
Abstract
Background
Chemotherapy is associated with postoperative ventral incisional hernia (PVIH) after right hemicolectomy (RHC) for colon cancer, and abdominal wall closure technique may affect PVIH. We sought to identify clinical predictors of PVIH.
Methods
We retrospectively analyzed patients who underwent RHC for colon cancer from 2008-2018 and later developed PVIH. Time to PVIH was analyzed with Kaplan-Meier analysis, clinical predictors were identified with multivariable Cox proportional hazards modeling, and the probability of PVIH given chemotherapy and the suture technique was estimated with Bayesian analysis.
Results
We identified 399 patients (209 no adjuvant chemotherapy and 190 adjuvant chemotherapy), with an overall PVIH rate of 38%. The 5-year PVIH rate was 55% for adjuvant chemotherapy, compared with 38% for none (log-rank P < .05). Adjuvant chemotherapy (hazard ratio [HR] 1.65, 95% confidence interval [CI] 1.18-2.31, P < .01), age (HR .99, 95% CI .97-1.00, P < .01), body mass index (HR 1.02, 95% CI 1.00-1.04, P < .01), and neoadjuvant chemotherapy (HR 1.92, 95% CI 1.21-3.00, P < .01) were independently associated with PVIH. Postoperative ventral incisional hernia was more common overall in patients who received adjuvant chemotherapy (46% compared with 30%, P < .01). In patients who received adjuvant chemotherapy, the probability of PVIH for incision closure with #1 running looped polydioxanone was 42%, compared with 59% for incision closure with #0 single interrupted polyglactin 910.
Discussion
Exposure to chemotherapy increases the probability of PVIH after RHC, and non–short stitch incision closure further increases this probability, more so than age or body mass index. The suture technique deserves further study as a modifiable factor in this high-risk population.
Introduction
Postoperative ventral incisional hernia (PVIH) is a public health problem due to high incidence, complications related to bowel obstructions and rehospitalizations, impacts on patient-related outcomes, and associated increased health care costs.1-5 Cancer patients in particular have a much higher incidence of PVIH than the general population. Radiographic incidence of PVIH after colorectal surgery has been reported as high as 48%. 1 As cancer care is improving, so is survivorship, and downstream outcomes that develop with time, such as PVIH, are becoming more important. 2
Beyond surgical resection, treatment for colon cancer is directly linked to pathologic stage of disease. However, for some groups of patients, the role for adjuvant chemotherapy is debated, specifically in patients with pathologic stage II disease. 6 Additionally, the evolving role of immunotherapy in the adjuvant treatment of colon cancer, as well as the potential use of liquid biopsies to further guide the use of adjuvant chemotherapy, is the subject of ongoing investigation.7,8 Despite these ongoing efforts, standard chemotherapy including 5-fluorouracil and oxaliplatin remains an integral part of the management of stage II and stage III colon cancer. Therefore, it is important to understand the impact of systemic chemotherapy on the incidence of PVIH, especially given that some targeted therapies, such as bevacizumab, have known effects on wound healing and an association with PVIH.9,10
As with most public health problems, prevention is a key intervention in mitigating impact and cost. Short stitch abdominal wall closure is effective in reducing PVIH in randomized clinical trials, and long-term data validate its efficacy.11-13 A reduction in health care costs from hernia prevention has also been demonstrated when short stitch abdominal wall closure is used. 3 Despite this evidence, widespread practice of this technique is uncommon in the United States. 14
The high incidence of PVIH after colorectal surgery, availability of effective hernia prevention, and the evolving role of chemotherapy in patients with colon cancer present an opportunity to identify modifiable risk factors for reducing PVIH. The purpose of our study was to determine whether chemotherapy is associated with higher PVIH rates after colorectal surgery and to identify clinical predictors of PVIH. On the basis of prior studies, we hypothesized that PVIH occurs more frequently in colorectal cancer patients exposed to chemotherapy and that the probability of developing PVIH among patients exposed to chemotherapy increases with certain abdominal wall closure techniques.
Methods
After obtaining institutional review board review and approval, patients who underwent a right hemicolectomy (RHC) for stage I-IV colon cancer between January 2008 and December 2018 and later developed a radiographically or clinically diagnosed PVIH from a midline incision were identified from a prospectively maintained database. A radiographic PVIH was defined as a defect width greater than 2 cm on axial computed tomography planes; this is the defect size most hernia surgeons would agree requires surgical repair. 13 A clinical PVIH was defined as a patient-reported complaint of a bulge in the abdominal wall that appeared in the surgical incision after RHC and was corroborated by palpation of a fascial defect documented at a physical examination. Only patients with adenocarcinoma of the colon were included in the analysis because this is the most common indication for RHC at our institution. Selection for adenocarcinoma patients also reduces the confounding effects of different chemotherapies and differing tumor types.
Right hemicolectomy was selected for analysis because it is a procedure commonly performed in both community and academic settings and is typically performed with a midline incision. Abdominal wall closure techniques were not standardized in this retrospective study. Given advances in surgery, such as implementation of short stitch abdominal wall closure for hernia prevention, looped slow absorbable sutures for ease of abdominal wall closure, and surgeon preferences from practice-based learning, various abdominal wall closure techniques were represented in the study group for possible analysis. Robotic and laparoscopic RHC were not excluded from this analysis because all surgeons in this group performed specimen extraction and extracorporeal intestinal anastomosis through a midline incision larger than 2 cm. Additionally, RHC rarely requires creation of an ostomy, which is a possible confounding variable for development of PVIH.
Patient demographics, chemotherapy exposure, and abdominal wall closure techniques were collected. Neoadjuvant chemotherapy was defined as chemotherapeutic exposure prior to RHC. Adjuvant chemotherapy was defined as chemotherapeutic exposure after RHC. The most common indication for neoadjuvant chemotherapy was the presence of metastatic disease, although some patients with locally advanced colon adenocarcinoma also received neoadjuvant therapy following discussion by a multidisciplinary tumor board. Adjuvant chemotherapy was administered in accordance with National Comprehensive Cancer Network guidelines, and for patients with stage II disease, the decision to administer chemotherapy was at the discretion of the treating medical oncologist following discussion of risks and benefits with the patient.
Univariate analysis was performed to identify baseline differences in categorical variables (chi-square test) and continuous variables (t-test). These tests were implemented in Stata. The level of significance was set at α < .05. Time to PVIH formation was analyzed using the Kaplan-Meier method to determine rates of PVIH formation. 15 Multivariable Cox proportional hazards modeling was used to control for confounding variables and identify a combination of variables that could jointly predict the development of PVIH. 16 Given high-quality prior knowledge of the efficacy of the suture technique in the prevention of PVIH, 11 the retrospective nature of the study, and the possibility of multiple confounders and limited power, the posterior probability of developing PVIH after chemotherapy for a given abdominal wall closure technique was evaluated using Bayesian analysis and a naïve prior. 17 Kullback-Leibler divergence was used to determine the effect of the abdominal wall closure technique on prevalence of PVIH given exposure to chemotherapy and closure with the short stitch technique. These analyses were implemented in R 3.6.1.
Results
We identified 417 patients who underwent RHC; 399 had adenocarcinoma of the colon and were included in the analysis. Among these, 209 patients did not receive adjuvant chemotherapy, and 190 patients received adjuvant chemotherapy. Across both groups, 64 patients had neoadjuvant chemotherapy, and 28 of these patients had neoadjuvant bevacizumab. Among those who had adjuvant chemotherapy, 101 patients (53%) received 5-fluorouracil–based therapy, 47 (25%) capecitabine, 33 (17%) bevacizumab, and 9 (5%) had a different regimen (see Figure 1). Flowchart of patients included in the study based on cancer type, substratified by chemotherapy received (5-FU, 5-fluorouracil–based therapy).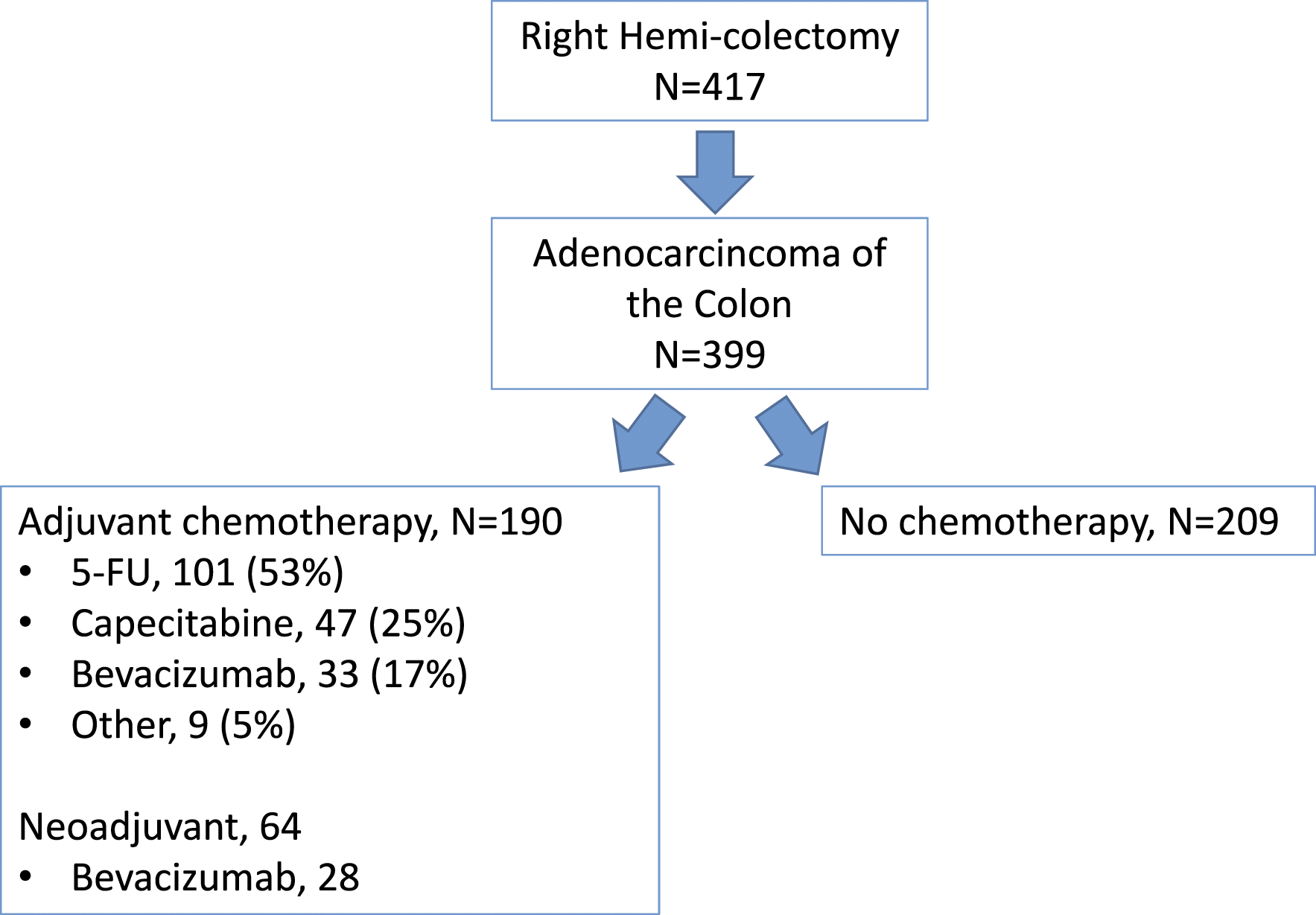
Characteristics of Patients Who Underwent Right Hemicolectomy Who Did or Did Not Receive Adjuvant Chemotherapy. a
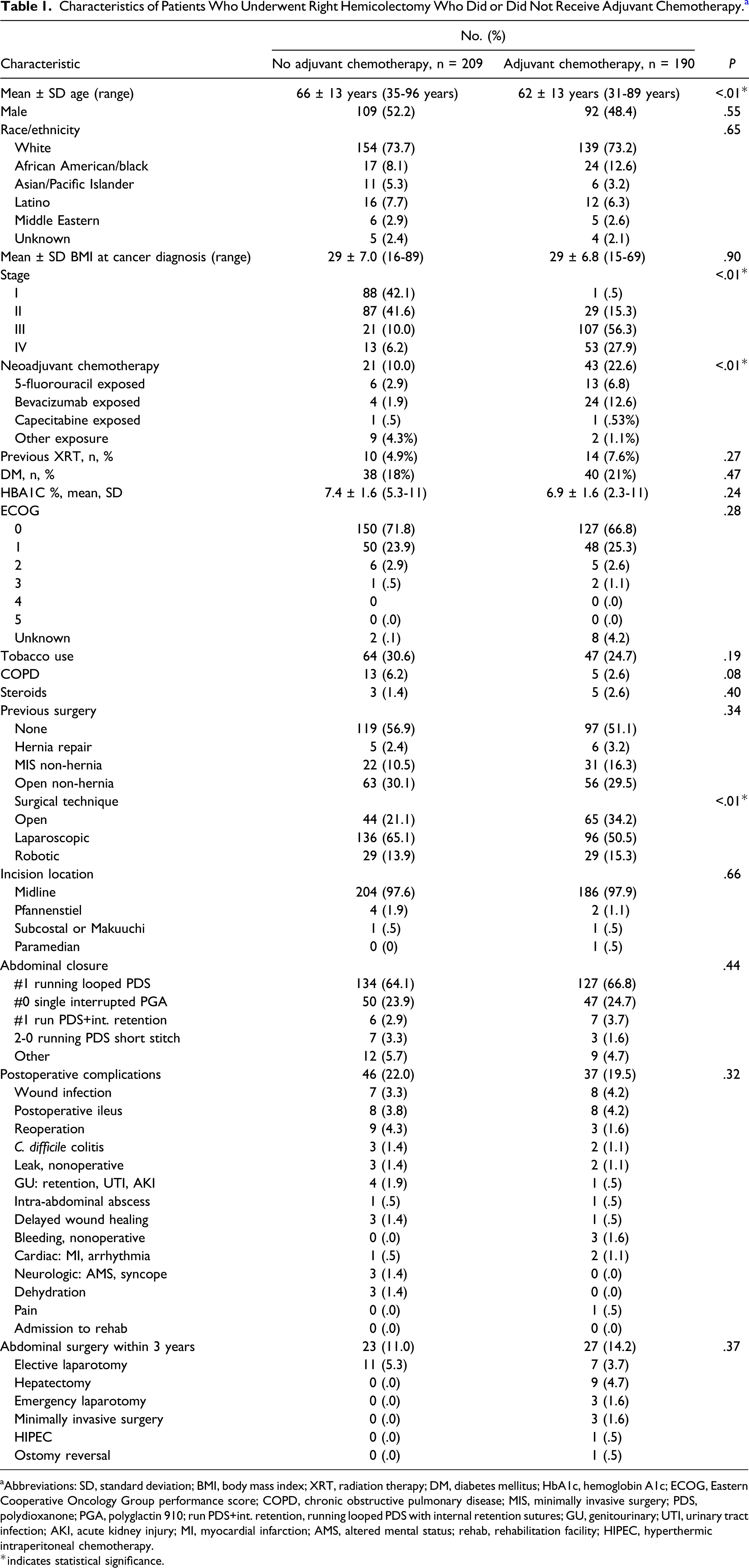
aAbbreviations: SD, standard deviation; BMI, body mass index; XRT, radiation therapy; DM, diabetes mellitus; HbA1c, hemoglobin A1c; ECOG, Eastern Cooperative Oncology Group performance score; COPD, chronic obstructive pulmonary disease; MIS, minimally invasive surgery; PDS, polydioxanone; PGA, polyglactin 910; run PDS+int. retention, running looped PDS with internal retention sutures; GU, genitourinary; UTI, urinary tract infection; AKI, acute kidney injury; MI, myocardial infarction; AMS, altered mental status; rehab, rehabilitation facility; HIPEC, hyperthermic intraperitoneal chemotherapy.
*indicates statistical significance.
Patients who received no adjuvant chemotherapy were more likely to have undergone laparoscopic RHC (65.1% compared with 50.5%), and patients who received adjuvant chemotherapy were more likely to have undergone open RHC (34.2% compared with 21.1%, P < .01). The rate of robotic RHC was similar between the groups (13.9% for no adjuvant chemotherapy and 15.3% for adjuvant chemotherapy). Most patients did not require additional surgical incisions aside from a midline incision, and there was no statistically significant difference in midline incisions between the groups (97.6% for no adjuvant chemotherapy and 97.9% for adjuvant chemotherapy, P = .66).
There were no statistically significant differences in abdominal wall closure techniques between the no adjuvant chemotherapy and adjuvant chemotherapy groups (Table 1). The most common abdominal wall closure technique was with a #1 running looped polydioxanone (PDS), a slow-absorbing, monofilament suture. The second most common closure technique was with a #0 single interrupted polyglactin 910 (PGA), a fast-absorbing, braided suture. Only 10 patients had abdominal wall closure with a 2-0 running PDS (short stitch abdominal wall closure). 11
There were no statistically significant differences in immediate postoperative complications between the no adjuvant chemotherapy and adjuvant chemotherapy groups (22.0% compared with 19.5%, P = .32; Table 1). Similarly, there were no statistically significant differences in non-hernia abdominal surgeries within 3 years of the index RHC (11.0% compared with 14.2%, P = .37).
Incidence of PVIH After Right Hemicolectomy, Methods of Diagnosis, Presenting Symptoms, and Proportion of Patients Pursuing Hernia Repair. a
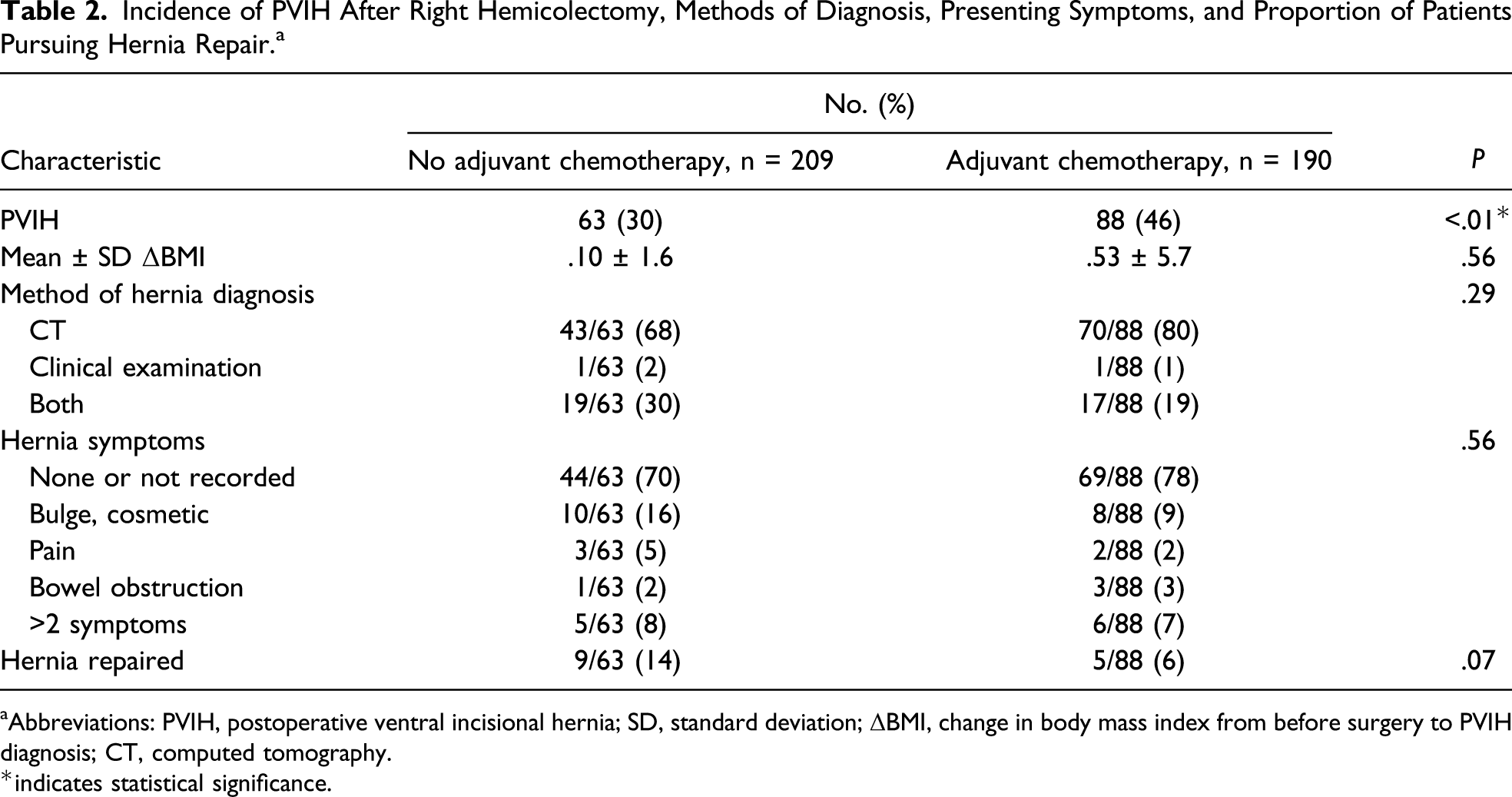
aAbbreviations: PVIH, postoperative ventral incisional hernia; SD, standard deviation; ΔBMI, change in body mass index from before surgery to PVIH diagnosis; CT, computed tomography.
*indicates statistical significance.
Time-to-event analysis showed a statistically significant difference in PVIH rates. The rate of PVIH formation at 5 years was 55% for patients who received adjuvant chemotherapy and 38% for patients who did not receive adjuvant chemotherapy (log-rank P < .001; Figure 2). At 2 years, 50% of patients who received adjuvant chemotherapy had developed PVIH. Univariate Cox proportional hazards modeling showed that adjuvant chemotherapy, neoadjuvant chemotherapy, young age, high BMI, advanced cancer stage, and previous minimally invasive non-hernia surgery were associated with a higher PVIH rate. After adjusting for confounding factors, multivariable Cox proportional hazards modeling showed that adjuvant chemotherapy (hazard ratio [HR] 1.65, 95% confidence interval [CI] 1.18-2.31, P < .01), BMI (HR 1.02, 95% CI 1.00-1.04, P < .01), and neoadjuvant chemotherapy (HR 1.92, 95% CI 1.21-3.00, P < .01) were independently associated with a high PVIH rate. Young age was independently associated with a low PVIH rate (HR .99, 95% CI .97-1.00, P < .01; Table 3). Kaplan-Meier curve for postoperative ventral incisional hernia (PVIH) recurrence over time, showing that the PVIH rate at 5 years was greater for patients who received adjuvant chemotherapy than for those who did not (55% compared with 38%, log-rank P < .01). Univariate and Multivariable Cox Proportional Hazards Modeling of Factors Associated With Postoperative Ventral Incisional Hernia.
a
aAbbreviations: HR, hazard ratio; CI, confidence interval; BMI, body mass index; MIS, minimally invasive surgery. *indicates statistical significance.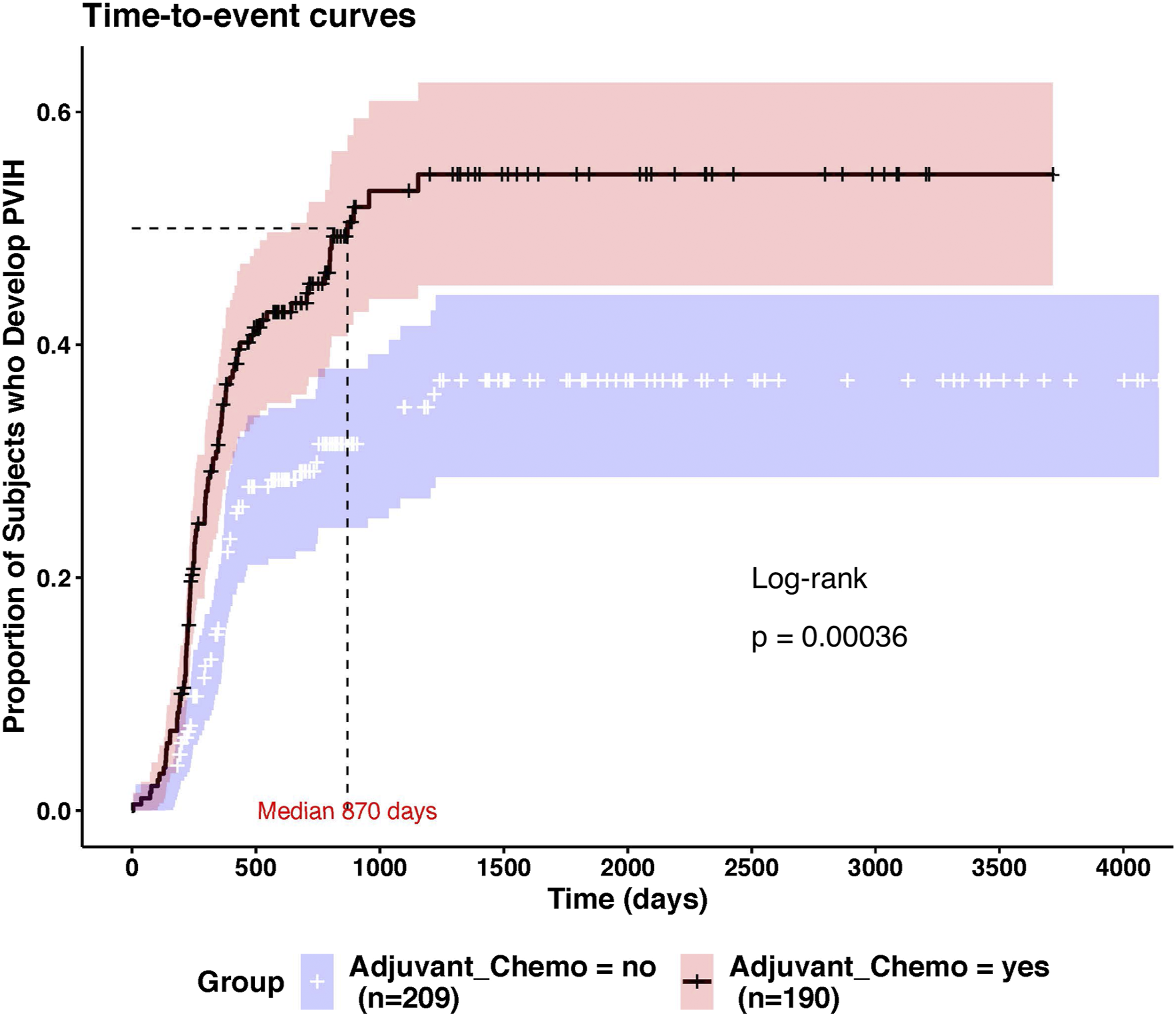
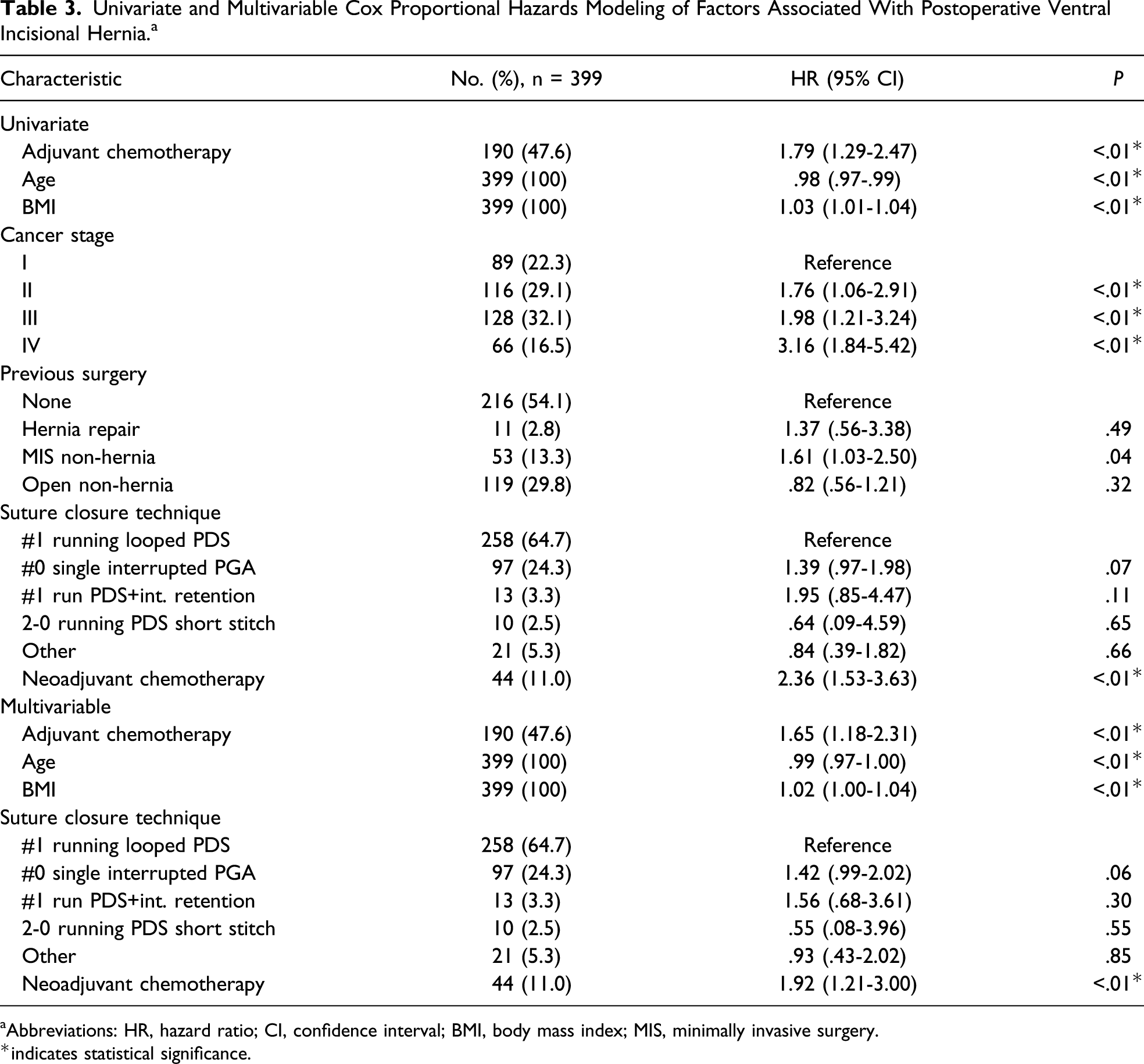
Cox proportional hazards analysis did not show any statistically significant independent associations of abdominal wall closure technique with PVIH rates; however, the effect sizes of these techniques appeared large despite the small sample size and lack of statistical significance. Relative to abdominal wall closure with #1 running looped PDS (n = 258), PVIH was more likely with closure with #0 single interrupted PGA (n = 97, HR 1.42, 95% CI .99-2.02, P = .06). Closure with 2-0 running PDS short stitch was performed in a small number of patients (n = 10) and could potentially decrease rates of PVIH (HR .55, 95% CI .08-4.0, P = .55), but this also did not reach statistical significance. Given the retrospective nature of the study, sample sizes were inadequately powered to show a statistically significant effect, although strong prior evidence from randomized controlled trials indicates that the short stitch suture technique can lower PVIH formation.
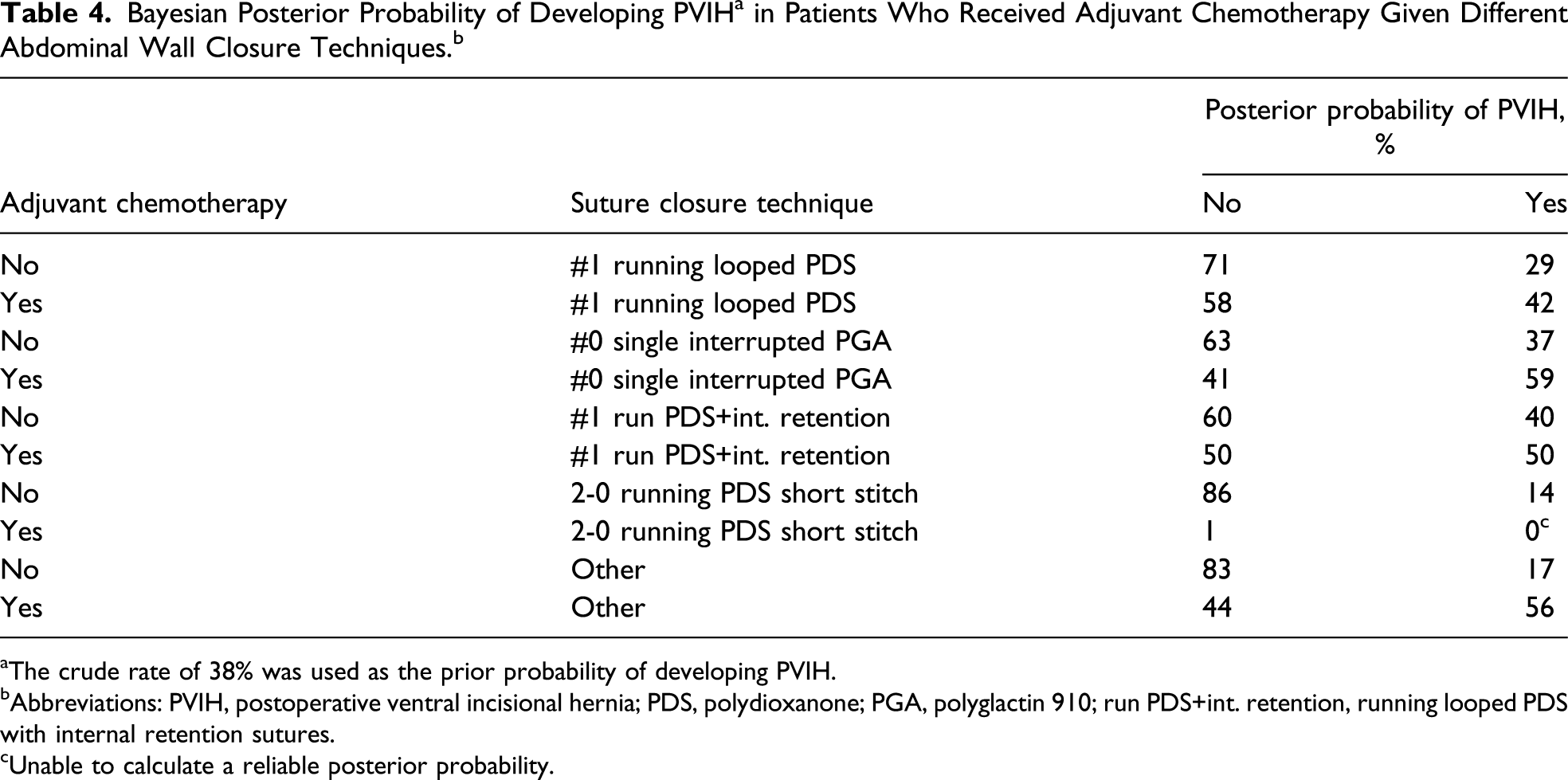
aThe crude rate of 38% was used as the prior probability of developing PVIH.
bAbbreviations: PVIH, postoperative ventral incisional hernia; PDS, polydioxanone; PGA, polyglactin 910; run PDS+int. retention, running looped PDS with internal retention sutures.
cUnable to calculate a reliable posterior probability.
Discussion
Our results indicate that chemotherapy and certain abdominal wall closure techniques increase the proportion and rate of PVIH after RHC. Patient factors independently associated with high PVIH rates include high BMI, adjuvant chemotherapy, and neoadjuvant chemotherapy. Non–short stitch abdominal wall closure techniques appear to have a clinically significant effect on the development of PVIH in patients who receive adjuvant chemotherapy.
Our study revealed surprising associations between BMI, adjuvant chemotherapy, and neoadjuvant chemotherapy and the development of PVIH. Body mass index is commonly regarded as a potentially modifiable risk factor for decreasing PVIH because it is considered completely dependent on the preoperative weight loss a patient can achieve. Unfortunately, our findings showed a minimal effect of BMI on PVIH formation. Each increase in BMI point increased the HR of PVIH by only 2%. Furthermore, there was no statistically significant change in postoperative BMI when comparing patients who received adjuvant chemotherapy with those who did not. Neoadjuvant and adjuvant chemotherapy had much larger effects on the rate of PVIH. Neoadjuvant chemotherapy increased the HR of PVIH by 92%, and adjuvant chemotherapy increased the HR by 65%. As treatment for colon cancer continues to improve, some oncologists may reason that patients with a low risk of recurrent colon cancer may not need postoperative chemotherapy, and it is tempting to consider chemotherapy in this subgroup of patients as a modifiable risk factor for PVIH. However, despite ongoing investigations into novel therapies and technologies to help guide treatment decisions, systemic chemotherapy remains an essential component of the treatment for colon cancer. 6 Further studies identifying colon cancer with features of low metastatic potential and demonstrating decreased need for systemic treatment are needed to support chemotherapy as a modifiable risk factor for PVIH.
The most modifiable risk factor for PVIH with the most impact in our study is the abdominal wall closure technique. The abdominal wall closure techniques presented in our study are common among practicing surgeons, and non–short stitch abdominal wall closure techniques are the standard of care for many surgeons. A strength of our study is the granular analysis of various suture techniques and their effect on PVIH in our population. Using conventional statistical analysis techniques, we found that the #1 running looped PDS and #0 single interrupted PGA techniques were not associated with statistically significant rates of PVIH. However, given the retrospective design of the study, the lack of statistical significance is likely due to lack of power. Similarly, multivariable Cox proportional hazards analysis showed that using the #0 single interrupted PGA technique increased the HR for PVIH by 42%, but the P-value was .06 after adjusting for chemotherapy, age, BMI, stage, and previous surgery. The potentially large effect size may have been statistically significant had more patient data been available for analysis. We surmounted these power limitations by using Bayesian analysis to examine the probability of PVIH given adjuvant chemotherapy and a specific abdominal wall closure technique. Bayesian inference showed that in patients who received chemotherapy, the probability of PVIH with commonly used abdominal wall closure techniques ranged from to 42% to 59%. Thus, the probability of PVIH in these patients is much higher than the overall rate of PVIH, which was 38% among all patients in our cohort. Although limited inferences could be made regarding the probability of PVIH with the 2-0 running PDS short stitch technique, Bayesian inference also suggests that the overall prevalence of PVIH may have been decreased by 30% among patients who received adjuvant chemotherapy and 2-0 running PDS short stitch for abdominal wall closure. Despite being used in a small number of patients, the appearance of the short stitch technique in our population suggests that surgeons know of the technique and may be interested in applying it to decrease the rate of PVIH.
Another strength of our study is the insight provided regarding surgical approach, timing, presentation, diagnosis, and treatment of PVIH in this population. It is commonly thought that minimally invasive surgical approaches result in lower rates of PVIH. In our cohort, although more patients in the no adjuvant chemotherapy group underwent laparoscopic RHC, no independent association was found between PVIH and surgical approach in the multivariable analysis. Additionally, the time course of PVIH differed in presentation between patients who received adjuvant chemotherapy and patients who did not. In patients who received adjuvant chemotherapy, 50% presented with radiographically diagnosed PVIH at 2 years after surgery, and this rate remained at 55% at 5 years. In contrast, less than half of patients who did not receive adjuvant chemotherapy presented with radiographic PVIH at 5 years. These findings suggest that screening for PVIH should begin earlier for patients who receive adjuvant chemotherapy.
In our study, the clinical diagnosis rate of PVIH was disproportionately lower than the radiographic diagnosis rate, most likely because follow-up visits focus on cancer surveillance and not screening symptoms of PVIH. Most patients did not report symptoms of PVIH, and a small proportion of patients (9-16%) reported a bulge or cosmetic deformity in the abdominal wall. Fewer patients may have mentioned symptoms in follow-up because they were not asked. Treatment of PVIH in our center was correspondingly low; only 6-14% of patients underwent subsequent hernia repair at our center, and it is possible some patients received hernia repairs at other hospitals during the period studied. Our study reveals the potential opportunity for increasing diagnosis and treatment of PVIH by recognizing that patients who received adjuvant chemotherapy may present with PVIH within 2 years of surgery, which would allow more specific PVIH screening at follow-up for oncologic surveillance and referral to hernia surgeons within our own center. Despite the low number of patients treated historically at our center, the recent development of a general surgery service with expertise in hernia surgery has increased our treatment of PVIH. Future applications of this knowledge include study of whether early screening and treatment of PVIH within 2 years of surgery may decrease morbidity and improve quality of life.
Our study has some limitations due to the retrospective nature of its design. Adjuvant chemotherapy exposure is broad, and we were unable to account for the specific effects of chemotherapeutic agents on PVIH. Although we broadly classified exposure to 5-fluorouracil, bevacizumab, and capecitabine, patients may have had multiple exposures to these agents owing to participation in clinical trials, medical oncologist experience, or patient preference. Accordingly, any dose effect of specific chemotherapeutic agents on the development of PVIH could not be analyzed reliably. Bevacizumab has known effects on wound healing, and although it could contribute to PVIH, we were unable to find a direct association between bevacizumab and PVIH rates. More patients who received neoadjuvant chemotherapy also received bevacizumab, and thus neoadjuvant chemotherapy may be a proxy variable for bevacizumab. This may explain the higher PVIH rates seen in patients who received neoadjuvant chemotherapy. Last, at our tertiary cancer center, novel chemotherapeutic drugs are used frequently and may have better safety profiles, fewer effects on wound healing, and ultimately PVIH. Given the 10-year period of study, the secular effects of improvements in chemotherapeutic agents on PVIH may not have been accounted for.
Our study is hypothesis-generating, and the most impactful risk factor to explore prospectively is abdominal wall closure for prophylactic PVIH prevention. There was low adoption of the 2-0 running PDS short stitch technique in our population, likely because experience, training, and evolution of this abdominal wall closure technique would have occurred during the latter part of the period studied. Although randomized studies have shown efficacy of this technique in a controlled population, this technique has not been studied for effectiveness in a pragmatic fashion, particularly in a US population that is more obese and disproportionally affected, such as colorectal cancer patients receiving surgery. Given the high risk of PVIH in this population, there may be additional opportunities to explore additional techniques such as placement of prophylactic mesh.
Postoperative ventral incisional hernia in colon cancer patients undergoing RHC is common and associated with cancer-related interventions, such as adjuvant chemotherapy and the specific abdominal wall closure technique used. PVIH rates are proportionately higher and occur sooner in patients exposed to chemotherapy, and they are potentially underdiagnosed and treated. Because cancer patients are surviving longer, prevention of downstream morbidity from PVIH by changing the abdominal wall closure technique deserves prospective study in a pragmatic trial.
Footnotes
Acknowledgements
We thank Erica Goodoff, Senior Scientific Editor in the Research Medical Library at The University of Texas MD Anderson Cancer Center, for editing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.