.
The Jaboulay gastroduodenostomy, first described in 1892
18
, includes separate longitudinal enterostomy incisions along the anterior surfaces of the stomach and duodenum, followed by side-to-side closure. The Jaboulay approach is perhaps best described as a pyloric bypass procedure, as it does not include a pyloric incision (Figure 2). Mathieu Jaboulay (1860-1913) and the Jaboulay gastroduodenostomy.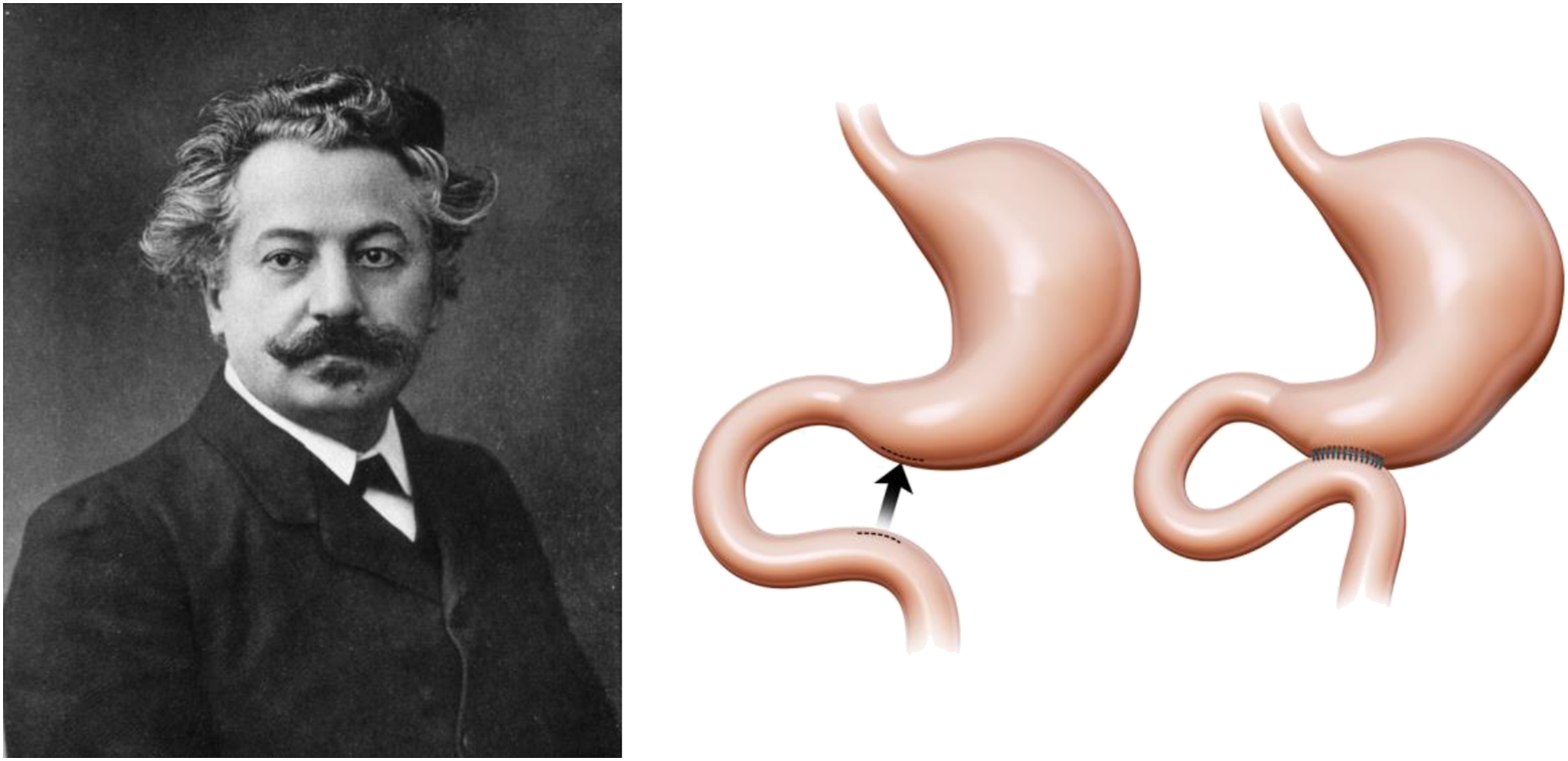
Interestingly, Jaboulay’s gastroduodenostomy procedure was not frequently used in the years following its publication. 19 In Jabolay’s initial article, as in subsequent descriptions on the Jaboulay gastroduodenostomy by his protégées Villard and Tixier,20,21 the authors allude to mobilizing the duodenum to bring it into contact with the stomach but do not provide any particular procedural details other than to say that it is technically easy. As duodenal mobilization is perhaps the critical portion for the success of the operation, the Jaboulay gastroduodenostomy was used infrequently until the later publication of duodenal mobilization techniques by Kocher. 19
Finney Pyloroplasty: John Miller Turpin Finney (1863-1942)
John M. T. Finney was born in 1863 in Natchez, MS, though his family relocated to Maryland following the tragic death of his mother.22,23 He completed his medical education at Harvard Medical School in 1888, followed by an internship at Massachusetts General Hospital. He joined the first resident house staff under William Halsted at Johns Hopkins Hospital in 1889,22,23 where he would spend the remainder of his career. He was a trusted colleague of Halsted and even performed an appendectomy on Halsted’s wife, Caroline Hampton Halsted. Finney was one of the founders of the American College of Surgeons, of which he served as the organization’s first president in 1913; he also served as president of the American Surgical Association in 1922.22,23 He was a Brigadier General during World War I and received numerous honors from both American and foreign armed forces. A notably humble man, Finney was nominated for the roles of Chair of Surgery at Hopkins and president of Princeton University, both of which he declined.22,23 He passed away in 1942, leaving a long legacy of American surgical excellence and a lasting impression on the Johns Hopkins surgical department.
Finney first presented the operation commonly known as the Finney pyloroplasty at the American Surgical Association in 1902.
24
Finney later described his procedure as “a natural development from the Jaboulay gastroduodenostomy.”
24
In the Finney approach, a longitudinal inverted U-shaped gastroduodenal incision is made along the greater curvature of the stomach and medial duodenal wall centered along the pylorus. The incision is then closed as a common gastroduodenal channel (Figure 3). Finney believed this was a superior approach to the Jaboulay for the ability to achieve “temporary abolition of the action of the pyloric sphincter” and “to excise ulcers on either the anterior or posterior wall of the duodenum, without materially altering the customary incision.”
24
In Finney’s 1929 presentation to the American Surgical Association in describing his 25-year experience in pyloroplasty, he reported a 5% mortality using his eponymous pyloroplasty against a 16.6% mortality using a Jaboulay gastroduodenostomy.
24
John Miller Turpin Finney (1863-1942) and the Finney pyloroplasty.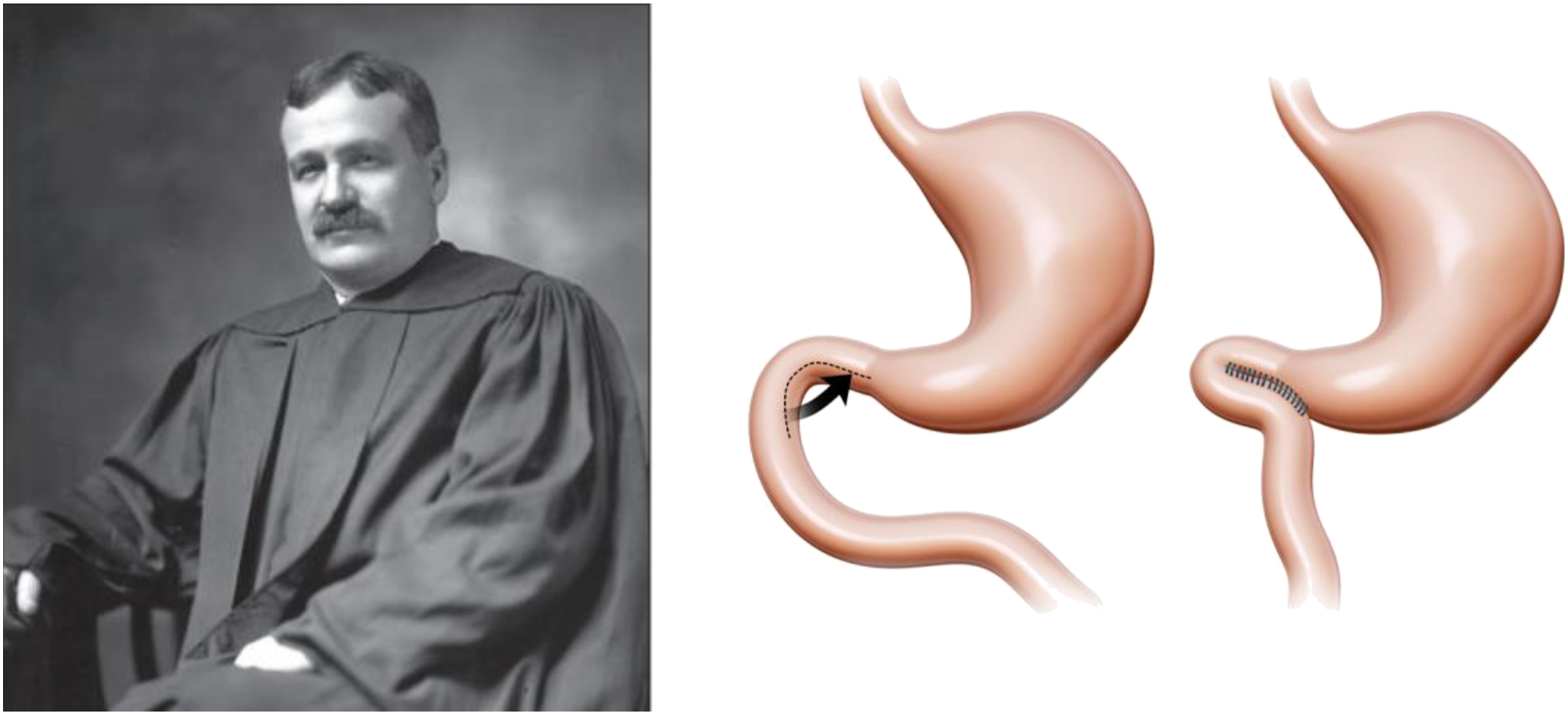
Conclusion
The history of the pyloroplasty operation includes the contributions of 4 notable surgeons, each of whom has left a remarkable legacy on the field of surgery beyond their contributions to pyloroplasty. The same operative techniques used in pyloroplasty have been extended to the surgical management other bowel strictures, including Crohn’s, radiation-induced enteritis, and post-necrotizing enterocolitis strictures. With the common similarities in surgical principles, these surgical legends with eponymous procedures developed techniques that ultimately could be applied more widely than their original intent. Today’s gastrointestinal surgeons employ a combination of techniques that highlight the rich and colorful history of their field.
Footnotes
Acknowledgments
The authors thank Andy Matlock MS, Carlos and Davis Center for Surgical Anatomy and Technique, Emory University School of Medicine for his contributions in medical illustration to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.