
Abstract
Introduction
Timing to start of chemoprophylaxis for venous thromboembolism (VTE) in patients with traumatic brain injury (TBI) remains controversial. We hypothesize that early administration is not associated with increased intracranial hemorrhage.
Methods
A retrospective study of adult patients with TBI following blunt injury was performed. Patients with penetrating brain injury, any moderate/severe organ injury other than the brain, need for craniotomy/craniectomy, death within 24 hours of admission, or progression of bleed on 6 hour follow-up head computed tomography scan were excluded. Patients were divided into early (≤24 hours) and late (>24 hours) cohorts based on time to initiation of chemoprophylaxis. Progression of bleed was the primary outcome.
Results
264 patients were enrolled, 40% of whom were in the early cohort. The average time to VTE prophylaxis initiation was 17 hours and 47 hours in the early and late groups, respectively (P < .0001). There was no difference in progression of bleed (5.6% vs. 7%, P = .67), craniectomy/-craniotomy rate (1.9% vs. 2.5%, P = .81), or VTE rate (0% vs. 2.5%, P = .1).
Conclusion
Early chemoprophylaxis is not associated with progression of hemorrhage or need for neurosurgical intervention in patients with TBI and a stable head CT 7 hours following injury.
Introduction
Among all injured patients, the prevalence of traumatic brain injury (TBI) is approximately 20%. 1 Patients with TBI have a 20-55% incidence of developing venous thromboembolic disease (VTE), which consists of both deep venous thrombosis (DVT) and pulmonary embolism (PE).2-5 Lack of mobility and delay to administration of pharmacologic prophylaxis against VTE contribute to this high incidence, with time to initiation of pharmacologic prophylaxis being the most readily modifiable risk factor. The Brain Trauma Foundation recommends lower extremity intermittent pneumatic compression stockings for VTE prophylaxis in patients with TBI, although it acknowledges that pharmacologic prophylaxis should be considered in patients with stable intracranial hemorrhage. 6 Despite this, there is no standard of care regarding time to start of pharmacologic prophylaxis in this population due to concern regarding the potential for harm related to increase in the size of the intracranial hemorrhage.
There is wide variability in practice regarding timing to start of pharmacologic VTE prophylaxis in patients with TBI. A recent national survey among members of The Eastern Association for the Surgery of Trauma showed that 50% of respondents consider their practice on VTE chemoprophylaxis in patients with TBI to be too conservative and 52% of report having no standardized protocols. 7 A near 50% difference in practice naturally lends itself to study.
The aim of this study is to evaluate the safety of a strategy for early initiation of VTE chemoprophylaxis in brain injured patients. We hypothesize that early administration, defined as within 24 hours following injury, is not associated with an increased risk of worsening intracranial bleed.
Methods
After obtaining approval from each institution’s research board, a retrospective cohort study was performed at 2 level 1 trauma centers from 2014-2016. We included all patients of 18 years of age or older with blunt TBI and head abbreviated injury score (AIS) >1 who received VTE chemoprophylaxis with low molecular weight heparin (LMWH) or unfractionated heparin (UFH) during their admission. Exclusion criteria included penetrating brain injury, any organ system other than the head with AIS ≥2, need for craniotomy/craniectomy within 24 hours of admission, progression of bleed on head CT scan performed within 6 hours after initial imaging, and death within the first 24 hours of admission. Patients with head AIS score of 1 were excluded in order to concentrate the study group to patients where there is controversy regarding timing for start of pharmacologic prophylaxis. Patients with any organ system AIS ≥2 were excluded to remove other considerations regarding the start of pharmacologic prophylaxis. Patients were divided into early (≤24 hours) and late (>24 hours) cohorts based on time to administration of the first dose of VTE chemoprophylaxis measured from time to arrival to the hospital.
All patients underwent hourly neurological exams, including intubated patients. If the neurological exam differed, patients underwent emergency head CT scan. If it did not, they were to undergo CT scan at 6 hours following admission. All patients had sequential compression devices ordered. Both UFH and LMWH were administered subcutaneously at fixed doses, regardless of body habitus, and neither anti-Xa levels nor partial thromboplastin time were checked. Unfractionated heparin (UFH) was given at 5000 units 3 times per day, and LMWH was given at 30 mg twice per day. Chemoprophylaxis was not to be given to patients who had an international standardized ratio (INR) greater than 1.5. No patients received tranexamic acid.
Demographic variables including age, head AIS, injury severity score (ISS), initial Glasgow coma score (GCS), and type of chemoprophylaxis given were collected. The primary outcome was progression of head bleed, which was determined based on interpretation of the attending radiologist’s report of the follow-up head CT scan found. If multiple sites of intracranial bleeding were present, an increase in any single bleed was considered a progression. Secondary outcomes included need for craniectomy/craniotomy after VTE start of chemoprophylaxis, in-hospital mortality, VTE events, total number of head CT scans obtained, intensive care unit (ICU) length of stay, and disposition destination. There was no routine surveillance for VTE carried out in either cohort. Deep venous thrombosis (DVT) was diagnosed using ultrasound and PE was diagnosed using CT angiography in symptomatic patients.
Univariate analyses between time to VTE chemoprophylaxis and demographics of interest were performed using chi-square tests, Fisher’s exact test, independent sample t-tests, and the Kruskal-Wallis test where appropriate. Variables with a corresponding univariate test P-value < .1 were adjusted for as potential confounders and entered into multivariate regression models to examine the independent relationship between time to VTE chemoprophylaxis and outcomes of interest. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, North Carolina) with P-value < .05 considered statistically significant.
Results
Overall Patient Demographics.
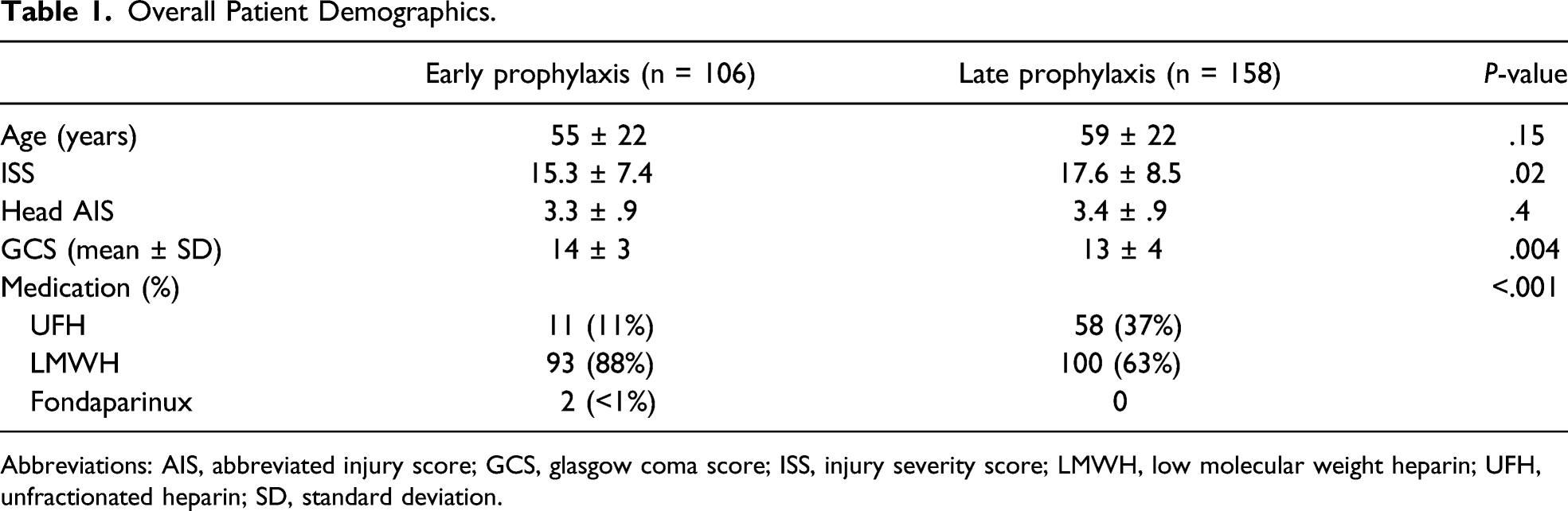
Abbreviations: AIS, abbreviated injury score; GCS, glasgow coma score; ISS, injury severity score; LMWH, low molecular weight heparin; UFH, unfractionated heparin; SD, standard deviation.
Univariate Outcomes in the Overall Cohort.
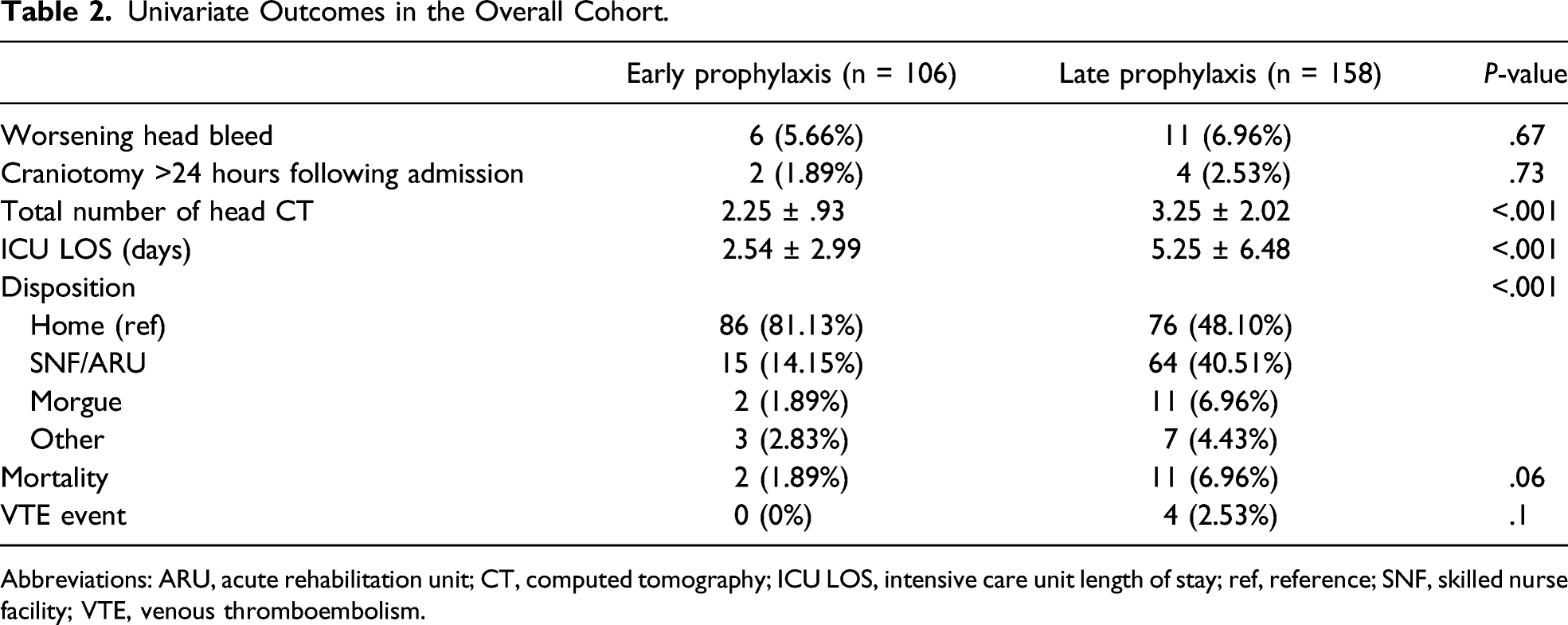
Abbreviations: ARU, acute rehabilitation unit; CT, computed tomography; ICU LOS, intensive care unit length of stay; ref, reference; SNF, skilled nurse facility; VTE, venous thromboembolism.
Between early and late prophylaxis groups, respectively, use of anticoagulants (24.5% vs. 27.8%, P = .55), DOACs (5.7% vs. 10.1%, P = .20), and antiplatelet meds (14.2% vs. 15.8%, P = .71) did not vary significantly. Furthermore, total use of anticoagulants was not associated with worsening head bleed (P = .25), need for craniotomy (P = .58), total number of head CTs (P = .77), intensive care unit length of stay (ICU LOS) (P = .34), mortality (P = .77), or VTE events (P = .58). We then looked into use of individual classes of anticoagulants. Use of direct oral anticoagulants (DOAC) was not associated with worsening head bleed (P = .64), need for craniotomy (P = .41), total number of head CTs (P = .36), ICU LOS (P = .37), mortality (P = .93), or VTE events (P = .54). Similarly, use of antiplatelet medications was not associated with worsening head bleed (P = .48), need for craniotomy (P = .92), total number of head CTs (P = .51), ICU LOS (P = .41), mortality (P = .70), or VTE events (P = .39).
Patient Demographics Based on Hemorrhage Type Within Each Cohort.
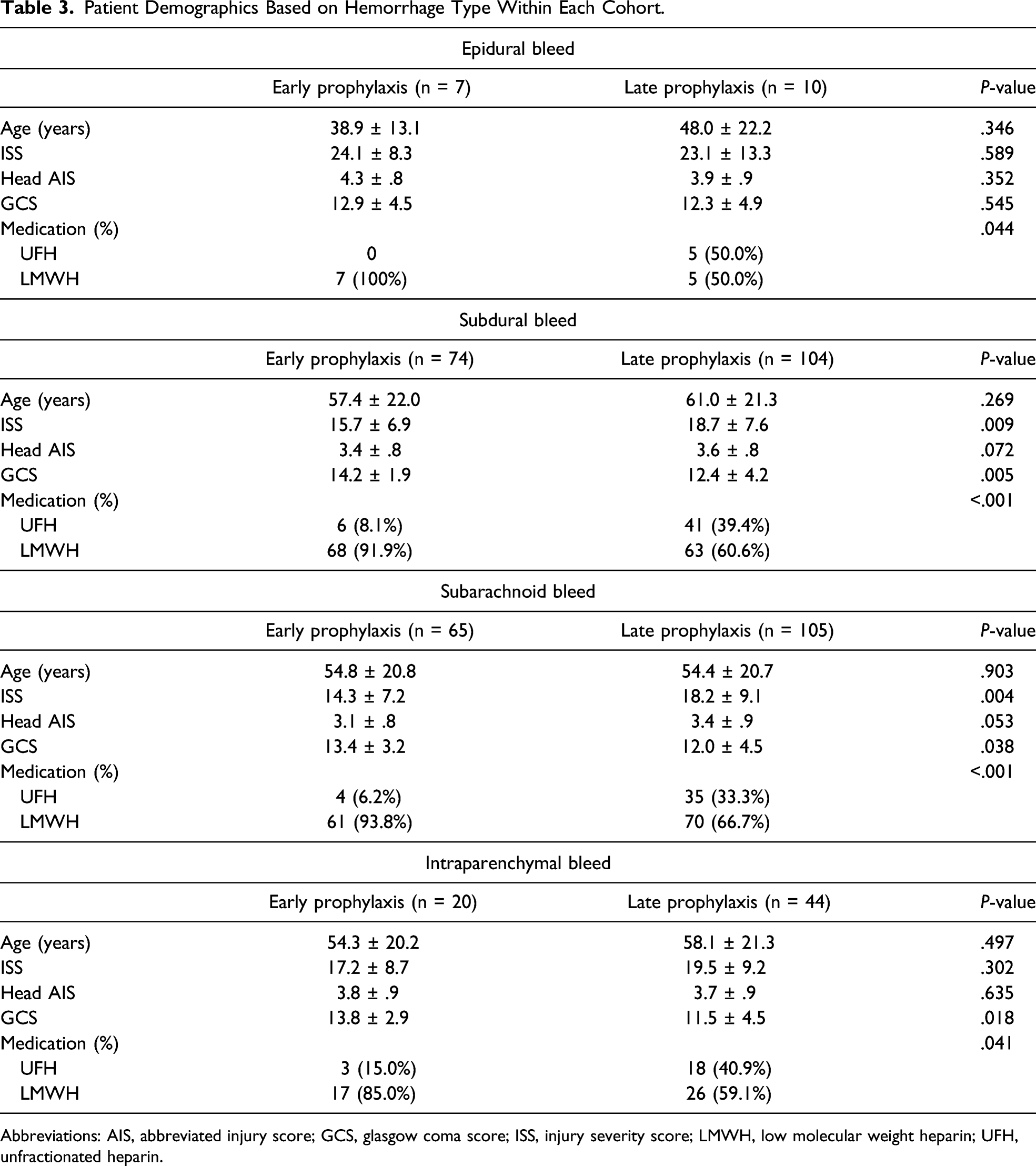
Abbreviations: AIS, abbreviated injury score; GCS, glasgow coma score; ISS, injury severity score; LMWH, low molecular weight heparin; UFH, unfractionated heparin.
Univariate Outcomes Based on Hemorrhage Type Within Each Cohort.
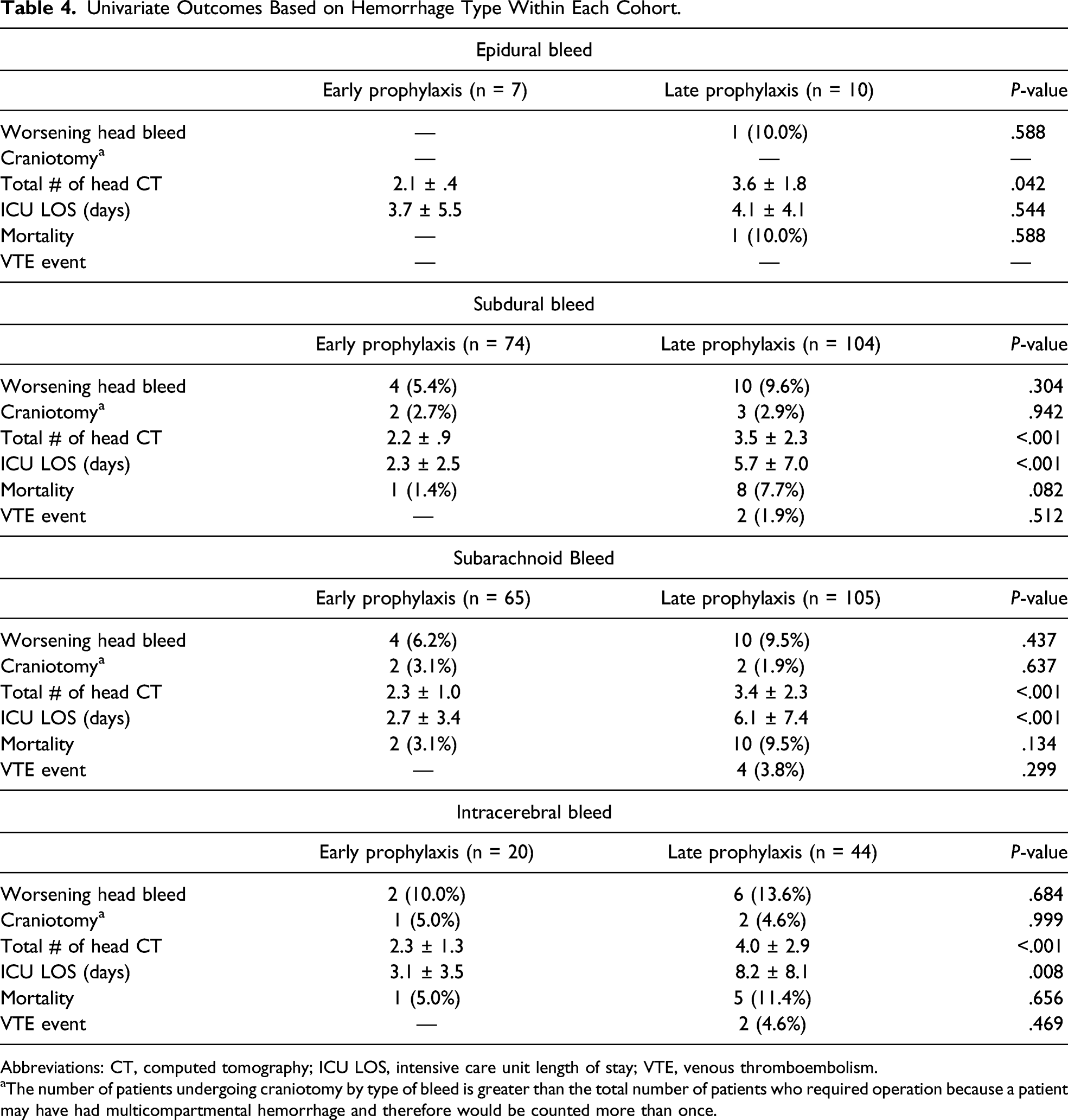
Abbreviations: CT, computed tomography; ICU LOS, intensive care unit length of stay; VTE, venous thromboembolism.
aThe number of patients undergoing craniotomy by type of bleed is greater than the total number of patients who required operation because a patient may have had multicompartmental hemorrhage and therefore would be counted more than once.
Discussion
In the current study, we found that early chemoprophylaxis is not associated with progression of intracranial hemorrhage or need for neurosurgical intervention in patients with blunt force TBI and a stable head CT 6 hours following injury. In addition, there was a trend toward fewer VTE events in patients started on chemical prophylaxis within 24 hours than those with more delayed initiation. The results did not change when patients were evaluated based on the nature of the intracranial hemorrhage within each VTE chemoprophylaxis timing cohort.
Use of chemoprophylaxis is the mainstay therapy for the prevention of VTE. However, its possible association with bleeding is of paramount concern. Levy et al. demonstrated that chemoprophylaxis in patients with TBI who had worsened findings on 24 hour follow-up head CT scan was associated with a 13-fold increase risk of rebleeding. 8 Because of these concerns, the ideal chemoprophylactic agent and timing to start VTE prophylaxis administration in patients with TBI remain controversial and there is no standard practice.
It has been shown that initiation of chemoprophylaxis within 72 hours of TBI lowers the incidence of VTE without an increased bleeding risk.9-11 A recent meta-analysis corroborated this finding in instances where there is no evidence of hemorrhage progression at 24 hours. 12 Other studies, albeit small and lacking generalizability, have reported no new or worsening intracranial hemorrhage in TBI patients if chemoprophylaxis is started as early as 48 hours after admission.8,9,13-18 Our study is the only one to date that evaluates outcomes based on 7 hour follow-up CT scan and initiation of chemoprophylaxis within 24 hours of injury. It adds to the body of evidence in this area by demonstrating that chemoprophylaxis can be safely started less than 24 hours following injury.
We did not obtain a surveillance CT scan to objectively measure the impact that start of VTE chemoprophylaxis might have had on the degree of intracranial hemorrhage. Rather, we utilized the need for further intervention, specifically craniotomy/craniectomy, and length of stay as surrogate markers for worsened outcome between the groups. Although this may be a less sensitive method for detecting adverse events, it is more generalizable and consistent with common practice, where decisions regarding medication administration, need for medical/surgical intervention, and readiness for discharge are made using clinical criteria rather than surveillance imaging.
We also found a greater number of VTE events in the late prophylaxis group, although the study was not powered to detect such a difference. If accurate, our results are consistent with the prior literature, where early initiation of VTE prophylaxis was associated with a decreased risk of VTE events without an increase in need for neurosurgical intervention or mortality. 19 As with follow-up head CT, patients did not undergo screening ultrasound to detect asymptomatic DVT. Thus, the VTE events noted were diagnosed clinically and confirmed radiographically. Most commonly, DVT was suspected if new onset, unilateral limb edema was noted. Pulmonary embolism (PE) was suspected if the patient developed a resting tachycardia or tachypnea, new oxygen requirement, and reported shortness of breath. Together with the finding that early initiation of chemoprophylaxis is not associated with worsening hemorrhage, this suggests that early initiation of chemoprophylaxis in this cohort may optimize overall patient safety.
Our work differs from and adds to previous reports in important ways. For example, in the recent study by Frisoli, 14 the investigators did not mention time to prophylaxis administration and also did not use follow-up head CT as a means to identify patients who may be safe for early VTE chemoprophylaxis. Our study reported the time to start of VTE prophylaxis as well as time to follow-up head CT scan, which addresses the limitations of the Frisoli study. As such, although some centers start to routinely utilize early chemoprophylaxis in patients with TBI, the current study serves as a validation of the safety of this practice, particularly for centers that do not routinely adhere to an early prophylaxis strategy.
This study has limitations that we acknowledge. First, it is retrospective in nature with all of the inherent limitations therein. Because there was no protocol governing treatment, the decision to use LMWH or UFH was up to the individual physician. Individual provider bias with respect to when to start chemoprophylaxis and which agent to use may have biased our results. We were not able to determine which patients had a history of VTE. Because imaging was ordered only as clinically indicated (ie, no surveillance imaging was performed), it is possible that the incidence of asymptomatic DVT differed between the cohorts. However, the clinical utility of such a finding remains controversial. There were statistically significant differences between the early and late prophylaxis groups with respect to ISS and GCS, although the differences may not be clinically significant. Head AIS scores were similar between groups, and we attempted to control for ISS and GCS in our multivariable logistic regression model. Although this is the largest study to date evaluating the safety of initiation of chemoprophylaxis within the first 24 hours of admission following brain injury, the sample size is small. The results of this study are only applicable to patients with radiographically stable brain injury as defined in the inclusion and exclusion criteria because we excluded patients who required operative intervention or demonstrated expansion of their intracranial bleed. Also, the study was not designed or powered to measure whether or not earlier initiation of VTE chemoprophylaxis is associated with a decrease in VTE events. Thus, whereas our study found that this practice is safe in this cohort, future studies are needed to demonstrate benefit. Finally, despite ordering sequential compression devices for all patients, there is no way to know how many patients applied them correctly.
Conclusion
Initiation of VTE chemoprophylaxis within 24 hours of admission in patients with TBI is safe in those without progression of bleed on repeat imaging 7 hours following arrival. Future, appropriately powered, prospective studies are needed to validate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.