
Abstract

A 74-year-old female Jehovah’s Witness with a history of type 2 diabetes mellitus and gastroesophageal reflux disease presented to the emergency department with acute-on-chronic right upper quadrant abdominal pain and a 2-week history of jaundice and pruritis. Her surgical history was notable for an open cholecystectomy 34 years prior to presentation. She was afebrile and normotensive. Laboratory studies demonstrated a total bilirubin of 2.5, direct bilirubin of 1.8, alanine aminotransferase level of 139, aspartate aminotransferase level of 127, and alkaline phosphatase of 273. Her electrolytes and white blood cell count were within normal limits, and her hemoglobin level was 12. A computed tomography (CT) scan demonstrated a cystic structure of the porta hepatis and marked intrahepatic ductal dilation, concerning for a choledochal cyst. A magnetic resonance cholangiopancreatography (MRCP) was obtained for further evaluation and again demonstrated a large cyst (4.8 × 4.1 × 3.2 cm) of the porta hepatis thought to represent a hepatic cyst with mass effect on the common bile duct versus a choledochal cyst (Figure 1). Magnetic resonance cholangiopancreatography demonstrating large cyst of the porta hepatis with associated intrahepatic biliary ductal dilation.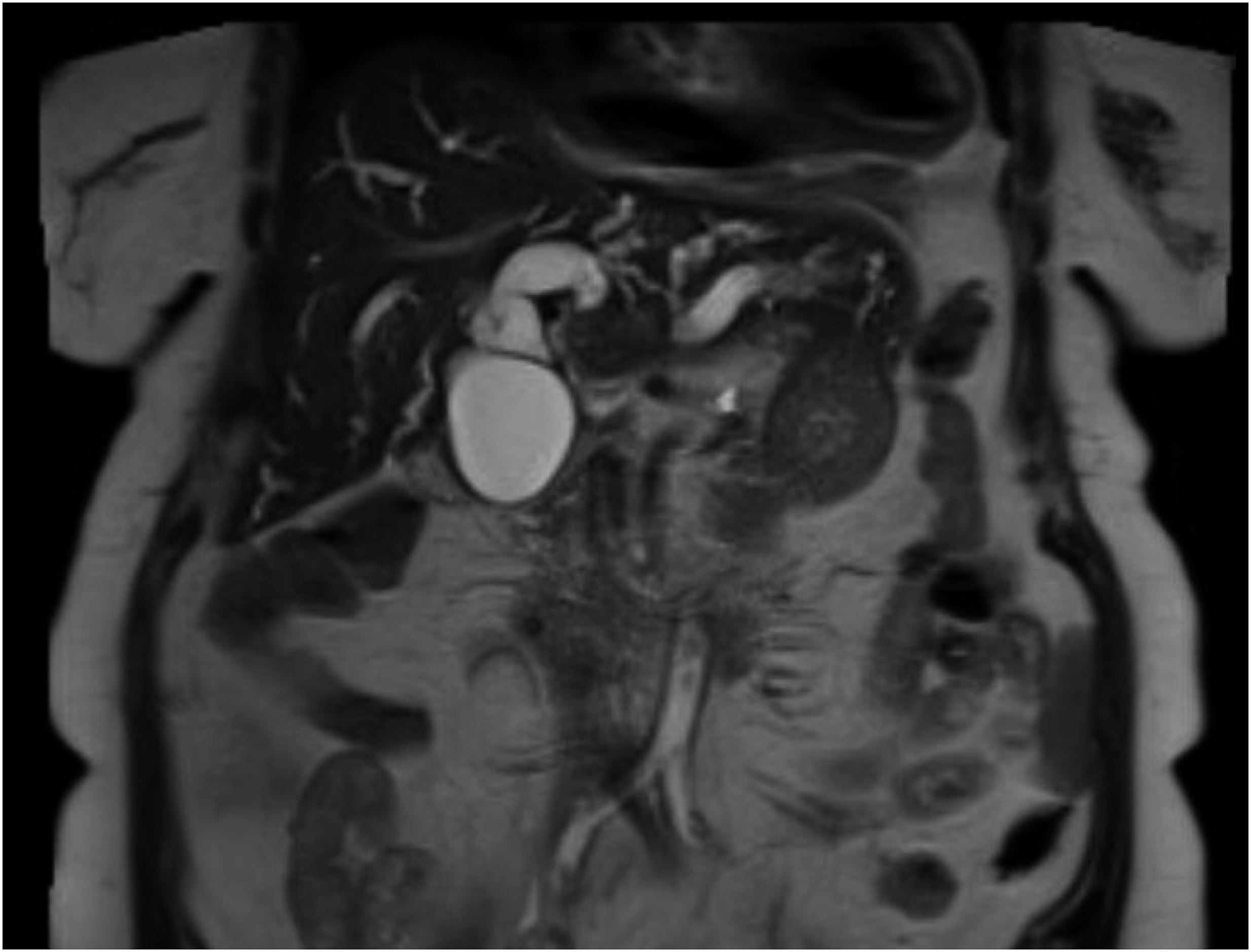
Given the likely longstanding nature of her biliary obstruction based on her imaging and the chronicity of her symptoms, as well as given concern for possible choledochal cyst, a decision was made to proceed to the operative room for an exploratory laparotomy and possible Roux-en-Y hepaticojejunostomy. An endoscopic retrograde cholangiopancreatography was not obtained preoperatively as it was unlikely to change management and risked contamination of the biliary tree. Considering patient’s Jehovah’s Witness status and the potential for blood loss in a reoperative vascular field, the hematology service was consulted and recommended darbepoetin-alfa and IV iron sucrose preoperatively to stimulate her bone marrow to increase red blood cell production at the time of surgery. Upon exploration of the abdomen via a midline laparotomy, the bile duct was noted to be dilated proximally and of normal caliber distally. The distal common bile duct was opened revealing a large cystic structure (Figure 2) within the duct. The cyst did not communicate with the bile duct lumen, thus ruling out a choledochal cyst. Given the imaging and intraoperative findings suggestive of a benign cyst, the cyst was fenestrated and the cyst fluid was found to be clear. The cyst wall was sent to pathology which confirmed the diagnosis of a benign biliary cyst. The bile duct was repaired over a 12 French T-tube, and a large round drain was left in the right upper quadrant. On postoperative day 3, her T-tube was clamped given that the output from her right upper quadrant remained serosanguinous. Her drain was subsequently removed 2 days later, and her T-tube was left clamped for 3 weeks. A follow-up cholangiogram via her T-tube demonstrated no evidence of leak or obstruction and the T-tube was subsequently removed. Her symptoms improved and her recovery was uneventful. Benign cyst within the common hepatic duct (grasped with forceps).
While several cases of intrahepatic peribiliary cysts have been described, solitary simple cysts of the extrahepatic biliary tree are extremely rare. Features include a unilocular cyst lined by a single layer of columnar or cuboidal epithelium and no communication between the lumen of the bile duct and the cyst.1,2 While these are benign lesions, they may require surgical intervention if symptomatic and/or indistinguishable from choledochal cysts which can potentially harbor malignancy. Cystectomy or cyst fenestration is the treatment of choice if the cyst is solitary.3,4 The etiology of this patient’s cyst remains unclear but may be related to chronic inflammation of her peribiliary glands after her prior open cholecystectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.