
Abstract
Background
Geriatric burn trauma patients (age ≥65 years) have a 5-fold higher mortality rate than younger adults. With the population of the US aging, the number of elderly burn and trauma patients is expected to increase. A past study using the National Burn Repository revealed a linear increase in mortality for those >65 years old. We hypothesized that octogenarians with burn and trauma injuries would have a higher rate of in-hospital complications and mortality, than patients aged 65-79 years old.
Methods
The Trauma Quality Improvement Program (2010-2016) was queried for burn trauma patients. To detect mortality risk a multivariable logistic regression model was used.
Results
From 282 patients, there were 73 (25.9%) octogenarians and 209 (74.1%) aged 65-79 years old. The two cohorts had similar median injury severity scores (16 vs. 15 in octogenarians, P = .81), total body surface area burned (P = .30), and comorbidities apart from an increased smoking (12.9% vs. 4.1%, P = .04) and decreased hypertension (52.2% vs. 65.8%, P = .04) in the younger cohort. Octogenarians had similar complications, including acute respiratory distress syndrome, pulmonary embolism, deep vein thrombosis (P > .05), and mortality (15.1% vs. 10.5%, P = .30), compared to the younger cohort. Octogenarians were not associated with an increased mortality risk (odds ratio 1.51, confidence interval 0.24-9.56, P = .67).
Discussion
Among burn trauma patients ≥65 years, age should not be a sole predictor for mortality risk. Continued research is necessary in order to determine more accurate approaches to prognosticate mortality in geriatric burn trauma patients, such as the validation and refinement of a burn-trauma-related frailty index.
Introduction
While there continues to be improvements in burn prevention including increased public awareness of fire safety, there were still nearly 500 000 patients with burn injuries requiring medical treatment in 2016. 1 In addition, the population of the United States is aging, with an estimated 13.2 million people age 80 years or older by 2020. 2 Consequently, the number of elderly burn and trauma patients is expected to increase, particularly when more elderly people are suffering from burn injuries when compared to a younger demographic. 3
A previous analysis from 2016 found an increasing linear correlation between the risk of mortality and age for patients suffering from burn injuries. 4 This study found that the 50% mortality rate (LD50) for burns is 45% total body surface area (TBSA) in a 55-year-old patient. The LD50 decreases to 25% TBSA in a 70-year-old patient, demonstrating that the elderly have worse outcomes from smaller burns. Aging is associated with more complications and worse clinical outcomes in burn trauma patients due to preexisting medical conditions, 5 impaired inflammatory and immune responses, 6 diminished functional reserve, impaired wound healing, 7 and thinner skin. 8 These factors make them susceptible to in-hospital complications including pneumonia, 9 acute respiratory distress syndrome, 10 multi-organ failure, 11 and a higher risk of mortality. 12 Lundgren et al 11 found that for elderly burn patients, the most significant predictors of in-hospital mortality risk were age and percentage of TBSA. Therefore, we hypothesized that octogenarians with concomitant burn and trauma injuries would have a higher rate of in-hospital complications as well as mortality, than patients aged 65-79 years old.
Methods
The Trauma Quality Improvement Program (TQIP) 13 database is a de-identified national database, and it was used to retrospectively analyze patients between 65 and 89 years old with burn injuries, defined by the International Classification of Diseases (ICD) version 9 diagnosis codes: 940-949, from January 2010 to December 2016. This study was deemed exempt by our institutional review board, and no consent was needed due to the de-identified nature of the national database. The TQIP database incorporates only patients with both traumatic injuries and burn injuries; therefore, patients that presented with isolated burns were not included.
Two groups were compared as follows: ages 65-79 years old (younger cohort) to ages 80-89 years old (octogenarians). The primary outcome of interest was in-hospital mortality. Secondary outcomes included discharge disposition, ventilator days, total hospital length of stay (LOS), intensive care unit (ICU) LOS, the in-hospital complications of unplanned intubation, pulmonary embolism (PE), unplanned intensive care unit (ICU) admission, pneumonia/ventilator-associated pneumonia (VAP), and deep vein thrombosis (DVT), among others.
We analyzed the patients’ prehospital comorbidities and the lowest systolic blood pressure (SBP) within the first 24 hours of admission. The prehospital comorbidities compiled included myocardial infarction (MI), diabetes, cerebrovascular accident (CVA), smoking, cirrhosis, hypertension, congestive heart failure (CHF), end-stage renal disease (ESRD), and chronic obstructive pulmonary disease (COPD). The injury analysis assessed included the TBSA of burns, injury severity score (ISS), and abbreviated injury scale (AIS) for the head, thorax, and abdomen. Other patient demographics included were age and sex.
Descriptive statistics were completed for all variables. A Mann-Whitney-U test was employed to compare continuous variables, and these data were reported as means with standard deviation or as medians with interquartile ranges. A chi-square test was used to assess the association between categorical variables, and percentages were used to report these data. The magnitude of the association between predictor variables and mortality was measured using a univariable logistic regression analysis. These variables were chosen based on a review of the literature.4,11,14 To control for covariates, a hierarchical multivariable logistic regression model was used. This was documented with an odds ratio (OR) and associated 95% confidence interval (CI). Values of P < .05 were considered statistically significant, and all P-values were two-sided. The statistical software of IBM SPSS Statistics for Windows, version 24 (Armonk, NY: IBM Corp) was used. This study adhered to all pertinent recommendations and standards as outlined in the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Informed consent was not possible to obtain as the TQIP holds a de-identified dataset.
Results
Patient Demographics and Primary Outcome
Demographics of Trauma Patients ≥65 Years With Burn Injuries.
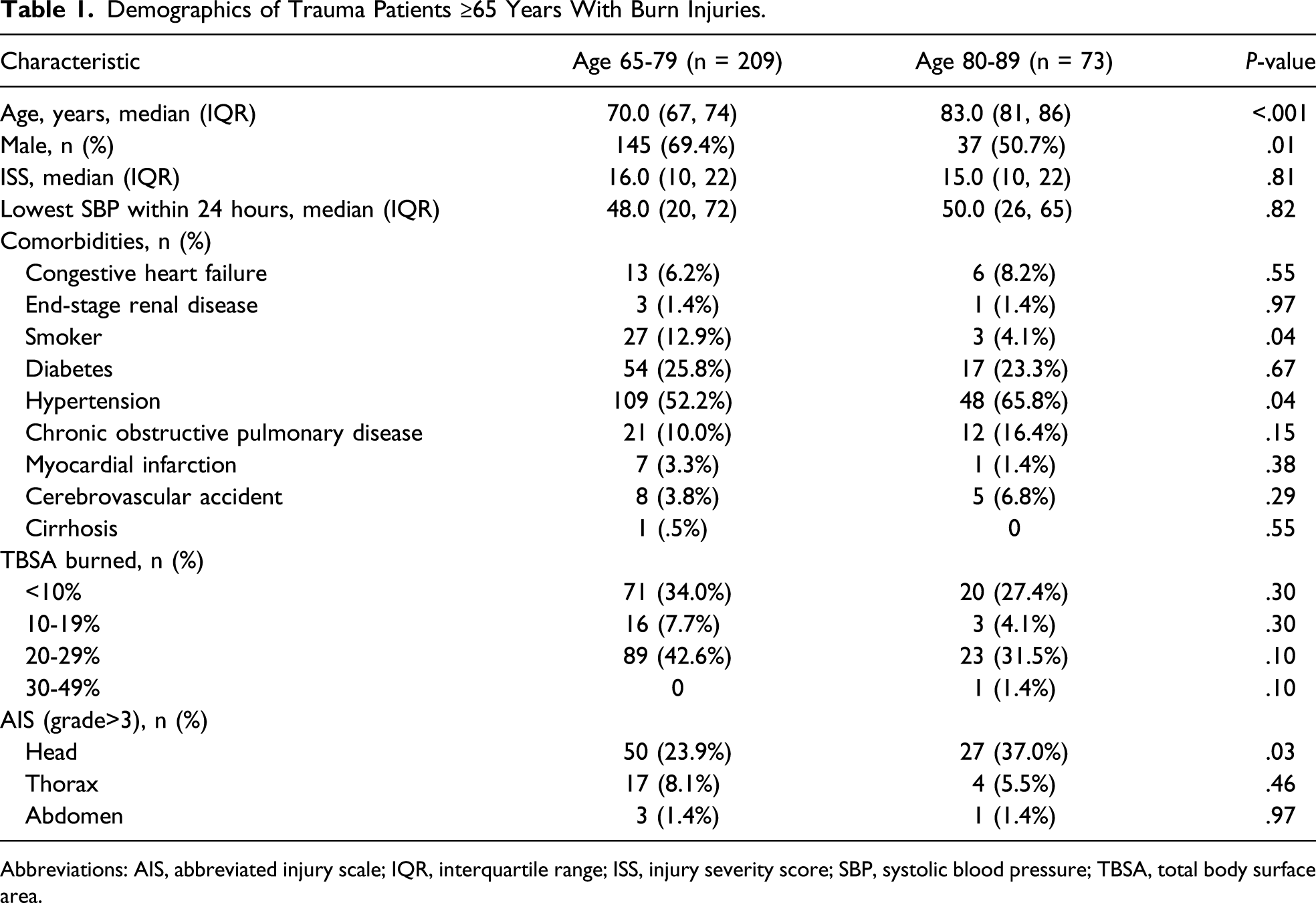
Abbreviations: AIS, abbreviated injury scale; IQR, interquartile range; ISS, injury severity score; SBP, systolic blood pressure; TBSA, total body surface area.
Mortality Risk Outcome
Adjusted Analysis for Risk of Mortality in Trauma Patients ≥65 Years With Burn Injuries.
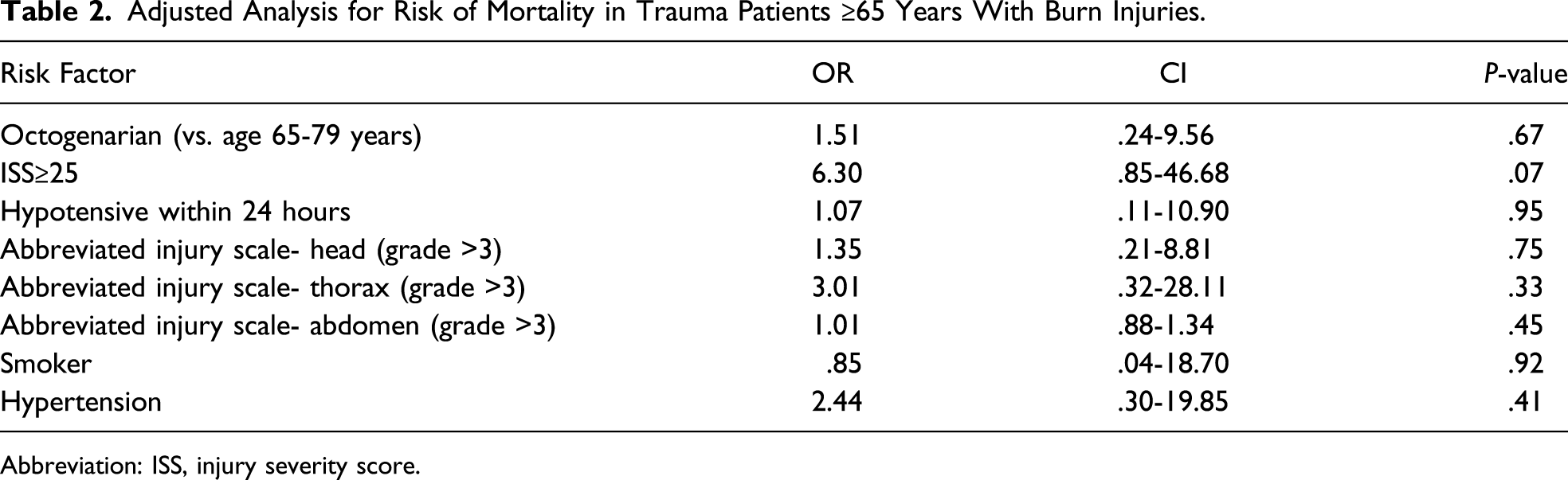
Abbreviation: ISS, injury severity score.
On a separate multivariable analysis, after excluding minor burns of TBSA <10%, there was no association with mortality risk in octogenarians compared to the younger cohort (OR .85, CI 0.14-5.15, P = .86). An ISS ≥25 was associated with an increased risk of mortality in burn trauma patients ≥65 years old (OR 6.55, CI 1.50-28.60, P = .01).
Hospital Outcomes
Outcomes of Trauma Patients ≥65 Years With Burn Injuries.
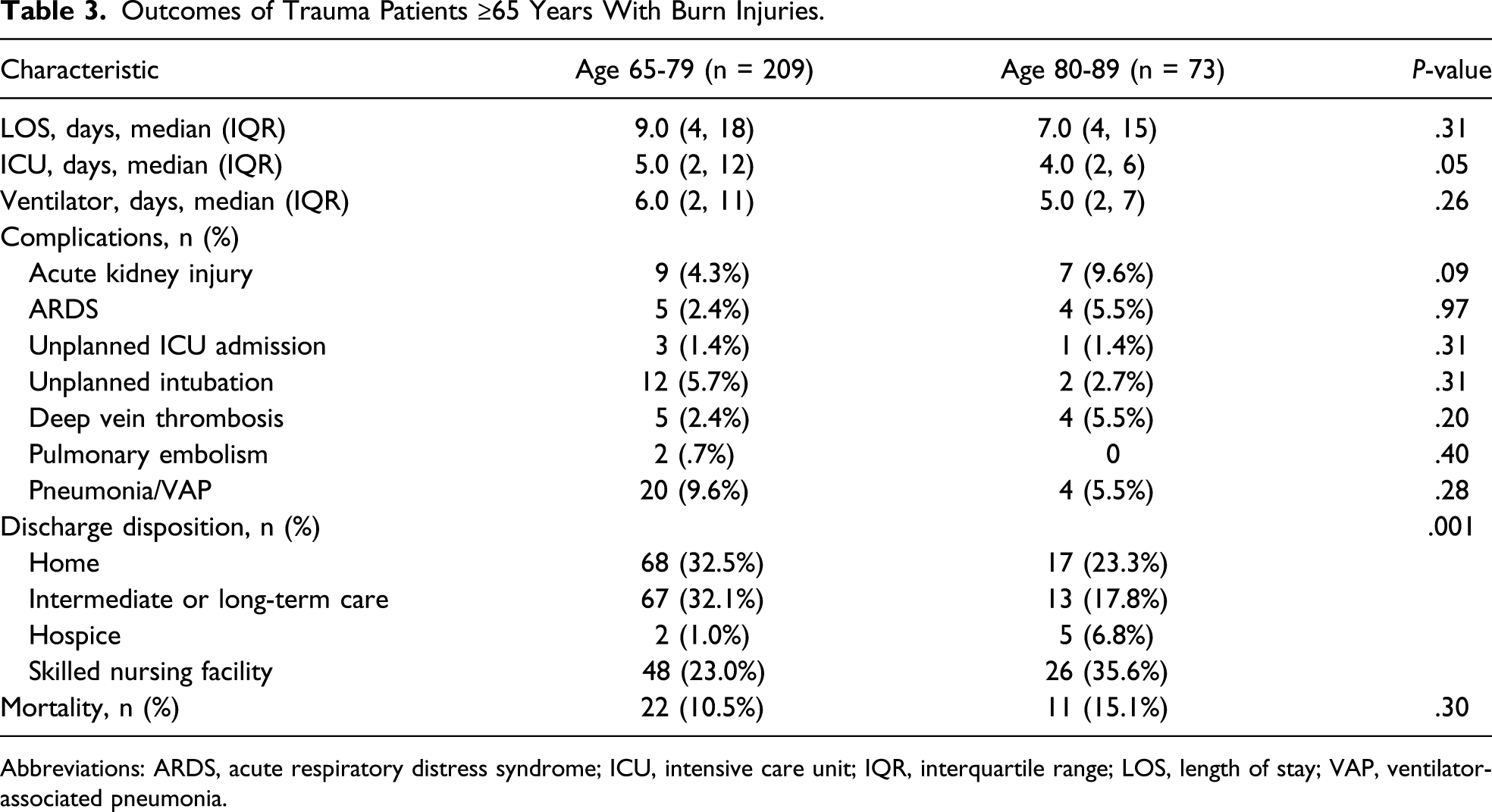
Abbreviations: ARDS, acute respiratory distress syndrome; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; VAP, ventilator-associated pneumonia.
Discussion
Due to an aging population, the number of elderly patients including octogenarians suffering burn injuries is expected to increase. The study demonstrates that octogenarians were not associated with an increased risk of mortality when compared to patients aged 65-79 years old; age therefore does not seem to be a significant predictor of mortality when comparing patients ≥65 years old. Octogenarian trauma patients with burn injuries also had similar LOS and rates of in-hospital complications including AKI, ARDS, DVT, PE, and pneumonia/VAP, when compared with younger geriatric patients.
Burn injuries in the geriatric population are associated with higher mortality. 15 In a previous large database study, age had a greater impact on mortality ≥60 years old than adults age 18-60 years old. 16 Jeschke et al studied burn injuries in 582 patients aged 0-99 years old from two databases with ≥20% TBSA burns and found the risk of mortality after burns increases linearly with increasing age. However, they could not define an age cutoff that predicted mortality vs. survivability thereby concluding that age is not an ideal predictor of burn outcome. 4 In comparison, our study looked specifically at elderly patients with a greater TBSA range plus concomitant trauma injuries and found no difference between the younger cohort and octogenarians in regards to mortality. Similarly, studies on both medical patients and trauma patients have also found age independently to be a poor predictor of mortality.17-21 Therefore, many fields of medicine and surgery have examined the use of a frailty index. 22 In regards to a burn frailty index, Masud et al performed a retrospective database study with 42 burn patients aged 65-95 years old and TBSA >10% from 2005-2009. They demonstrated that there was no significant difference between survivors and those who died with regard to age; however, there was a significant difference in regards to a frailty score which included fitness, comorbidities, and level of dependence. 15 Similarly, Romanowski et al found that increased admission frailty using the Canadian Study of Health and Aging Clinical Frailty Scale that included fitness, comorbidities, and level of dependence 21 is associated with mortality in burn trauma patients ≥50 years old. 23 A future prospective multicenter study is needed to evaluate and validate existing burn frailty indexes and/or develop a novel validated tool to determine risk of mortality in geriatric burn-trauma patients.
The geriatric population tends to have increased risk factors for adverse complications following burn injuries. However, this study demonstrated that octogenarians, when compared to patients 65-79 years old, had similar complication rates including AKI, ARDS, unplanned ICU admission, DVT/PE, and pneumonia/VAP. To further examine whether comorbidities and other factors (aside from age) may be more predictive of complications, Sepehripour et al performed a retrospective study on 129 burn patients ≥75 years old with TBSA burn from .5-43%. They calculated an admission frailty score using the Clinical Frailty Scale and compared patients who survived to patients that died within five years and found a significant correlation between the cumulative deficit frailty score (a model encompassing comorbidities, cognitive, and social factors) and complications. 24 Furthermore, Lundgren et al studied the impact of age and comorbidities on outcome in burn patients ≥55 years and found that infections were the most common complication, and the rate did not vary between the different age groups (55-64 years old vs. 65-74 years old vs. ≥75 years old). We also found similar rates of complications between our two cohorts, although our population was older (≥65 vs. ≥55 years old). This suggests that even in the extremes of older age, age alone is not a useful predictor of burn-trauma outcomes and should not be used as the sole decision maker for resource allocation and/or prognostication.
There are many limitations to this study including those inherent to a retrospective database study such as misclassification and missing data. In addition, our overall sample size was relatively small. Also, our population included predominant patients with smaller TBSA burns (primarily 20-29% TBSA); however, as previously mentioned, this degree of TBSA carries a significant mortality in elderly burn-trauma patients. Furthermore, limitations of the database include missing pertinent data variables such as the etiology of the burn, presence of inhalation injury, time from injury to admission, which patients had care withdrawn, and aspects of resuscitation and/or operative management which have been shown to affect burn-related outcomes. In addition, by using the TQIP database, these patients have traumatic injuries in addition to burn injuries; therefore, caution should be employed when generalizing results to patients with isolated burn injuries. In addition to the complications measured, there is a potential for non-index hospitalization complications and/or mortality, which are not captured in this database as well as a lack of long-term outcomes including functional and psychological outcomes. Lastly, while we focused on in-hospital mortality, there were a larger number of octogenarians that were discharged to skilled nursing facilities, and research has shown an association between older trauma patients and post-discharge mortality within a short period of time. 25
As our population continues to age and burn care has advanced, we now have improved ways to care for elderly burn patients 26 and thereby must develop better ways than just age to prognosticate outcomes and inform patients and families what to expect regarding morbidity and mortality associated with their burn injuries.
In conclusion, octogenarian trauma patients suffering from burn injuries appear to have a similar associated risk of in-hospital complications and mortality as patients aged 65-79 years old. Therefore, when focusing on patients ≥65 years old, age should not be used as a sole predictor for mortality risk in combined burn-trauma injuries. Continued research is necessary in order to determine more accurate approaches to prognosticate mortality in geriatric burn patients, such as the validation and refinement of a burn-trauma-related frailty index.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.