
Abstract

Trauma is a significant source of morbidity and mortality in the United States. Multiple organ failure (MOF) is a resource-intensive condition that is a significant cause of late death in trauma patients. 1 One common practice in the care of trauma patients is initial resuscitation with fluids and blood products to achieve hemostasis after the initial injury. 2 There are certain guiding principles in initial hemostatic resuscitation of trauma patients: high ratios of plasma and platelets to packed red blood cells (PRBCs), limitation of crystalloid fluids in initial hemostatic resuscitation, and permissive hypotensive resuscitation in some clinical scenarios. 2 There are a number of fluid and blood product (FBP) resuscitation practices in the initial-hemostatic resuscitation period in hospital care that are associated with increased rates of MOF in trauma patients, including increased administration of PRBC, fresh frozen plasma (FFP), and crystalloid fluids. 2
Despite the development of the guiding principles for initial resuscitation, 2 no recommendations exist regarding fluid administration in the period following the achievement of hemostasis, which has previously been defined as the post-hemostatic period. 2 This study examines the hypothesis that higher levels of fluids and blood products administered to trauma patients at high-risk of MOF over the first 72 hours of hospitalization are associated with higher rates of MOF.
A retrospective chart review was performed to evaluate the hypothesis in accordance with approval of the study protocol from the institutional review board at our institution. Patients were included in this study who were determined to be at high risk for the development of MOF and admitted to the trauma service between June 1st, 2015, and May 31st, 2018. To be eligible for this study, patients had to suffer a traumatic injury, be at least 18 years of age, have an injury severity score (ISS) of at least 9, receive at least one unit of PRBC within 4 hours of admission, and be admitted to the intensive care unit (ICU) for at least 72 hours. Patients were excluded if they had a head abbreviated injury score of 3 or greater at admission or suffered a burn injury.
Total liters of crystalloid and colloid fluids, as well as units of PRBC, platelets, fresh frozen plasma, and cryoprecipitate that were administered to patients were collected and organized into distinct time periods: 0-4 hours after admission, 4-24 hours after admission, 24-48 hours after admission, and 48-72 hours after admission. Sequential organ failure assessment (SOFA) scores were utilized to monitor for the development of MOF in this study. SOFA scores were calculated and categorized for each patient over each 24-hour period of their hospital stay. Linear regression models were performed to determine the association between each patient’s maximum SOFA score of their hospital stay and the amounts of fluids and blood products administered over the first 72 hours of their hospital stay.
Between June 1st, 2015, and May 31st, 2018, a cohort of 31 trauma patients at high risk for MOF were identified at our institution. 23 of 31 patients were men, and the median age was 46 years [IQR: 30-57.5]. Of note, all patients in this series sustained blunt trauma. The injuries were notably severe with a median ISS of 24. The majority of patients (28 of 31) survived to discharge.
Median Liters of Fluids and Units of Blood Products Administered.
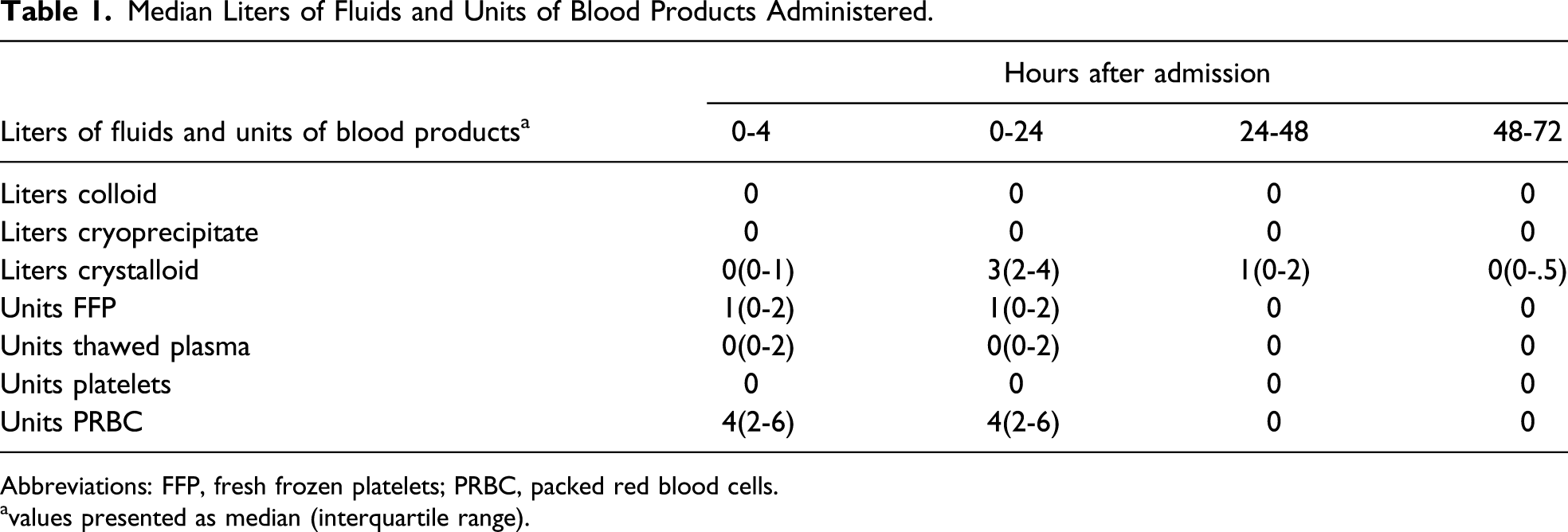
Abbreviations: FFP, fresh frozen platelets; PRBC, packed red blood cells.
values presented as median (interquartile range).
(Table 1) The majority of all fluids and blood products were given within 24 hours after admission. Crystalloid fluids represented the majority of fluids and blood products given from 24-72 hours after admission, accounting for the majority (51 of 70) of the total fluids and blood products given over this time period. Sufficient clinical data were available on 22 of 31 patients to calculate at least one SOFA score of patient hospital stay.
For each additional 1 unit of transfusion product, SOFA score is expected to change by .1219 (alternatively, SOFA will decrease by 87.8%; P = .333). For each additional 1 L of IV fluids administered, SOFA score will decrease by 65.7% (P = .0426). In a linear regression model that controlled for units of blood products transfused, total fluid volume was significantly associated with maximum SOFA score (P = .0426) with an R2 value of .219. When considered individually using Fisher’s exact test, neither the total transfusion units nor the total fluid volume were significantly associated with maximum SOFA score.
These results support the hypothesis that increased fluid administration over 72 hours after admission to a group of trauma patients at high risk for the development of MOF is associated with an increase in the development of MOF. While the sample size is small, the significance of this association suggests that FBP administration over the first 72 hours of hospital care has a strong relationship with MOF in the posthemostatic resuscitation period. Interestingly, the linear regression analysis found that neither number of blood products transfused, nor liters of fluid administered were significantly associated with maximum SOFA score, but that total fluid was associated with maximum SOFA score when controlling for the number of blood products administered. This result suggests that while initial hemostatic resuscitation with blood products confers a risk of MOF development, excess fluid administration may confer an increased risk of MOF development. Additionally, crystalloid fluids comprised most fluids and blood products administered to trauma patients between 24 and 72 hours after admission. These results, although novel for the time period examined, do share a similar trend with previous studies examining initial resuscitation in trauma patients with MOF development.2,3
A recent study has investigated fluid balance and outcomes in a population of critically ill patients, finding that a positive fluid balance on day 3 after ICU admission is associated with increased 30-day MOF development and 30-day mortality compared to a negative fluid balance 3 days after ICU admission. 4 While this study did not focus exclusively on trauma patients and measured deresuscitation measures and not solely on FBP administration, the overall concept that an increased fluid balance 3 days after ICU admission is associated with an increased risk of MOF is similar to these results.
There are important strengths and limitations with this study. Most notably, this represents the first study to examine FBP administration in trauma patients at high risk for subsequent MOF development in the post-hemostatic resuscitation period. In addition, statistically significant association of this trend in a sample of only 31 patients demonstrates just how important FBP administration in the post-hemostatic resuscitation period is to MOF development. The most important limitation with this study is the small sample of only 31 patients. Because of this, analysis of the hypothesis over specific 24-hour time intervals and further analysis of specific trends beyond the main objective were not possible. Future studies should be conducted to investigate this relationship in larger patient population with more statistical power to allow for analysis of FBP administration over specific time intervals to MOF development and consideration of other factors that could confound this association, further clarifying this complex clinical issue.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.