
Abstract
Background
Academic achievement is an integral part of the promotion process; however, there are no standardized metrics for faculty or leadership to reference in assessing this potential for promotion. The aim of this study was to identify metrics that correlate with academic rank in hepatopancreaticobiliary (HPB) surgeons.
Materials and Methods
Faculty was identified from 17 fellowship council accredited HPB surgery fellowships in the United States and Canada. The number of publications, citations, h-index values, and National Institutes of Health (NIH) funding for each faculty member was captured.
Results
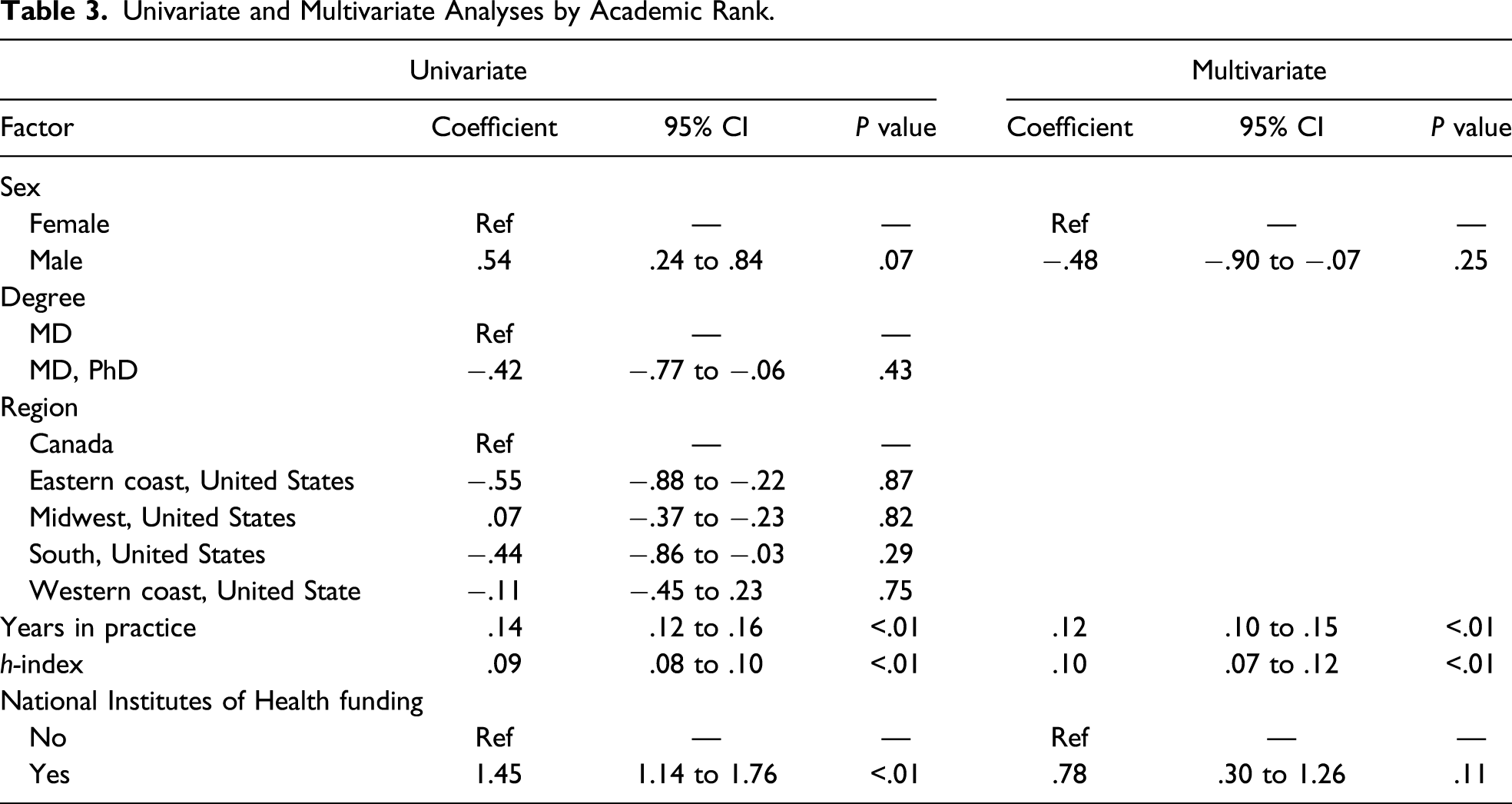
Of 111 surgeons identified, there were 31 (27%) assistant, 39 (35%) associate, and 41 (36%) full professors. On univariate analysis, years in practice, h-index, and a history of NIH funding were significantly associated with a surgeon’s academic rank (P < .05). Years in practice and h-index remained significant on multivariate analysis (P < .001).
Discussion
Academic productivity metrics including h-index and NIH funding are associated with promotion to the next academic rank.
Introduction
Hepatopancreaticobiliary (HPB) surgery is a highly nuanced and competitive subspecialty. A surgeon’s academic rank is a measure of success in the surgical field, yet there are no benchmarks standardized across institutions that are uniformly met prior to promotion or tenure. Academic surgeons are often involved in educational and clinical roles with expectations that they maintain both acceptable surgical volume, and regional or national reputation, all while demonstrating institutional leadership skills and academic scholarship.1-3 These factors are often considered by institutions when selecting candidates for promotion. 4-6 However, traditionally, academic achievement, including publications in high-impact journals and funding from sources such as the National Institutes of Health (NIH) or other large extramural sources, has been relied heavily upon as a measure of success in academic surgery.
Quantifying academic achievement merely on individual bibliometric measurements, such as the number of publications or citations, may not accurately reflect the researcher’s academic accomplishments. The total number of publications does not reflect their quality, and the total number of citations can falsely be elevated by a single publication of major impact. The Hirsch index (h-index), published by Hirsch et al, is an attempt to measure both the quality and quantity of a scientific output. 7 It is defined as the highest number of publications of a scientist that have been cited h times. For example, for a researcher to have an h-index of 12, they must have 12 publications with at least 12 citations each, while the remainder of his/her publications will have ≤12 citations. 7 The h-index is often used in medicine to evaluate academic productivity and is a better predictor of scientific achievement as compared to the number of citations or publications alone. In addition to determining individual scientific productivity, the h-index has been generalized to evaluate the collective academic prowess of entire surgical departments.8,9
Hepatopancreaticobiliary surgery, which earlier was often folded into the general surgery, transplant, or surgical oncology divisions of surgery departments, is now emerging as a unique specialty often gaining its own division within surgical departments. HPB surgeons in North America and Canada feed from 4 distinct training tracts or fellowships, namely hepatopancreaticobiliary surgery (HPB), surgical oncology, solid organ transplantation (transplant) and minimally invasive surgery (MIS). There have been some data published on objective benchmarks for academic promotion within surgical oncology and general surgery.9,10 However, there are no data looking at promotion within HPB surgery. This creates a challenge for junior HPB faculty seeking academic promotion. A challenge only made more complex as HPB surgeons come from different fellowship training backgrounds of various lengths with different emphasis placed and time dedicated to research. Therefore, we sought to quantify the metrics associated with increased academic rank in HPB faculty at institutions with Fellowship Council accredited HPB fellowship programs.
Materials and Methods
All data collection occurred between September 1, 2017 and September 14, 2017.
Faculty Selection
The 17 Fellowship Council accredited HPB surgery fellowships within the United States and Canada were identified from the Fellowship Council Web site (https://fellowshipcouncil.org). Individual faculty members were identified from Fellowship Council and departmental Web sites. Only surgeons trained through a general surgery residency pathway were included and individuals clearly identified as research-only faculty, without a clinical practice, were excluded. Surgeons were identified as assistant professors, associate professors, or professors. The surgeon’s index fellowship track (HPB, surgical oncology, MIS, or transplant) was identified. Surgeons without fellowship training were designated to a general surgery track.
Demographics and Bibliometrics
Gender, years in practice, and degree (MD, MD/PhD, MD/MPH, and MD/MBA) were recorded for each surgeon. Gender and degree were recorded from the institutional Web sites. The number of years in practice was calculated from the year of initial American Board of Surgery (ABS) certification obtained from the ABS Web site (http://www.absurgery.org) to the present year.
The Scopus database (http://www.scopus.com) was searched by the author name. Number of publications, citations, and h-index for individual faculty members were collected. If similar author names existed in the database, the author of interest’s current and previous affiliations were cross-referenced to ensure only the intended author’s information was collected.
NIH Funding
The NIH Reporter database (https://report.nih.gov/) was used to obtain grant funding information. The database was searched for all included faculty. Documentation of history of any NIH funding or current NIH funding was noted separately. The funding was counted only if the surgeon was listed as principal investigator of the award. All NIH-designated awards were included.
Statistical Analysis
Descriptive statistics were performed for the variables. A multivariate analysis was performed using an ordinal regression to analyze factors that contribute to academic rank. A value was considered significant when P < .05. All statistical analyses were performed with STATA 15 (StataCorp LLC, College Station, Texas).
Results
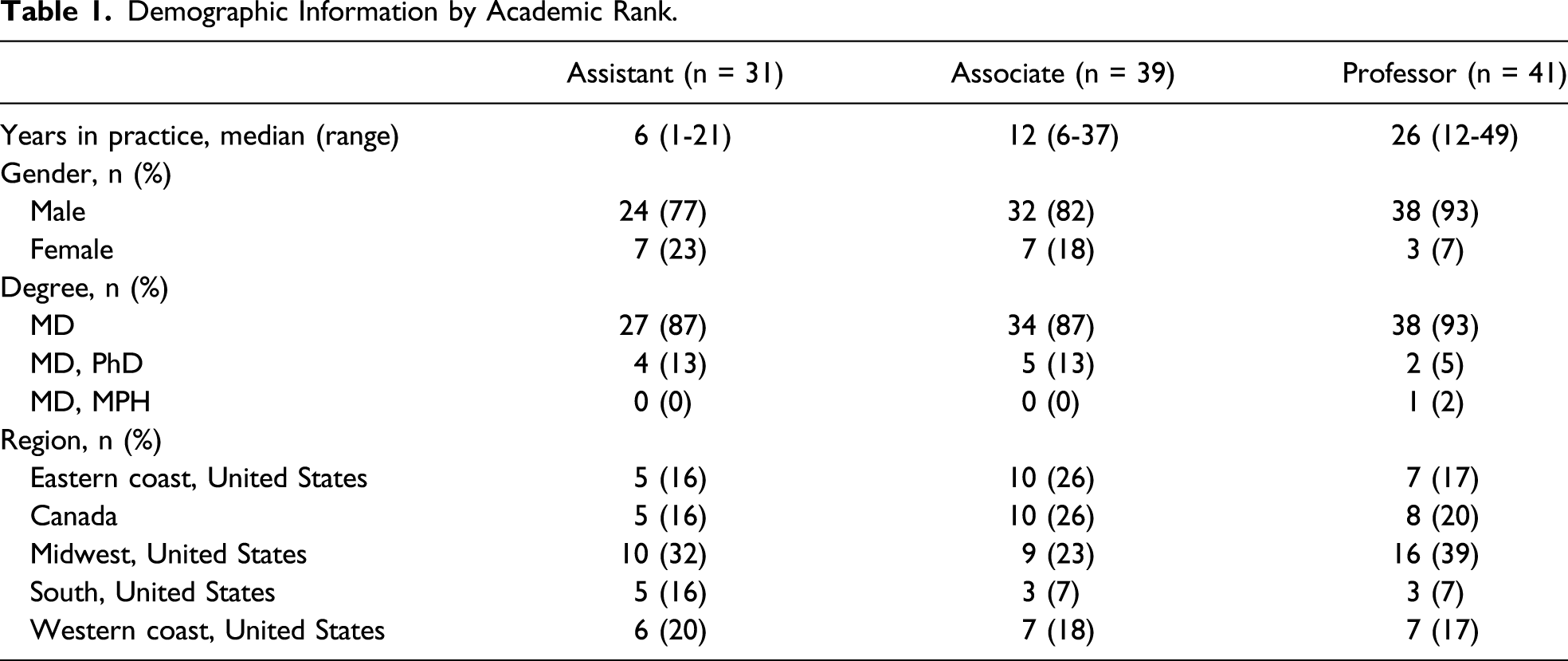
A total of 17 institutions were identified on the Fellowship Council Web site as accredited HPB fellowship programs. From these, 17 programs, 111 surgeons were identified on the individual institutional Web sites. Rank information was obtained for all 111 surgeons. Of these, 31 (27.9%) were listed as assistant professors, 39 (35.1%) associate professors, and 41 (36.9%) professors. Ninety-four of the 111 total faculties were men (85%). Of the full professors, only 7% were women as opposed to 23% at the level of assistant professor.
Demographic Information by Academic Rank.
Quantitative Bibliometric Data by Academic Rank.
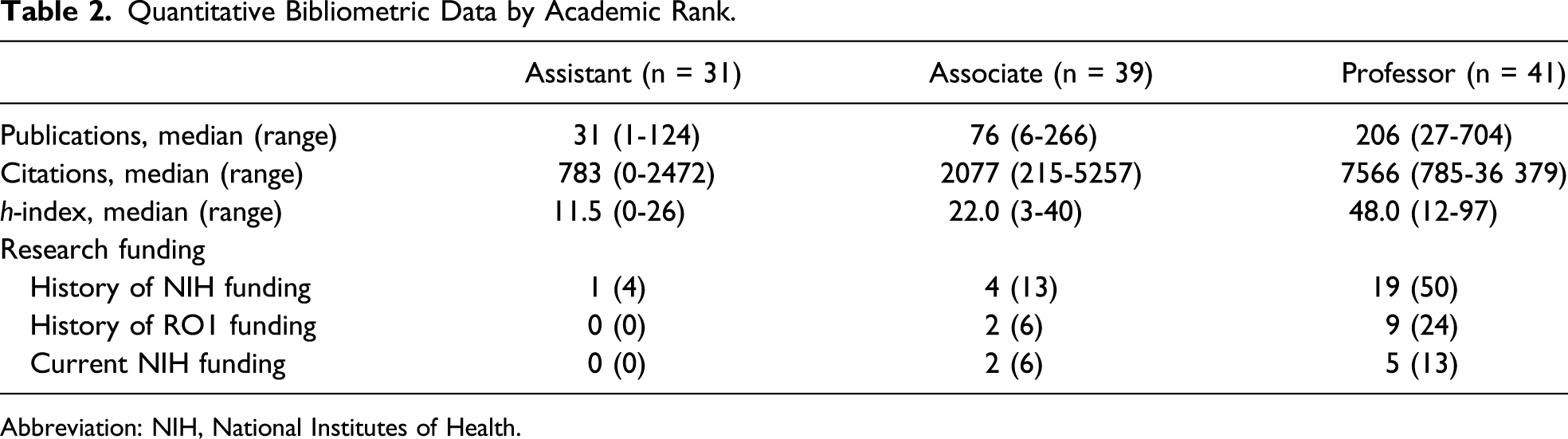
Abbreviation: NIH, National Institutes of Health.
Twenty-one percent of all surgeons had a history of NIH funding; however, only 6.3% were currently funded. Forty-six percent of those at the full professor rank had a history of NIH funding, while only 3.2% of assistant professors and 10.3% of associate professors had previous NIH funding.
Univariate and Multivariate Analyses by Academic Rank.
We also compared faculty based on their index fellowship training including surgical oncology, HPB, solid organ transplant, and MIS. The trend of increasing number of publications and citations with an increasing academic rank was maintained. Surgeons in the transplant and the surgical oncology group had a higher median number of publications than those who completed a HPB or MIS fellowship (87, 78, 67, and 68, respectively). The same trend was found for h-index. Surgeons who completed transplant and surgical oncology fellowships had a higher median h-index than those who completed HPB or MIS fellowships (26, 22, 19, and 18, respectively). Training in a specific fellowship track was not associated with an increase in academic rank (P = .319).
Discussion
Promotion to the next academic rank is a measure of success for academic HPB surgeons and is often linked to academic achievements such as publications and extramural funding. However, for young academic HPB surgeons, the promotion process is not uniform and there are little data regarding criteria needed for promotion. We sought to identify criteria associated with increased academic rank among HPB attending surgeons at hospitals with Fellowship Council approved HPB fellowships.
In our study, the number of publications, citations, and h-index increased proportionately with an increasing academic rank. Additionally, percentage of those with previous NIH funding also increased with rise in academic rank. Only 4% of assistant professors have a history of obtaining NIH funding, while 50% of full professors have had NIH funding at some point in their career. However, it must be noted that these data represent a snapshot in time and do not reflect the median values for h-index, number of publications, citations, or NIH funding at the precise time of promotion for each surgeon. These data are not easily captured, and we believe that using the median values for each rank provides valuable information regarding objective criteria for promotion as an HPB surgeon. In our data, the number of years in practice, NIH funding, and h-index were associated with academic rank. Certainly, the number of years in practice is not a metric that can be changed; however, attaining a median h-index of the next highest rank or securing NIH funding are metrics that could fuel promotions.
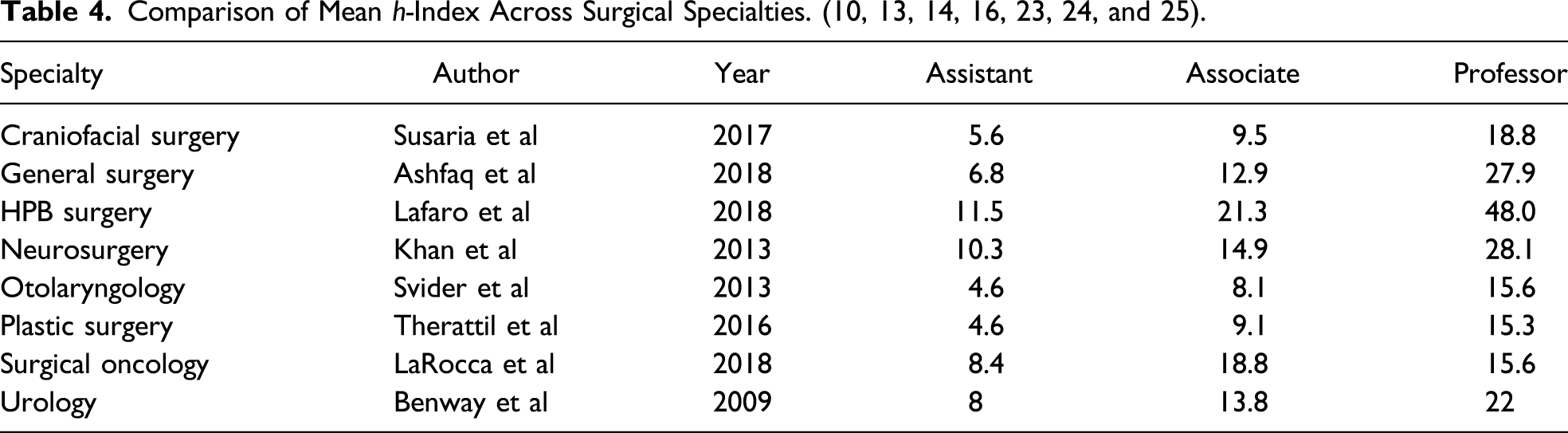
Multivariate analysis demonstrated that years in practice and h-index were the only factors significantly associated with academic rank. While years in practice are indicative of academic productivity, the h-index is the only quantifiable objective factor in our study of an increasing academic rank. The h-index has been associated with increased academic rank in other specialties including surgical oncology, plastic surgery, neurosurgery, urology, otolaryngology, and in general surgery as a whole. 9,11-16 However, the h-index is not without flaws. Surgeons who have been in training longer have a longer time interval to accumulate numbers of citations and publications. In addition, it does not take into account the order of authorship or type of publication. Authors get the same credit toward their h-index whether they are the first author or fifth. Lastly, self-citation has been postulated to affect one’s h-index; however, this has not born out to be true in studies.17,18 Lastly, we used the Scopus database to determine each surgeon’s h-index; however, there are other sources of computing the h-index including Google Scholar and Web of Science that might provide varied indices.
Comparison of Mean h-Index Across Surgical Specialties. (10, 13, 14, 16, 23, 24, and 25).
There has been a concern about a wide gender disparity in medicine and specifically in surgery. Our study also demonstrated a gender disparity amongst HPB surgeons. At the assistant professor and the associate professor rank, only 23% and 18% were female, respectively. At the professor level, only 7% of professors are women. While gender was not significant in either our univariate or multivariate analyses, the numbers are alarming. Previous studies have identified gender-based trends and barriers to careers in academic surgery.21,22 However, additional research is needed to determine factors that may mitigate gender disparities in the recruitment and promotion of academic surgeons.
Median h-Index by Academic Rank and Fellowship Training.
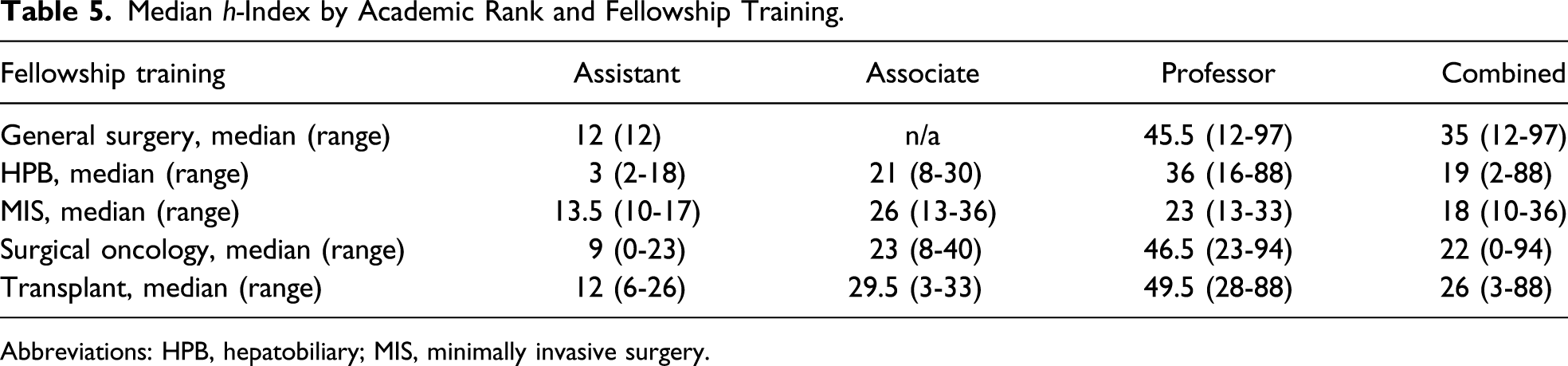
Abbreviations: HPB, hepatobiliary; MIS, minimally invasive surgery.
The data herein are dependent on the institutions and their Web sites. Some institutions may update them at different time intervals which could potentially make some of the data inaccurate. It also does not inform how long it took for each faculty to reach the next level of promotion. We have tried to reduce this bias by including data from all faculties within a specified time period. Lastly, this was a database of academic HPB surgeons involved with HPB fellowships. Academic HPB surgeons who may be faculty of other fellowships or surgical residencies are not represented in the study.
HPB is a unique specialty in that there are multiple fellowship tracks which enable surgeons to practice in the field, and the ideal track of training has been an issue of intense discussion and debate. While the discussion has mainly focused on the content and philosophy of training, whether a specific training track contributes more to academic productivity and rank has not been studied. This is the first study that analyzes the factors predictive of academic rank amongst those that identify HPB surgeons and are training future HPB surgeons.
In conclusion, academic rank amongst HPB surgeons is related to the number of years in practice and their h-indices. Specific fellowship training did not predict a higher academic rank amongst HPB surgeons. These objective measures may help to provide some insight and clarity for this promotion process. Studies of all academic HPB surgeons may help elucidate the effect of these factors more effectively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under award number NIH 5K12CA001727‐20.