
Abstract
Hepatic injuries are common following blunt trauma and while frequently managed expectantly, biliary injury as a result of the trauma requires a high index of suspicion, a focused workup, and likely interventional treatment. A 44-year-old female with a history of Roux-en-Y gastric bypass presented after a ground level fall and was initially discharged home but represented with worsening abdominal pain and elevated liver enzymes. She was found to have a segment 5/6 biliary injury requiring laparoscopic-assisted transgastric endoscopic retrograde cholangiopancreatography with common bile duct stent placement. This case represents the difficulty of diagnosing biliary injuries following blunt trauma, and the need for advanced endoscopic interventions for treatment in patients with atypical anatomy.
Keywords
Hepatic injuries are one of the most common findings following blunt trauma. Although more frequently associated with abdominal trauma, patients with blunt thoracic trauma may also present with hepatic injuries. Rib fractures are considered a likely cause of thoracic trauma-associated hepatic injury; however, the number of rib fractures is not predictive of abdominal solid organ injury occurrence, and the clinical course following this injury pattern is variable. 1 Given the infrequent presentation of hepatic injury following thoracic trauma, it is important for clinicians to remain cognizant of this potentially devastating injury, as well as its associated complications.
A 44-year-old female with hypothyroidism and a remote surgical history of Roux-en-Y gastric bypass and cholecystectomy presented to the emergency department 1 day after experiencing a ground level fall at home. On arrival, she endorsed worsening pleuritic right-sided chest pain, but otherwise denied dyspnea, abdominal pain, nausea, or vomiting. Vital signs were unremarkable. Admission laboratory values were significant for mildly elevated alanine transaminase (ALT) and aspartate aminotransferase (AST) with a normal total bilirubin level, white blood cell count, and hemoglobin. Computed tomography of abdomen and pelvis without contrast identified multiple right-sided nondisplaced rib fractures and mild intrahepatic ductal dilatation of unclear etiology (Figure 1(A)). She was admitted to the trauma surgery service for observation and discharged home on post-trauma day (PTD) 2 in good condition. Serial cross-sectional imaging of liver injury. (A) CT A/P without contrast, axial view on PTD 1: mild intrahepatic dilatation and partially imaged right-sided nondisplaced rib fractures. (B) CT A/P with contrast, coronal view on PTD 2: laceration of right lobe of liver (dashed arrow). (C) CT A/P with contrast, axial view on PTD 6: large volume pelvic free fluid. (D) MRCP, axial view on PTD 6: parenchymal liver contusion with T2 laceration extending 5.8 cm in segment 5/6 (dashed arrow). Abbreviations: A/P, abdomen/pelvis; MRCP, magnetic resonance cholangiopancreatography; PTD, post-trauma day.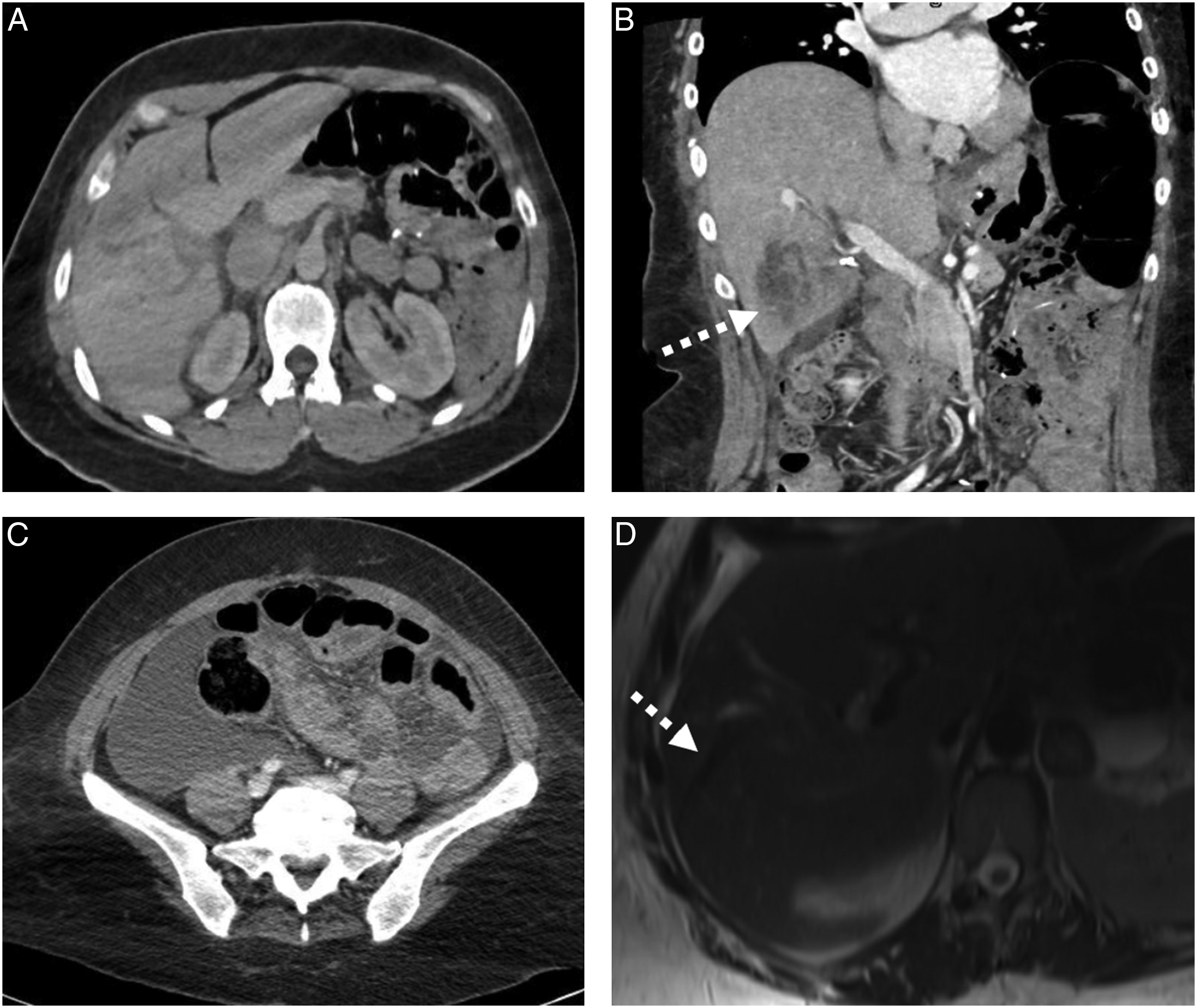
She presented to the emergency department on PTD 2 with sudden onset right-sided abdominal pain, as well as anorexia and increasing nausea. On physical exam, she endorsed right upper quadrant abdominal pain. She remained hemodynamically stable; however, repeat labs were notable for hyperbilirubinemia of 3.3 and elevated alkaline phosphatase, AST, and ALT. Hemoglobin was unchanged and within normal limits. Repeat CT abdomen and pelvis with contrast on PTD 2 was worrisome for a possible Grade IV liver laceration and pelvic free fluid but no active extravasation (Figures 1(B) and (C)). She was admitted to the trauma surgery service for expectant nonoperative management; however, over the next few days, she developed worsening abdominal pain and tachycardia. Subsequent magnetic resonance cholangiopancreatography (MRCP) on PTD 6 confirmed a 5.8 cm parenchymal laceration consistent with a Grade III/IV liver injury and large volume biliary ascites concerning for significant biliary injury in segment 5/6 (Figure 1(D)). There was no evidence of vascular injury. Endoscopic biliary stenting and abdominal washout were recommended jointly by the gastroenterology and surgical teams, but conventional endoscopic retrograde cholangiopancreatography (ERCP) was not feasible, given her history of Roux-en-Y gastric bypass. As a result, patient underwent successful laparoscopic-assisted transgastric ERCP with common bile duct stent placement via the remnant stomach, peritoneal washout, and drainage on PTD 7. Bile peritonitis was seen throughout the abdomen (Figure 2). She completed a 5-day course of intravenous Zosyn and was discharged home on PTD 10. Approximately 5 weeks after discharge, she underwent elective laparoscopic-assisted transgastric ERCP and stent removal and is recovering well. Intraoperative view during laparoscopic-assisted ERCP and washout. (A) Contrast leak visible during ERCP (dashed arrow). (B) Bilious ascites in the pelvis with associated peritonitis. (C) Loculated bilious ascites above the dome of the liver and parenchymal injury to right lobe of liver (dashed arrow). Abbreviation: ERCP, endoscopic retrograde cholangiopancreatography.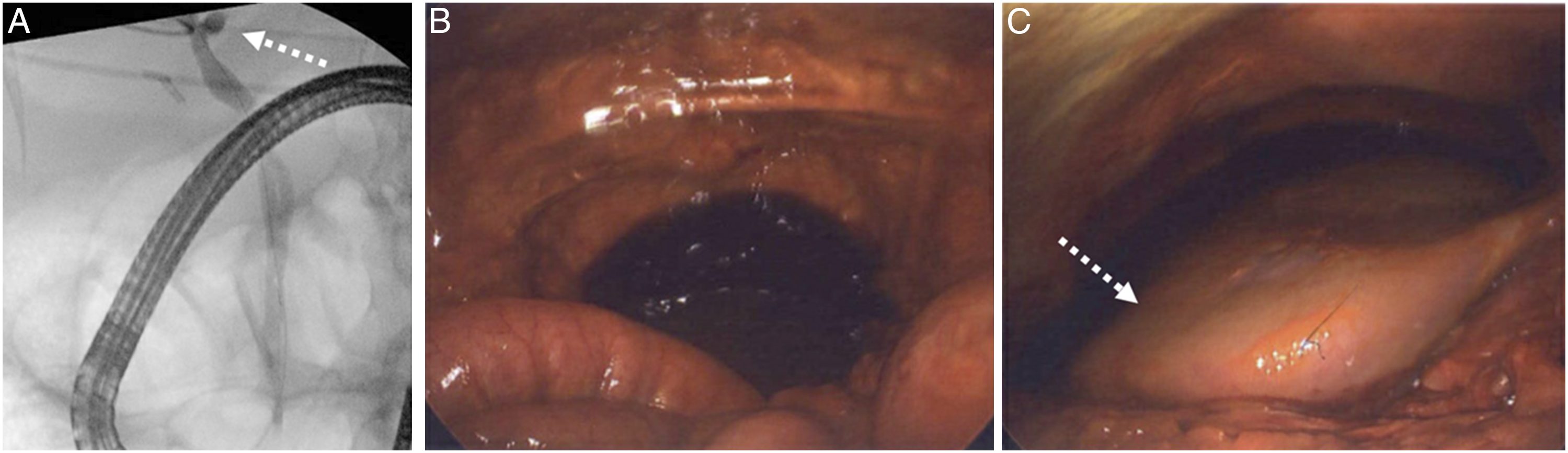
Hepatic injury following blunt trauma is often diagnosed with CT scan; however, there may be reduced suspicion for injury in low-impact and thoracic traumas. Patients who present with rib fractures should be assessed for abdominal injury. 1 Targeted lab work may assist clinicians in diagnosing occult injury as elevated liver function tests (LFTs) are frequently associated with liver injury. However, the degree of elevation in LFTs is not related to the degree of injury, 2 and additional workup may be necessary, such as hemoglobin monitoring and serial abdominal exams. If the patient fails to improve or suspicion of solid organ injury is high, further imaging such as contrasted CT scans, abdominal ultrasound, MRCP, or hepatobiliary iminodiacetic acid (HIDA) scan may be warranted to evaluate for vascular, parenchymal, or biliary injury.
In addition, blunt hepatic injuries are frequently managed nonoperatively, but patients may benefit from inpatient monitoring, especially for those with high grade injuries as the extent of initial injury is associated with complication risk. 3 For example, complications from high grade hepatic injuries, such as bleeding, infection, biliary leak or obstruction, are relatively common and occur in approximately 10% of blunt hepatic injury. 3 These complications can have detrimental effects on health care utilization and optimal patient recovery. Although post-traumatic bleeding is the most common and is often managed expectantly, clinicians must have a high index of suspicion for biliary disruption in the setting of stable hemoglobin, rising LFTs, and worsening abdominal pain because damage to the biliary system requires intervention.
Fortunately, ERCP and biliary stenting have been shown to be an effective treatment for biliary damage following severe liver injury. 4 Patients with a complicated surgical history, such as Roux-en-Y gastric bypass or reconstructive intestinal surgery, need advanced and highly trained endoscopists and may require transfer to a tertiary facility for definitive management. Early coordinated involvement of gastroenterology and surgery, however, may negate the need for transfer as laparoscopic-assisted ERCP, in which a small gastrotomy is made in the remnant stomach to facilitate access to the biliary tree, is effective in patients with disrupted anatomy. Finally, as seen in this patient, biliary injury may not be easily diagnosed, but left untreated can lead to peritonitis, deep infection, or sepsis, and require additional treatment such as abdominal washout, drainage, and antibiotics.
Blunt hepatic injury can occur after low-impact thoracic trauma, and the presence of rib fractures should be considered a risk factor. Nonoperative management of bleeding complications may be possible, but biliary injuries require early recognition and intervention to reduce patient morbidity. This case demonstrates the efficacy of multidisciplinary management of a surgically complicated patient with biliary injury as a result of blunt thoracic trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.