
Abstract
Background
Abdominal wall reconstruction in high-risk and contaminated cases remains a challenging surgical dilemma. We report long-term clinical outcomes for a rifampin-/minocycline-coated acellular dermal graft (XenMatrix™ AB) in complex abdominal wall reconstruction for patients with a prior open abdomen or contaminated wounds.
Methods
Patients undergoing abdominal wall reconstruction at our institution at high risk for surgical site occurrence and reconstructed with XenMatrix™ AB with intent-to-treat between 2014 and 2017 were included. Demographics, operative characteristics, and outcomes were collected. The primary outcome was hernia recurrence. The secondary outcomes included length of stay, surgical site occurrence, readmission, morbidity, and mortality.
Results
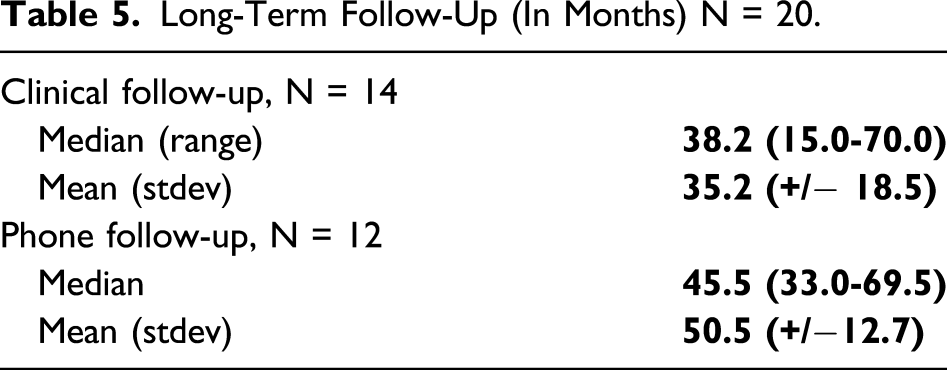
Twenty-two patients underwent abdominal wall reconstruction using XenMatrix™ AB during the study period. Two patients died while inpatient from progression of their comorbid diseases and were excluded. Sixty percent of patients had an open abdomen at the time of repair. All patients were from modified Ventral Hernia Working Group class 2 or 3. There were a total of four 30-day infectious complications including superficial cellulitis/fat necrosis (15%) and one intraperitoneal abscess (5%). No patients required reoperation or graft excision. Median clinical follow-up was 38.2 months with a mean of 35.2 +/− 18.5 months. Two asymptomatic recurrences and one symptomatic recurrence were noted during this period with one planning for elective repair of an eventration. Follow-up was extended by phone interview which identified no additional recurrences at a median of 45.5 and mean of 50.5 +/−12.7 months.
Conclusion
We present long-term outcomes for patients with high-risk and contaminated wounds who underwent abdominal wall reconstruction reinforced with XenMatrix™ AB to achieve early, permanent abdominal closure. Acceptable outcomes were noted.
Keywords
Key Takeaways:
Numerous factors place patients undergoing abdominal wall reconstruction at increased risk for recurrence and hernia-related complications, with the necessity of mesh removal remaining a feared complication of synthetic mesh placement in such cases. Despite a paucity of evidence that biologic grafts alone prevent surgical site infection, they are often used in contaminated and high-risk cases of abdominal wall reconstruction with the goal of avoiding graft explantation and its dire consequences. The incorporation of longitudinally-released antimicrobials into biologic graft materials may confer further benefit to the use of acellular dermal grafts through the mitigation of bacterial seeding and inflammation over time which is supported by the positive outcomes of this study.
Introduction
Abdominal wall reconstruction (AWR) in contaminated surgical fields remains a challenging surgical issue. There are more than four million laparotomies and approximately 350 000 ventral hernia repairs (VHR) performed annually in the United States alone. 1 An estimated 2-5% of patients who undergo laparotomy and 10-25% of all trauma patients who receive surgery are managed with an open abdomen (OA). 2 For patients with complex defects and loss of abdominal domain, AWR is required to reestablish abdominal wall integrity. Mesh placement is associated with lower rates of defect recurrence compared to primary repair; however, its placement is associated with a unique set of potential complications. 3 In contaminated fields, infection of the implanted prosthetic is the primary concern, occurring in up to 10% of ventral hernia repairs, with higher incidence noted in open repairs.4,5 Additionally, chronic pain, hernia recurrence, seroma, and visceral adhesion formation leading to bowel obstruction, erosion of viscera, and enterocutaneous fistula (ECF) formation are other mesh-related complications often necessitating further operative intervention. Such issues lead to significant patient morbidity, increased cost, and prolonged hospitalization.4-6
Cases involving contaminated surgical fields, reconstruction of complex wounds, and open abdominal closure are a greater challenge. Defect-related factors including large defect size, a contaminated surgical field, and repair completed without mesh reinforcement increase the risk of hernia formation, surgical site infection (SSI), and reoperation. 7 Patient-related factors such as smoking and comorbid conditions further increase this risk.8-11
Patients with peritonitis, severe sepsis from an abdominal etiology, and traumatic intra-abdominal organ injury are frequently managed with temporary closure of the abdominal fascia, or an open abdomen, following the initial operation. Most of these patients will be managed with a temporary fascial closure with subsequent delayed (typically 6-12 months) or early (typically within 2-3 weeks) permanent closure.11,12 Delayed fascial closure is often implemented to avoid the complication of intra-abdominal hypertension in the critically ill patient in exchange for an increased risk of ventral hernia formation. 13 Importantly, for patients with open abdomens, early definitive closure has been identified as an important factor associated with improved survival.14,15
With such considerations in mind, techniques and materials that mitigate infectious risk while offering a sufficient structure to obtain a durable closure have been implemented; however, with inconsistent results. Biologic acellular dermal matrices (ADM) are a logical solution due to a composition allowing for tissue integration and neovascularization, theoretically facilitating improved delivery of immune cells and antibiotics. 16
The XenMatrix™ AB Surgical Graft (C. R. Bard, Inc. [Davol], Warwick, RI) is a non–cross-linked porcine acellular dermal graft (NCPADG) with a tyrosine polymer coating which contains the antibiotics rifampin and minocycline. Studies preceding its clinical application demonstrated inhibition of multidrug-resistant Staphylococcus aureus (MRSA), Escherichia coli, and other bacteria which protect the implanted graft prior to neovascularization and prevent bacterial biofilm formation.16,17 Numerous preclinical studies have investigated the in vitro effects of antimicrobial releasing polymers since and with promising results (Figure 1).18-20 XenMatrix™ AB is an antibacterial coated, non–cross-linked porcine acellular dermal graft. The polymer coating contains a combination of rifampin and minocycline.
Early clinical outcomes for XenMatrix™ AB in complex abdominal defects were promising with a low rate of postoperative SSO and other postoperative complications. 21 Initial clinical evaluation via a multi-institutional retrospective study of seventy-four patients who underwent complex AWR assessed outcomes in the first thirty days postoperatively and through six-month follow-up with low rates of SSO and hernia recurrence, possibly related to the antimicrobial properties of the mesh. 21 Herein, we present long-term outcomes for our institutional cohort who underwent complex AWR using the XenMatrix™ AB Surgical Graft to achieve early permanent closure.
Methods
This study is a planned follow-up of long-term clinical outcomes for patients at our center who were included in a previously published multicenter study. 21 An in-depth description of the study design is available for review in that previously published work. 21 Approval for the study was obtained from our center’s Institutional Review Board. Data were retrospectively collected on patients who underwent open or laparoscopic AWR using XenMatrix™ AB at Carolinas Medical Center between December 2014 and December 2017.
This study’s inclusion criteria and exclusion criteria were as follows: age ≥17 years, presence of a ventral hernia requiring open or laparoscopic repair, use of XenMatrix™ AB, Ventral Hernia Working Group (VHWG) class ≥2, modified VHWG classification ≥2, and at least 30 days of postoperative follow-up. The exclusion criteria mirrored that of the original study and included incomplete removal of any existing mesh from a prior repair in the same area, defined collagen disorder, known sensitivity to porcine products, known infection by human immunodeficiency virus, pregnant or breastfeeding status or plans to become pregnant during the study period, and a history of allergy or hypersensitivity to tetracyclines or rifamycins.
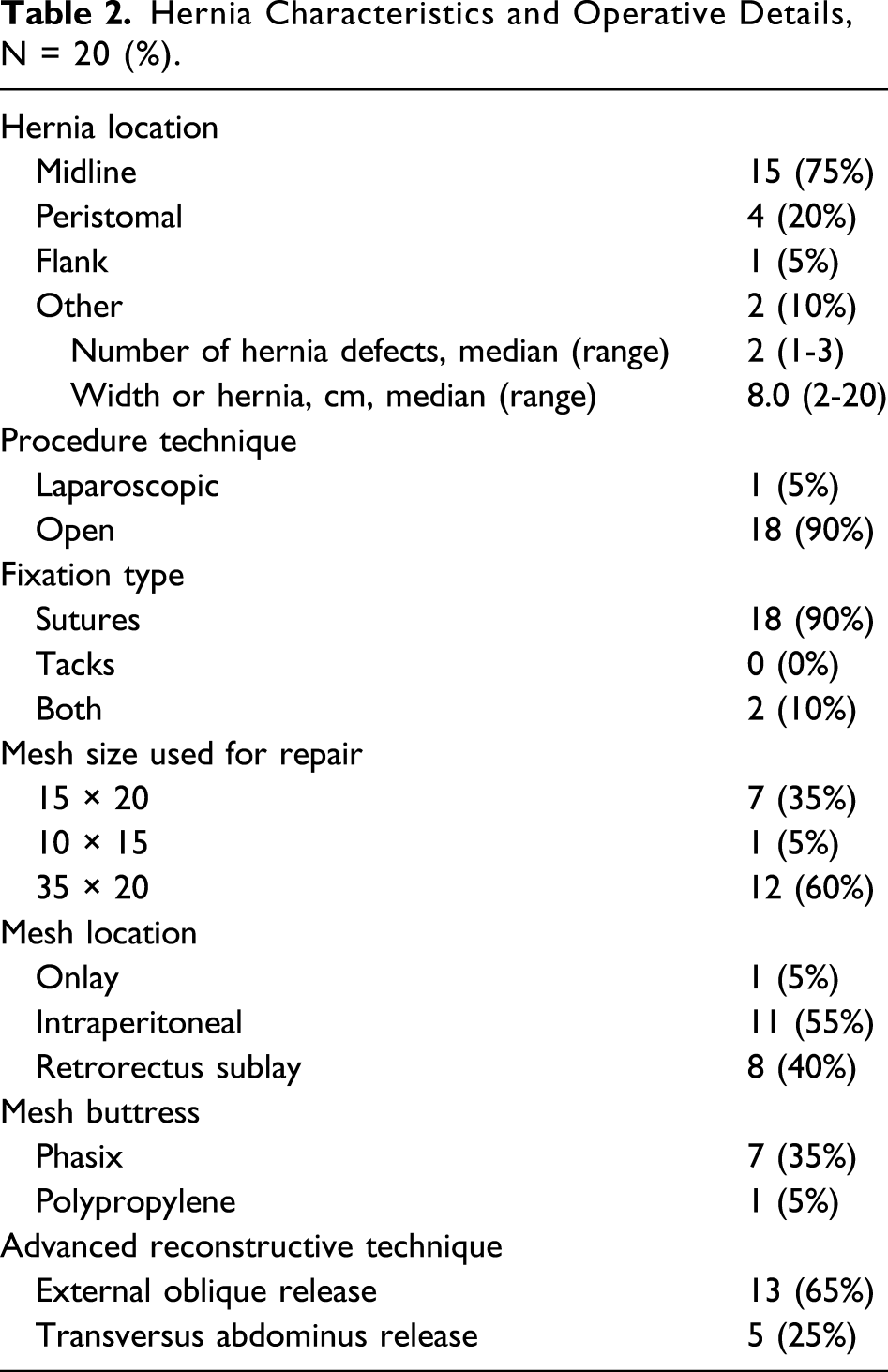
Repair type and graft locations were determined at the discretion of the operating surgeon and included onlay, intraperitoneal sublay, and retrorectus sublay. Fixation of the grafts was primarily achieved through transfascial suture fixation with monofilament absorbable sutures. Complex abdominal wall defects required the application of advanced reconstructive techniques including thirteen patients who underwent external oblique release (EOR) and five patients who received a transversus abdominis release (TAR) to ensure adequate defect coverage and fascial overlap. An onlay buttress (7 Phasix; 1 Polypropylene) was performed in cases where complete defect coverage could not be achieved with physiologic intra-abdominal pressures.
Patient demographics, operative, perioperative, and postoperative data were collected. Descriptive statistics were used to calculate quantitative data including mean and median values, standard deviations, and proportions. Frequency and proportion tables were used to summarize the qualitative data. Hernia grade was determined by the VHWG and modified VHWG classification, which stratify patients undergoing AWR into groups based on SSO risk. In the VHWG classification, patients are stratified into four grades based on SSO risk: Grade I are patients of low risk with no history of wound infection; Grade II are patients with comorbidities with no previous wound infection; Grade III are patients potentially contaminated with history of wound infection or entry into the gastrointestinal tract; and Grade IV are patients actively infected. 22 The modified VHWG classification, which sought to improve the accuracy of the original classification to predict SSO risk, uses three grades: Grade 1 are patients of low risk with no history of wound infection; Grade 2 are patients with comorbidities or previous wound infection; and Grade 3 are patients with contaminated cases which can be further stratified by Centers for Disease Control (CDC) wound class into clean-contaminated, contaminated, and dirty wounds. 23 The primary outcome of interest was hernia recurrence. The secondary outcomes included SSO, readmission, morbidity, and mortality. Data were analyzed with intent-to-treat.
Results
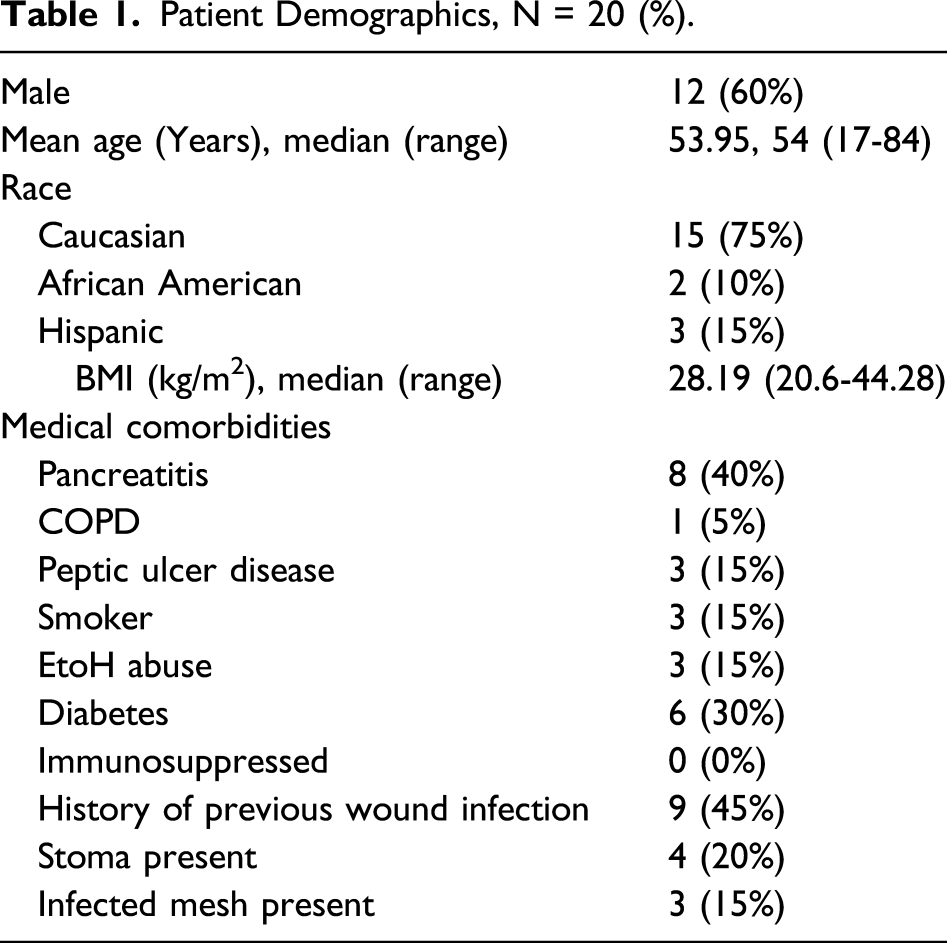
Patient Demographics, N = 20 (%).
Hernia Characteristics and Operative Details, N = 20 (%).
Ventral Herina Working Group Classification N = 20.
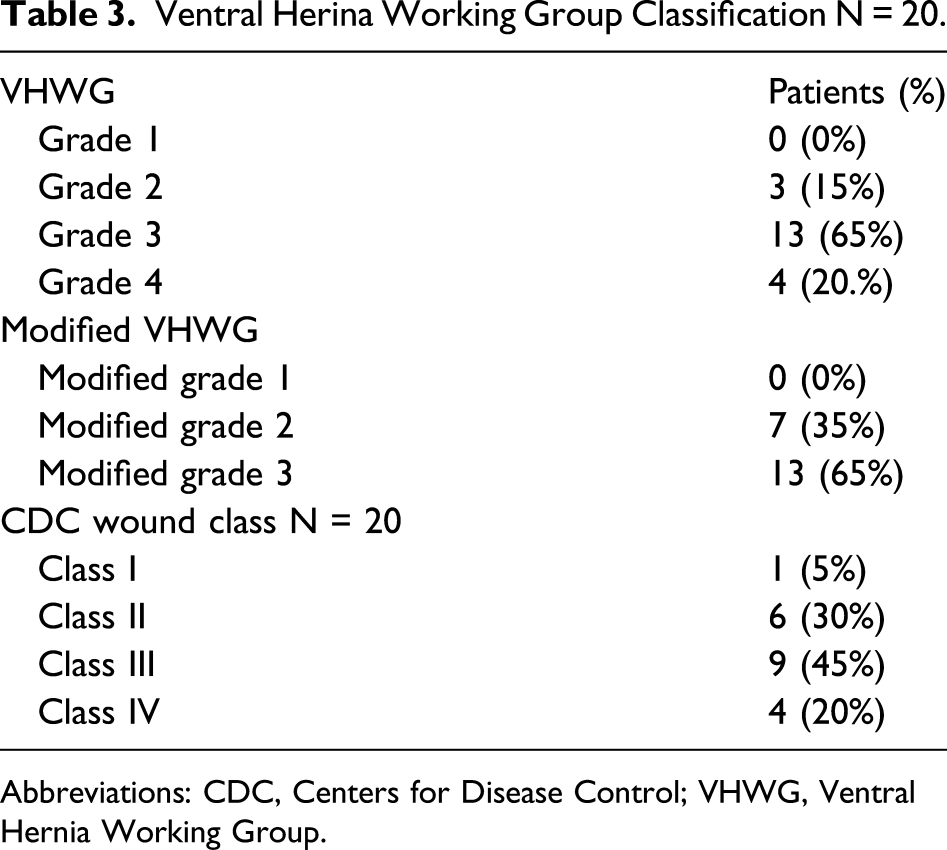
Abbreviations: CDC, Centers for Disease Control; VHWG, Ventral Hernia Working Group.
Long-Term Postoperative Outcomes and Complications N = 20.
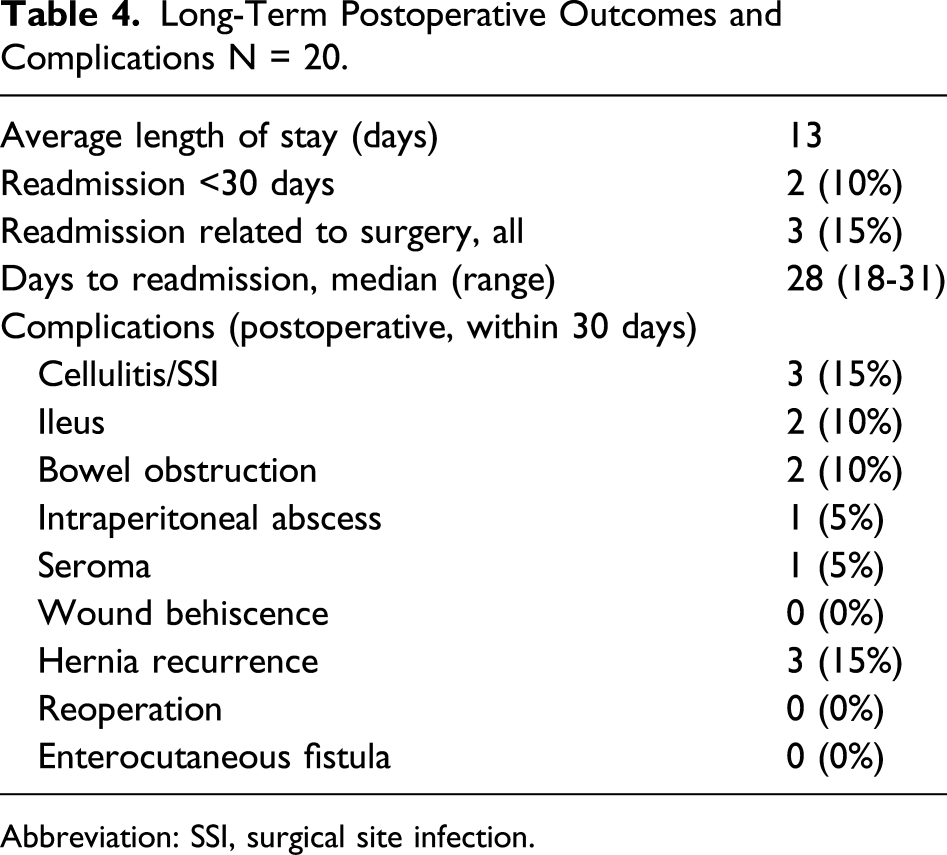
Abbreviation: SSI, surgical site infection.
Details regarding post-procedural complications and long-term follow-up from 31 days to 70 months following AWR/graft implantation were obtained with zero patients developing ECF, wound dehiscence, or requiring reoperation. Two patients developed cellulitis treated with antibiotics on an outpatient basis. Two patients also developed bowel obstruction that did not require operative intervention. One patient developed a seroma which was managed without procedural intervention. There were two asymptomatic hernia recurrences and one symptomatic recurrence noted in long-term follow-up. These included subcostal, midline, and paramedian recurrences.
Long-Term Follow-Up (In Months) N = 20.
Discussion
The widespread application of the tension-free repair for body wall defects and open abdomen has come with several attendant advantages, but also a variety of challenges and complications. While mesh or graft use to buttress abdominal wall defects is associated with a more durable repair, bacterial colonization and infection of the implanted foreign body can lead to a vicious cycle of complications and patient morbidity. 25 Complex wounds and contaminated fields further complicate management. Despite numerous graft options and the frequent creation of novel technologies to address hernia-related issues, the optimal solution to the challenges surrounding infectious graft-related complications remains unclear.26-31
Properties intrinsic to biologic grafts allowing for revascularization and ingrowth into the host’s native tissue have made biologic grafts a popular choice among surgeons, particularly in the setting of an infected or contaminated surgical field.32,33 Still, outcomes in this patient population remain unsatisfactory and new strategies to address these shortcomings are necessary.24,27-29 Holihan et al 26 noted postoperative infection rates nearing sixty-five percent in cases with bowel contamination, even when using biologic mesh underlay. Additionally, the risk of mesh infection increases in cases with concomitant procedures, often requiring mesh explantation. 34 For these reasons, there are no abdominal wall grafts approved by the US Food and Drug Administration (FDA) to be placed in an infected field.34,35
Biologic grafts alone do not prevent SSI or graft contamination. The true benefit of biologic grafts is their ability to obviate the need for explantation should the graft become exposed or the surgical site become contaminated, as their incorporation facilitates neovascularization and perfusion at the site and consequentially the penetration of administered antimicrobials.16,25 The characteristics of the polymer coating surrounding the XenMatrix™ AB Surgical Graft allow for prolonged antibiotic release imparting longitudinal benefit over time. 36 The longitudinal release of antibiotics may confer additional benefit through the mitigation of deleterious inflammation and prevention of bacterial seeding.17-20
There is a paucity of literature assessing long-term outcomes following graft implantation in contaminated settings, particularly with an intent-to-treat and to obtain a permanent abdominal closure. Previous evaluation of the XenMatrix™ AB Surgical Graft placement in complex abdominal wound closure and contaminated surgical fields demonstrated its safety and revealed promising short-term patient outcomes. 21
The patient population included in this study exhibited multiple comorbid conditions, as evidenced by eighty-five percent falling under the VHWG grade 3 or 4 wound classification and all patients being classified as modified VHWG grade 2 or 3. Clinical conditions requiring several days of open abdominal management and large defect size also inevitably put this population at increased risk for developing SSI and wound complications.11,14,15,25
Many patients presented with complex abdominal wall defects and loss of abdominal domain requiring the application of advanced reconstructive techniques such as transversus abdominis muscle release (TAR), external oblique release, and the “sandwiching” of grafts to achieve a durable repair. Although the authors feel an extraperitoneal, retrorectus sublay is the best position for a reinforcing material during ventral hernia repair, several factors including defect location (ie, lumbar hernias), a surgically absent rectus muscle, substantial thinning of fascial layers, and large defect size precluded preperitoneal, retrorectus graft placement. The heterogeneity of graft location is reflective of the breadth and severity of the presenting clinical conditions in this patient population.
Notably, rates of wound complication and SSI remained low even with a median of 38.2 months of clinical follow-up and 45.5 months of phone interview follow-up after repair. Graft antibiotic coating may aid in bacterial clearance, particularly in contaminated environments, and may have potentially contributed to the low rate of SSI reported in this series. Rates of SSI following VHR with biologic grafts range from 4.7 to 22.3%, based on a systematic review published in 2013. 37 Cost is a significant concern when using biologic grafts; therefore, the VHWG classification system and other risk stratification techniques should be applied to assess a patient’s risk and to balance cost with a graft’s ability to mitigate the incidence and risk of complications. Importantly, among patients in this series with noted recurrence, none required hernia-related reoperation (although one patient is considering intervention for eventration at site of previous transverse rectus abdominis myocutaneous (TRAM) flap) and no patients developed an ECF following AWR. Three patients ultimately required readmission in the immediate postoperative period, and only one of these was related to an SSO following AWR.
Multiple factors likely influenced the low rate of SSO observed in this study. Detailed, patient-specific operative and perioperative care including thorough medical optimization prior to fascial closure was implemented. Procedures were staged and preceded by clinically appropriate washouts prior to graft placement. As described above, defects with inadequate coverage were buttressed with an onlay mesh, which has been demonstrated to improve outcomes. 26 Additionally, deaths in high-risk patients may have masked cases of eventual recurrence. Graft-related considerations include a theorized increase in vascular penetrance which may facilitate wound healing. Furthermore, effective longitudinal antibiosis could attenuate levels of inflammation that may otherwise compromise wound healing.
The study is limited by multiple factors common to retrospective chart review and single-center studies. 38 The patient sample size is limited due to its single institution structure and its aim to primarily investigate high-risk patients. Both the limited sample size and retrospective study design have the potential to introduce bias into the interpretation of the results. 38 The study population was relatively heterogeneous, but the primary feature of interest being high-risk and contaminated cases was appropriately captured. Given the complexity of our patient population and the variable nature of ventral hernias in general, we are unable to meaningfully identify specific factors that may contribute to hernia recurrence following repair with an antibiotic-coated NCPADG. However, the positive findings in this diverse group of extremely complex patients for whom AWR is notoriously difficult remain promising. As such, we believe further investigation through a randomized controlled trial is warranted and would more clearly demonstrate a relationship between the antibiotic coating and the prevention of both short-term and long-term complications in these patients.
Conclusion
We present long-term follow-up for patients with high-risk and contaminated wounds who underwent AWR reinforced with a novel rifampin-/minocycline-coated NCPADG (XenMatrix™ AB). Its use was associated with a low rate of postoperative SSO and postoperative complications during the first 30 days and through long-term follow-up. No negative effect of XenMatrix™ AB was demonstrated to patients, and importantly, wound complication rates were notably low, given preexisting patient- and hernia-related factors. A low rate of hernia recurrence was observed at a median of 38.2 months of clinical follow-up and 45.5 months of phone follow-up. A small study size and retrospective study design substantially limit the generalizability of these findings; however, given the observed safety and acceptable clinical outcomes noted in this study, prospective investigation of antibiotic-coated grafts in this patient population is warranted.
Footnotes
Author Contributions
Study conception and design: Robinson, Baker, and Iannitti
Acquisition of data: Robinson, Sulzer, and Iannitti
Drafting of Manuscript: Robinson and Iannitti
Critical Revision: Robinson, Baker, Motz, and Iannitti
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Iannitti serves as a consultant for BD Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed Consent
This study has been reviewed by our Institutional Review Board who was determined that this type of study does not require informed consent.