
Abstract
Background
Intestinal anastomoses in military settings are performed in severely injured patients who often undergo damage control laparotomy in austere environments. We describe anastomotic outcomes of patients from recent wars.
Methods
Military personnel with combat-related intra-abdominal injuries (June 2009-December 2014) requiring laparotomy with resection and anastomosis were analyzed. Patients were evacuated from Iraq or Afghanistan to Landstuhl Regional Medical Center (Germany) before being transferred to participating U.S. military hospitals.
Results
Among 341 patients who underwent 1053 laparotomies, 87 (25.5%) required ≥1 anastomosis. Stapled anastomosis only was performed in 57.5% of patients, while hand-sewn only was performed in 14.9%, and 9.2% had both stapled and hand-sewn techniques (type unknown for 18.4%). Anastomotic failure occurred in 15% of patients. Those with anastomotic failure required more anastomoses (median 2 anastomoses, interquartile range [IQR] 1-3 vs. 1 anastomosis, IQR 1-2, P = .03) and more total laparotomies (median 5 laparotomies, IQR 3-12 vs. 3, IQR 2-4, P = .01). There were no leaks in patients that had only hand-sewn anastomoses, though a significant difference was not seen with those who had stapled anastomoses. While there was an increasing trend regarding surgical site infections (SSIs) with anastomotic failure after excluding superficial SSIs, it was not significant. There was no difference in mortality.
Discussion
Military trauma patients have a similar anastomotic failure rate to civilian trauma patients. Patients with anastomotic failure were more likely to have had more anastomoses and more total laparotomies. No definitive conclusions can be drawn about anastomotic outcome differences between hand-sewn and stapled techniques.
Key Takeaways
15% of combat casualties who had at least one anastomosis had anastomotic failure with the time to failure being a median of 3 days post-injury. There was no significant difference in the technique used (hand-sewn vs. stapled), injury characteristics, or surgical site infections between the patients with and without anastomotic failure with the only significant factors being the number of total exploratory laparotomies and anastomoses. Despite higher severity with battlefield trauma, the proportion of anastomotic failure was similar to what was reported in civilian literature.
Introduction
The management of intestinal injury in combat settings has changed significantly over the past century. Dating back to World War I, nonintervention with selective primary repair was the preferred approach for gastrointestinal injuries. 1 More recently during the wars in Iraq and Afghanistan, damage control laparotomy with delayed primary anastomoses became commonplace. 2 Intestinal anastomoses in military settings are performed in severely injured patients who often undergo damage control laparotomy in austere environments. These patients commonly have a high associated burden of injury and are potentially at a greater risk of anastomotic complications. 3 Abdominal trauma represents approximately 10% of the injuries from the recent conflicts in Iraq and Afghanistan, with abdominal operations accounting for at least 13% of surgical procedures performed on combat casualties. 4
The anastomotic outcomes for civilian trauma and acute care surgery patients have been previously described.5-7 Leak rates vary from 6 to 15% and have similar outcomes between stapled and hand-sewn techniques. While there exists a debate in elective civilian cases whether stapled intestinal anastomoses are more cost-effective than hand-sewn anastomoses, 8 no differences in outcomes between the two techniques have been demonstrated. 9 The anastomotic outcomes in military settings from the wars in Iraq and Afghanistan have not yet been described. Herein, we sought to characterize the outcomes of anastomoses performed in military settings and determine if any differences exist between the techniques used.
Methods
This study was approved by the Institutional Review Board (IRB) of the Uniformed Services University of the Health Sciences (Bethesda, MD). Data were collected through an IRB-approved waiver of consent for use of de-identified data not obtained through interaction or intervention with human subjects. Data were collected as part of the Trauma Infectious Disease Outcomes Study (TIDOS), an observational study of infectious complications in combat casualties.10,11 Criteria for inclusion in TIDOS were being active-duty or Department of Defense beneficiary, age 18 years or older, being injured while deployed (June 1, 2009-December 31, 2014), and requiring medical evacuation to Landstuhl Regional Medical Center before transition to participating military hospitals in the United States. The participating hospitals are Walter Reed National Military Medical Center (previously was Walter Reed Army Medical Center and National Naval Medical Center prior to September 2011) and Brooke Army Medical Center. For this study, the population was restricted to military personnel with combat-related intra-abdominal injuries requiring laparotomy with intestinal resection and anastomosis.
Patient demographics (ie, age at injury and sex), injury characteristics (ie, Injury Severity Score [ISS] and mechanism of injury), and early trauma care data (ie, blood transfusion and shock index) were collected from the Department of Defense Trauma Registry (DoDTR), 12 while infection-related information (ie, surgical site infections [SSIs]) was obtained through the DoDTR TIDOS Infectious Disease module. 10 Data related to abdominal surgery (ie, laparotomy, anastomoses, and abdominal organ injury) and outcomes were retrospectively abstracted from medical records. Particular attention was paid to the anastomotic technique used where this information was available. In addition to visualized anastomotic breakdown, anastomotic failure was defined as the presence of intra-abdominal abscess, enterocutaneous fistula, or subsequent intraperitoneal spillage deemed to be related to anastomotic leak. Retrospective review of clinical findings, medical records, imaging, and laboratory results were utilized to classify abdominal SSIs as superficial, deep incisional, or organ space, as previously described. 13
Chi-squared or Fisher’s exact tests were used to detect differences between patients with and without anastomotic failure for categorical variables, and the Kruskal-Wallis test was used for continuous variables. A P value <.05 was deemed statistically significant. Statistical analysis was performed using SAS version 9.4 (Cary, NC).
Results
Study Population
Characteristics of Combat Casualties Undergoing Intestinal Anastomosis During Exploratory Laparotomy.
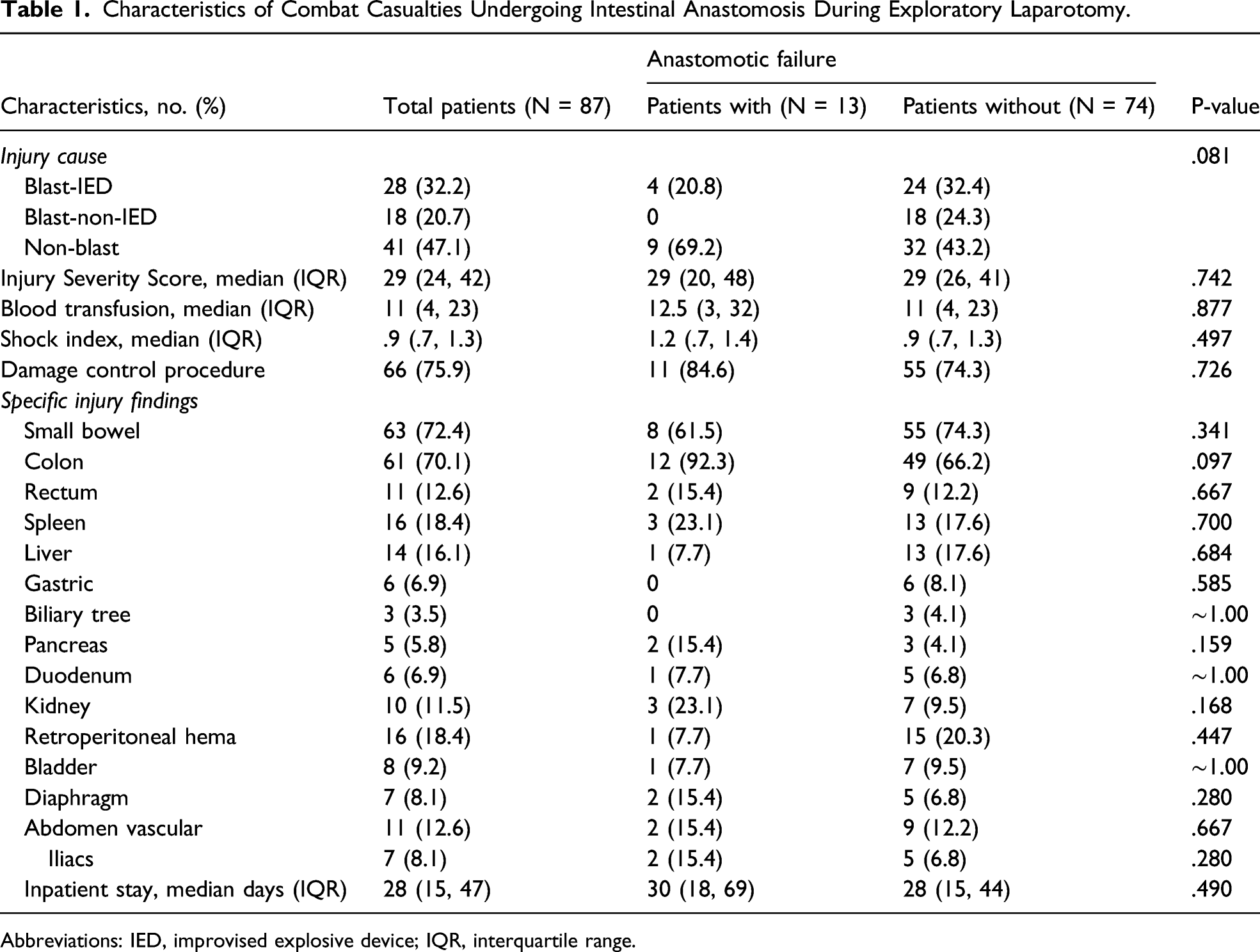
Abbreviations: IED, improvised explosive device; IQR, interquartile range.
Anastomotic Characteristics and Outcomes
Anastomotic Characteristics and Outcomes.
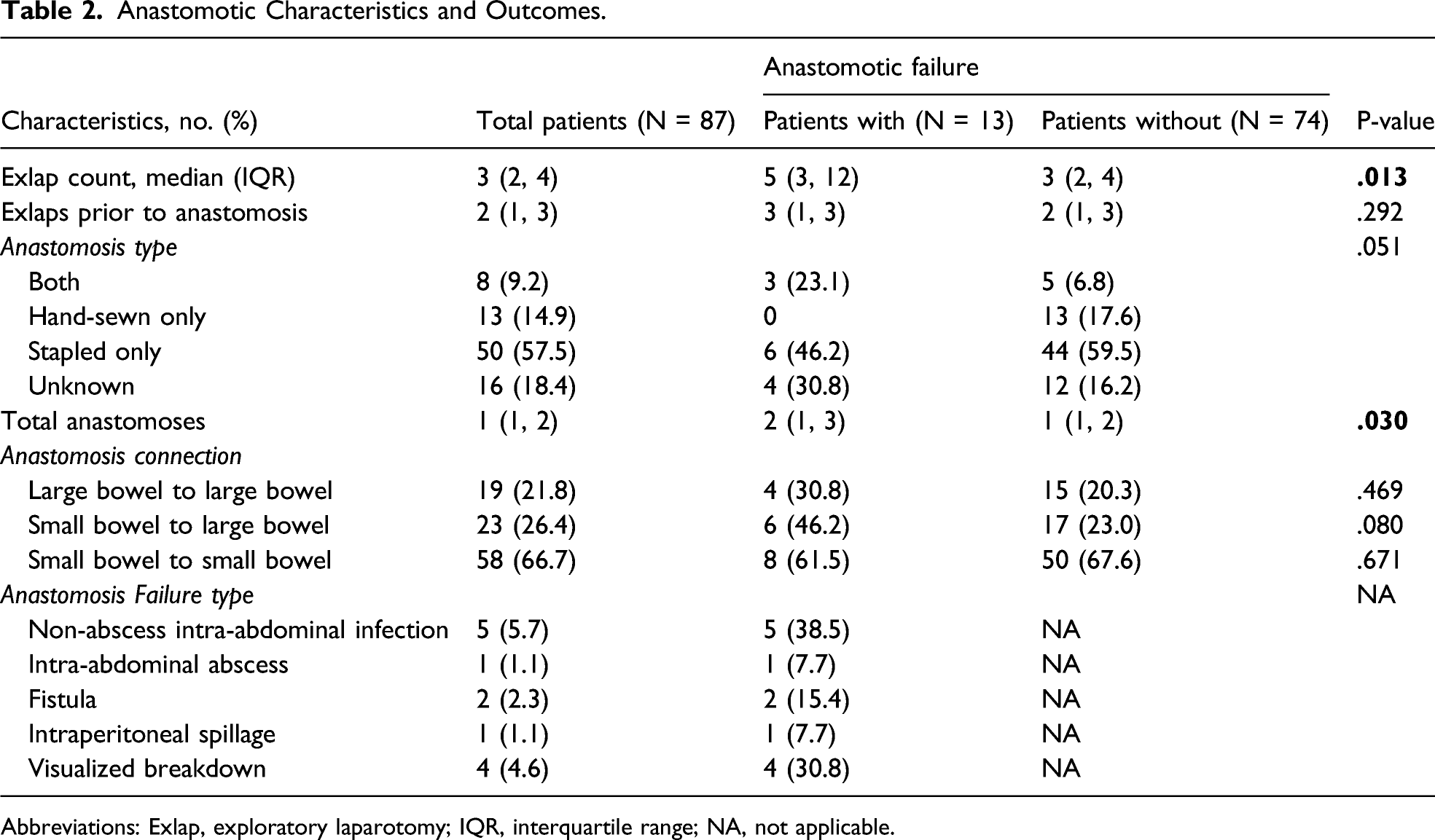
Abbreviations: Exlap, exploratory laparotomy; IQR, interquartile range; NA, not applicable.
Time to anastomotic failure was a median of 3 days post-injury (IQR: 2-6 days). Of the 13 patients with anastomotic failure, 1 (7.7%) had an associated intra-abdominal abscess, 5 (38.5%) developed a non-abscess intra-abdominal infection, 2 (15.4%) developed an enterocutaneous fistula, 1 (7.7%) had intraperitoneal spillage, and 4 patients (30.8%) had visualized breakdowns on subsequent laparotomies. Those who had an anastomotic failure were more likely to have multiple anastomoses (median 2 anastomoses, IQR 1-3 vs. 1 anastomosis, IQR 1-2, P = .03) and required more total laparotomies (median 5 laparotomies, IQR 3-12 vs. 3, IQR 2-4, P=.01).
Outcomes of Patients Stratified by Occurrence of Anastomotic Failure.
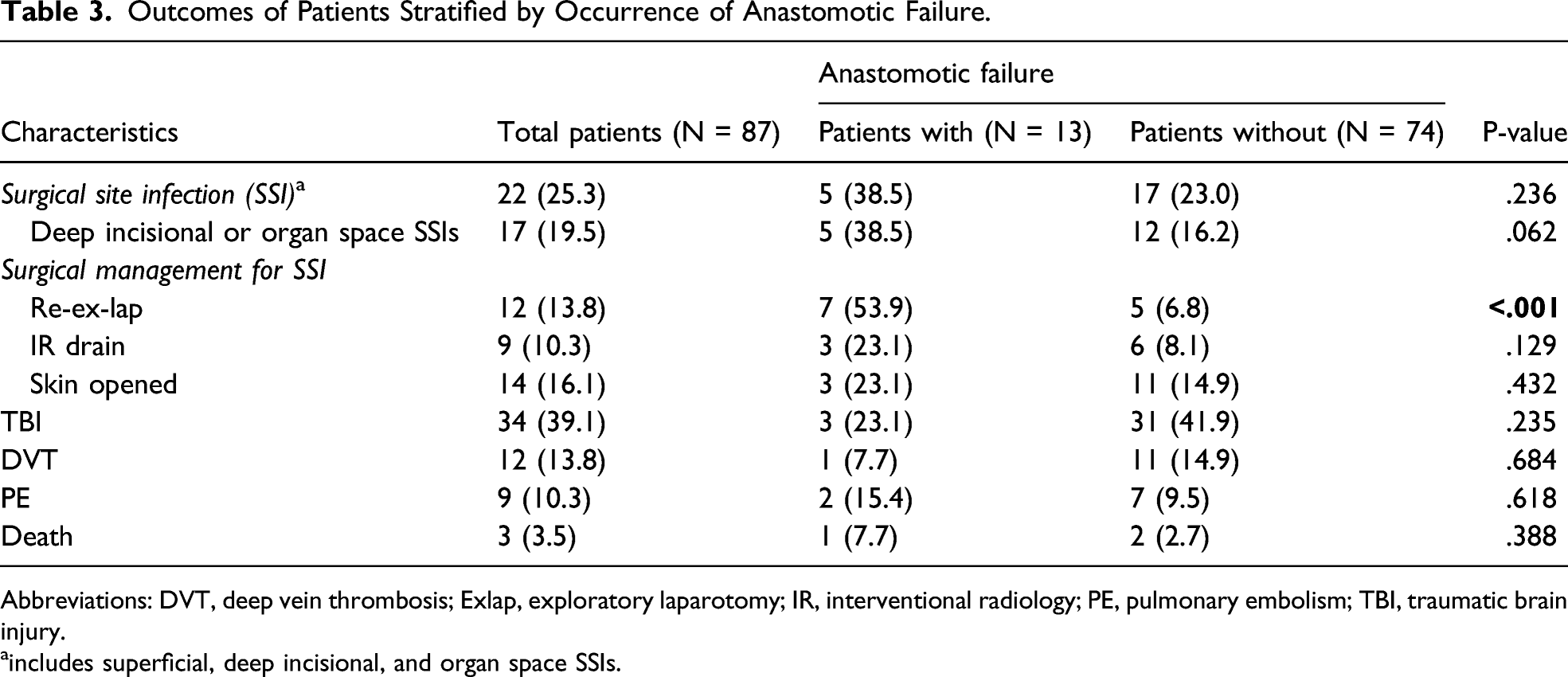
Abbreviations: DVT, deep vein thrombosis; Exlap, exploratory laparotomy; IR, interventional radiology; PE, pulmonary embolism; TBI, traumatic brain injury.
aincludes superficial, deep incisional, and organ space SSIs.
Discussion
This retrospective study on the anastomotic outcomes of recent military laparotomies demonstrated that patients with anastomotic failure in this series were more likely to have had a greater number of laparotomies as well as anastomoses. No leaks were seen in those who had hand-sewn only anastomoses, although this was not a statistically significant difference. Therefore, we did not see any notable outcome differences between stapled and hand-sewn technique.
In this military population, we observed a similar leak rate to anastomoses reported in civilian settings. Brundage et al 6 described a leak rate of 13% for stapled anastomoses and 5% for hand-sewn that was not statistically significantly different. In addition, a study of penetrating colon injuries found that 6.3% of stapled colorectal anastomoses leaked compared to 7.8% of hand-sewn anastomoses (P = .69). 7 Furthermore, Bruns et al 5 reported a leak rate of 15.4% for hand-sewn anastomoses and 10.6% for stapled anastomoses in an assessment of civilian acute care surgery patients. Despite the military patients in our study being generally more severely injured, our leak rate was comparable to these prior civilian studies. In particular, the mean ISS for two of the previously described series comprising trauma patients was 16.5 and 21.9, respectively.6,7 In our study, the median ISS was 29, which is slightly higher as compared to a prior series of military patients where the median ISS was 25 for those who underwent therapeutic laparotomy from 2002 to 2011. 14 An in-theater evacuation time of 60 minutes or less was mandated in June 2009, 15 and this may have accounted for why more severely injured patients were reported in our study. The overall burden of injury due to the high prevalence of blast injuries (53%) also likely contributed to the anastomotic outcomes of our patients.
Although there was no statistical difference in the proportion of SSIs, whether assessing all SSIs or restricting to deep incisional/organ space SSIs, between patients who leaked and who did not in our study, there does appear to be a higher incidence of abdominal SSIs in military patients who undergo intestinal anastomosis. Abdominal SSIs have previously been described in a broader series of military laparotomies using the TIDOS population. As noted by Bozzay et al, 14.4% of 341 combat casualties who underwent combat-related exploratory laparotomies developed an abdominal SSI with the majority being organ space or deep incisional (12.0%).13,16 In this more restricted TIDOS population, the overall proportion of any SSIs was 25.3%, while it was 19.5% for either deep incisional or organ space SSIs and it is possible that distinguishing a true meaningful difference regarding the development of abdominal SSIs between the groups was hindered by the low numbers included in the study.
Over 90% of patients in our study had an open abdomen during the course of their care, and the median number of exploratory laparotomies prior to anastomosis was two. Furthermore, approximately 76% of patients had damage control procedures performed. This compares to the 77% incidence of damage control laparotomies reported in Smith et al. 2 While there was not an association in our study with having had an open abdomen and experiencing anastomotic leak, we did find that patients with anastomotic failure more frequently had a greater number of both anastomoses and laparotomies. Significant consequences, of course, are associated with anastomotic failures. Beyond the infectious complications and need for further intervention, anastomotic leaks likely play a role in contributing to the high rate of incisional hernias after military laparotomies, which is estimated to be as high as 19.1%. 17
This study does include limitations inherent with retrospective analyses. Additionally, incomplete or missing documentation for patients as they were transferred through different levels of care also contributed to a small number of patients for which the technique of anastomosis was not known. Last, complete follow-up information was not available for some patients.
Operations performed in the forward deployed environments are at times limited by the supplies that are available. Thus, combat surgeons should be adept at being able to perform both hand-sewn and stapled anastomotic techniques. Overall, the results of this study support that combat surgeons should be able to perform intestinal anastomoses with the technique best supported by their patient’s clinical circumstances, resources available, and prior training.
Footnotes
Acknowledgments
We are indebted to the Infectious Disease Clinical Research Program Trauma Infectious Disease Outcomes Study team of clinical coordinators, microbiology technicians, data managers, clinical site managers, and administrative support personnel for their tireless hours to ensure the success of this project.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work (IDCRP-024) was provided by the Infectious Disease Clinical Research Program (IDCRP), a Department of Defense program executed through the Uniformed Services University of the Health Sciences, Department of Preventive Medicine and Biostatistics through a cooperative agreement with The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF). This project has been funded by the National Institute of Allergy and Infectious Diseases, National Institutes of Health, under InterAgency Agreement Y1-AI-5072, the Defense Health Program, U.S. DoD, under award HU0001190002, and the Department of the Navy under the Wounded, Ill, and Injured Program (HU0001-10-1-0014). The funders had no role in study design, data collection, data analysis, data interpretation, or writing the manuscript.
Disclaimer
The views expressed are those of the authors and do not reflect the official views of the Uniformed Services University of the Health Sciences, Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the National Institute of Health or the Department of Health and Human Services, Brooke Army Medical Center, Walter Reed National Military Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of Defense, or the Departments of the Army, Navy or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.