
Abstract
Obturator hernias are quite rare in the world of hernias, and one that contains an acutely inflamed appendix becomes a very rare case indeed. An obturator hernia containing the appendix has been reported only 5 times in the surgical literature. Three of those cases were in elderly women with delayed presentations and were fatal. The most recent case was in a young woman with prompt laparoscopic appendectomy and no complications. We present a case in a 25-year-old man presenting with acute appendicitis and found to be incarcerated within the obturator canal during laparoscopy. The patient was treated with a 4-day course of postoperative antibiotics and a surgical drain that was later removed who had a full recovery. We conclude that the appropriate workup includes CT imaging and treatment with laparoscopic surgery for removal of the appendix.
A 25-year-old man presented to the hospital with 1 week of abdominal pain especially with ambulation and decreased appetite. He had a temperature of 99 F, was tachycardic to 109 bpm, and found to be tender at McBurney’s point. Acute Care Surgery was consulted for possible acute appendicitis. Laboratory results on admission showed a leukocytosis of 12.02 × 109. With acute abdominal pain in the man, a CT abdomen pelvis with IV contrast was obtained and showed a 1.2 cm appendicolith in the proximal appendix with fluid-filled dilation of the distal appendix measuring up to 1.1 cm with moderate periappendiceal stranding consistent with a diagnosis of acute appendicitis.
The patient was started on antibiotics in the emergency department and was consented for the operating room. During laparoscopy, it was noted that the cecum was tethered to the pelvis and was difficult to elevate and visualize. The terminal ileum and base of the appendix were able to be viewed. The appendix was adherent to the pelvic sidewall and was divided at its base. A laparoscopic stapler and Ligasure [Covidien, Minneapolis, MN] were used to divide the base of the appendix from the cecum and the mesoappendix until the pelvic sidewall was reached. It was then realized that the appendix was completely incarcerated within the obturator canal. As much of the appendix was delivered that could be done safely, eventually separating at the tip. Blunt dissection was attempted to deliver the appendiceal tip which proved unsuccessful [Figure 1]. It was decided to place a 15 French Blake drain positioned at the dissection plan. The procedure was completed, and the patient tolerated it well. The appendix was removed and sent as a specimen with the fecalith. Intraoperative laparoscopic image of obturator hernia with arrow #1 obturator membrane, arrow #2 tip of appendix, and arrow #3 pubic bone.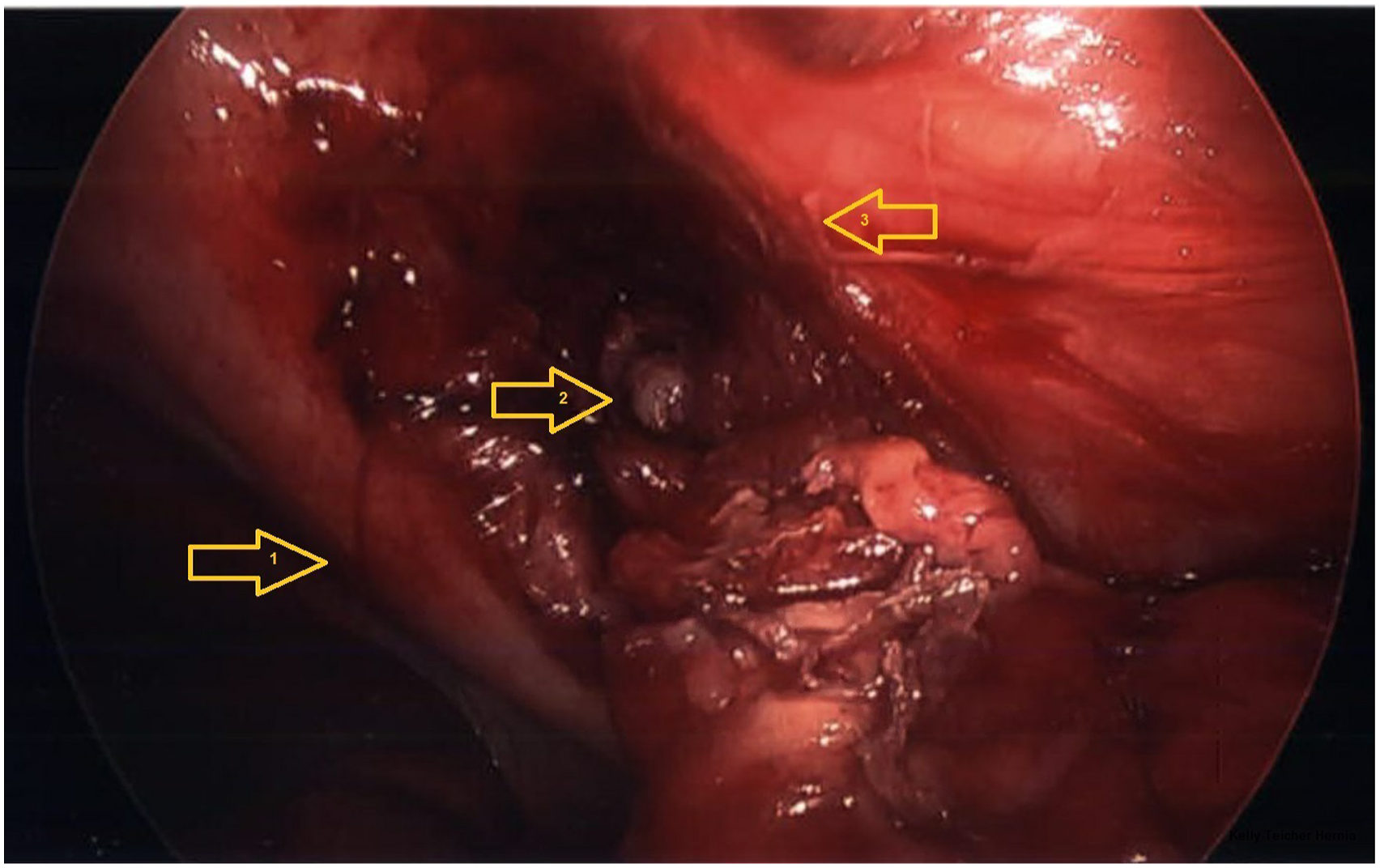
The patient did well postoperatively with an uncomplicated recovery. He was discharged on the first postoperative day with 20cc of serosanguinous output from the drain. He was treated with a 4-day course of antibiotics with ciprofloxacin and Flagyl. He followed up in clinic on postoperative day 8 with scant serous drainage in the drain which was removed in the office. He had an uneventful recovery and had returned to regular activities.
The surgical pathology report showed acute necrotizing appendicitis with periappendicitis and fecalith. The specimen confirmed the perforation at the tip of the appendix. The serosa was disrupted. The lumen measured .2 cm in diameter and contained hemorrhagic material and a fecalith.
Obturator hernias are a rare diagnosis with an incidence varying from .073 to <1% of all hernias. 1 It occurs with herniation through the obturator canal which contains the obturator vessels and nerve, bound by the obturator membrane, obturator and pectineus muscles inferiorly, and the pubic bone laterally and superiorly. Most cases occur in older, multiparous, emaciated women with a male to female ratio of 1:6-20 and a mean age of 70-90 years. They are up to twice as common on the right side possibly due to the position of the sigmoid colon on the left. 1 It is unusual to occur in a 25-year-old man. The most common clinical presentation of an obturator hernia is intestinal obstruction, with nausea, vomiting, abdominal pain, and distention. With these relatively acute symptoms, first-line treatment is prompt surgical intervention. 1
Even more rare are obturator hernias containing the appendix with only 5 prior cases found on our literature search.2-6 Although herniation of the appendix has been described in inguinal and femoral hernias, called Amyand and De Garengeot hernias, respectively, there is no eponym for a herniated appendix in an obturator hernia. If incarceration of bowel loops occurs, obstruction and subsequent symptoms follow acutely leading to prompt presentation and treatment. As seen with only 2 of the 5 prior cases, our patient presented with appendicitis while the other 3 cases presented with right thigh or groin pain and resulted in death postoperatively from septic shock.2-6 The appendix was resected to the extent that was possible with safe dissection. With the amount of inflammation, fecalith, and perforated appendix, the decision to leave a drain successfully treated the patient without postoperative abscess formation.
CT scan is the preferred imaging method for evaluating suspected obturator hernia.
1
It is also an acceptable image modality for suspected appendicitis. Although our patient’s CT imaging initially confirmed acute appendicitis with a fecalith, the obturator hernia was only appreciated at laparoscopy and later appreciated on imaging [Figure 2]. Only 1 of the 5 prior cases had a diagnosis of obturator hernia seen on CT imaging prior to the operating room, lending to this interesting problem.
3
A. Sagittal slice with arrow #1 showing fecalith with inflamed appendix and tracking into the obturator canal. B. Coronal slice showing inflamed tissue in the obturator canal at arrow #2.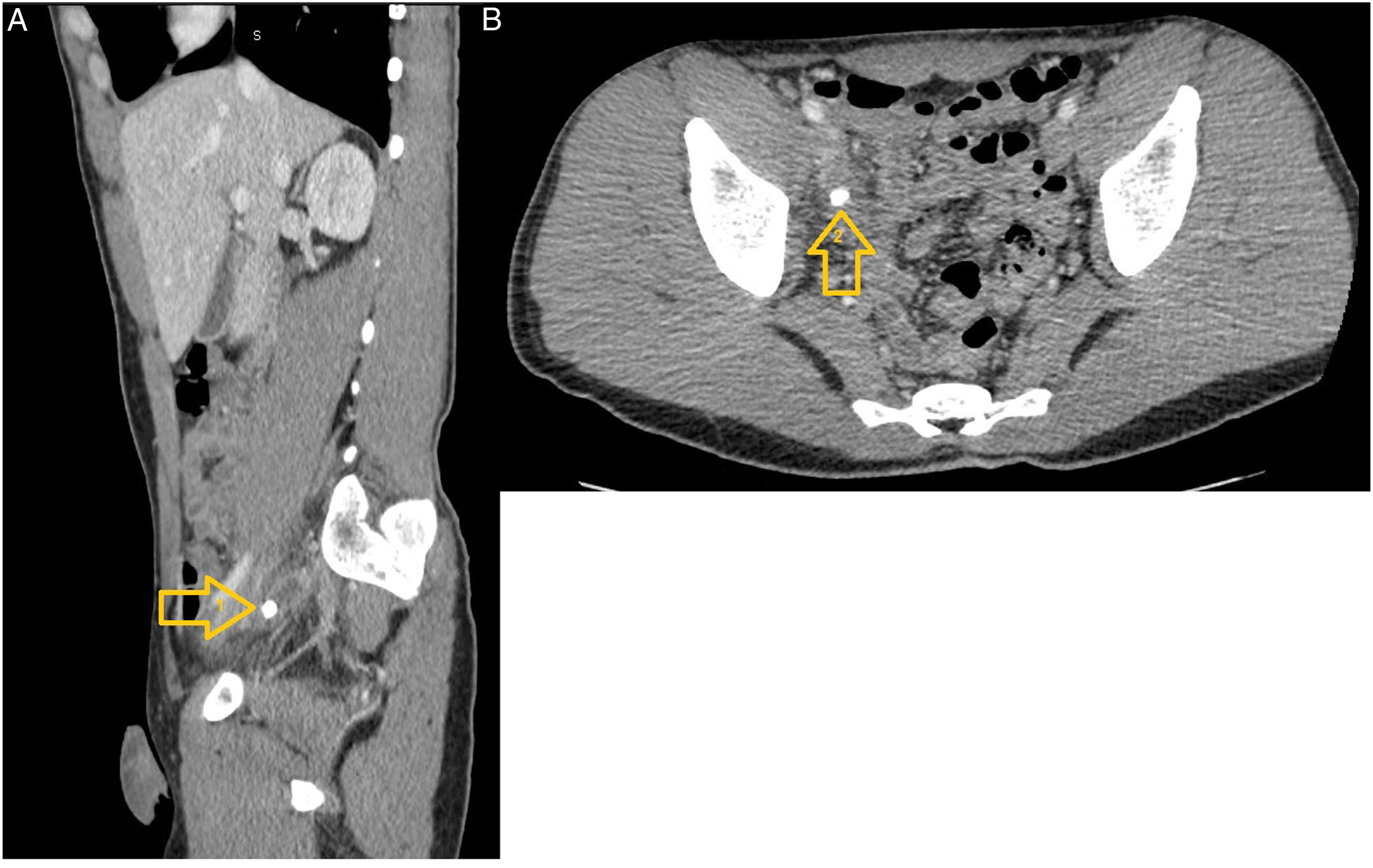
In conclusion, obturator hernias containing the appendix are exceedingly rare. CT imaging is appropriate as a diagnosing modality. As with our patient, laparoscopic approach is safe and appropriate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.