
Abstract
Background
Computed tomography (CT) has emerged as the diagnostic modality of choice in trauma patients. Recent studies suggest its use in hemodynamically unstable patients is safe and potentially lifesaving; however, the incidence of adverse events (AE) during the trauma CT scanning process remains unknown.
Study Design
Over a 6-month period at a Level 1 trauma center, data on patients undergoing trauma CT (whole-body CT (WBCT) +/− additional CT studies) were prospectively collected. All patients requiring a trauma team activation (TTA) were included. Adverse events and specific time intervals were recorded from the time of TTA notification to the time of return to the resuscitation bay from the CT suite.
Results
Of the 94 consecutive patients included in the study, 47.9% experienced 1 or more AE. Median duration away from the resuscitation bay for all patients was 24 minutes. Patients with AE spent a significantly longer time away from the resuscitation bay and had longer scan times. Vasopressor support and ongoing transfusion requirement at the time of CT scanning were associated with AE.
Conclusion
Adverse events of varying clinical significance occur frequently in patients undergoing emergent trauma CT. A standard trauma CT protocol could improve the efficiency and safety of the scanning process.
Introduction
The use of computed tomography (CT) has increased steadily since the early 2000s due, in part, to its role as the imaging modality of choice for trauma patients.1,2 While current Advanced Trauma Life Support (ATLS) recommendations advocate for selective imaging, whole-body CT (WBCT) protocols are now widely implemented throughout the United States and internationally.3-8 As the use of WBCT has expanded, so too have the performing criteria. A large multicenter retrospective study challenged the idea of hemodynamic instability as a contraindication by demonstrating a significant survival benefit in patients who presented with moderate or severe shock and underwent WBCT as part of the initial workup. 9 More recent retrospective studies from Japan and Columbia have shown similar findings.10,11 While the results of these studies are encouraging, many of the included centers have CT scanners incorporated in the resuscitation bays or have access to portable scanners which can be wheeled in without the need for patient transport. This technology has yet to reach widespread use in the United States, where the concept of imaging unstable patients remains an ongoing debate.
Even in the absence of hemodynamic instability, the transport and imaging of severely injured patients who are often intubated and undergoing active resuscitation remain a challenge. Outside of the resuscitation bay, access to airway supplies, blood products, sedatives, or vasoactive medications is limited. Once in the CT suite, the transfer and subsequent scan time without direct bedside presence of the trauma team present several opportunities for complications. Prior studies describing adverse events (AE) during this critical time period are limited, and the majority are retrospective in nature.5,8-10,12 The purpose of this study was to assess the duration of the CT scanning process in polytrauma patients and the incidence of AE during this period. In addition, we sought to identify clinical factors associated with AE.
Methods
This is a retrospective review of data collected as part of a lean improvement initiative. The study was approved by the Institutional Review Board at the University of Southern California (USC). Consecutive trauma patients who met specific prehospital criteria for a trauma team activation (TTA) and who underwent an emergent trauma CT after the secondary survey were included between October 1, 2017 and March 31, 2018. Trauma CT was defined as WBCT (non-contrast CT head and cervical spine, repositioning of the arms to above the shoulders, arterial phase CT of the chest and upper abdomen, and a portal venous phase from the diaphragm to the lower pelvis) in addition to any other CT studies performed as part of the same imaging sequence. All scans were performed on a Toshiba 64-slice multidetector CT scanner.
The CT scanning process for TTA patients was mapped from the time of TTA notification to the time of return to the resuscitation bay from the CT suite. The CT suite is located adjacent to the resuscitation bay at our institution. Upon mapping this process, we identified the following 7 points at which times were to be recorded for each patient: Trauma team activation notification, patient arrival, end of secondary survey, leave resuscitation bay, CT scan start, CT scan end, and return to resuscitation bay.
Our primary outcome was the total duration of the scanning process. All time and AE data were collected in real time. In addition to time data, we collected variables including patient demographics, admission vital signs including Glasgow Coma Scale (GCS), injury data (mechanism and Injury Severity Score [ISS]), risk factors potentially associated with AE (mechanical ventilation, use of sedatives/muscle relaxant, vasopressor or transfusion requirement, activation of massive transfusion protocol, or resuscitative endovascular balloon occlusion of the aorta [REBOA]), and in-hospital mortality. Adverse events were defined as endotracheal (ET) tube kinking or dislodging, peripheral or central intravenous (IV) access issues (inadequate type, size, or location of the catheter, inadvertent removal, and contrast extravasation), agitation requiring medical treatment and/or restraints, new onset of hypotension during the CT scanning process (systolic blood pressure < 90 mmHg), arrhythmia identified on the portable monitoring device, incorrect CT orders, interruption of the scan, or if the scanner was occupied at the time of patient transport.
Patients were divided into 2 groups: AE and no-adverse events (no-AE). Descriptive statistics were used to summarize demographics, vital signs, injury data, and outcomes. Categorical variables were reported as numbers and percentages. Continuous variables were reported as medians with interquartile range (IQR). Univariate comparisons were made using Mann-Whitney U test for continuous variables and chi-square or Fisher’s exact test for categorical variables. We considered P values less than .05 to be significant. Statistical analysis was performed using SPSS, version 23.0.
Results
Demographics and Time Intervals of Patients Undergoing Trauma CT.
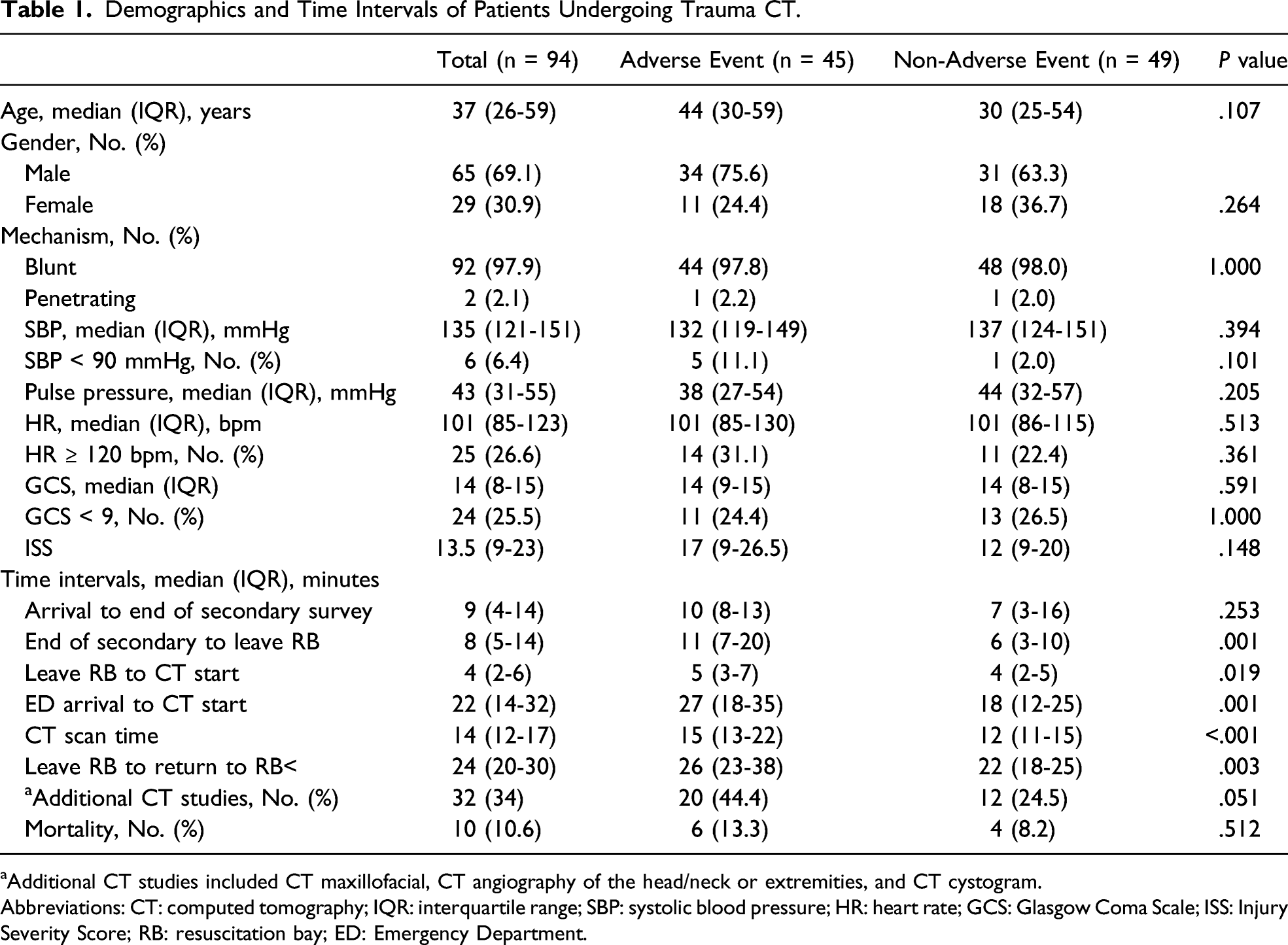
aAdditional CT studies included CT maxillofacial, CT angiography of the head/neck or extremities, and CT cystogram.
Abbreviations: CT: computed tomography; IQR: interquartile range; SBP: systolic blood pressure; HR: heart rate; GCS: Glasgow Coma Scale; ISS: Injury Severity Score; RB: resuscitation bay; ED: Emergency Department.
Incidence of Adverse Events During Trauma CT.
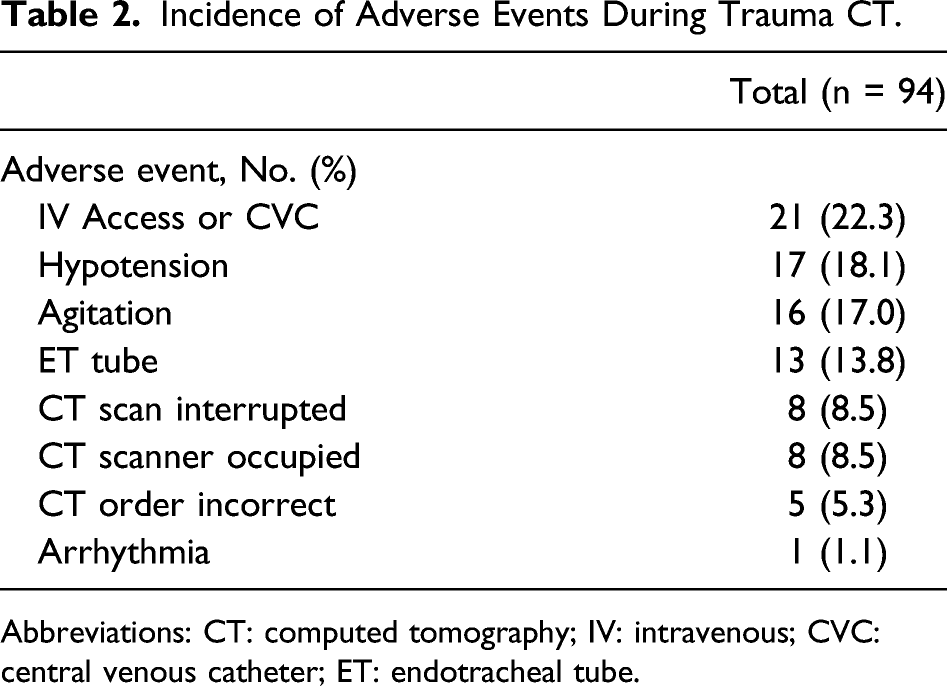
Abbreviations: CT: computed tomography; IV: intravenous; CVC: central venous catheter; ET: endotracheal tube.
Adverse Events During Trauma CT Stratified by Clinical Risk Factor.
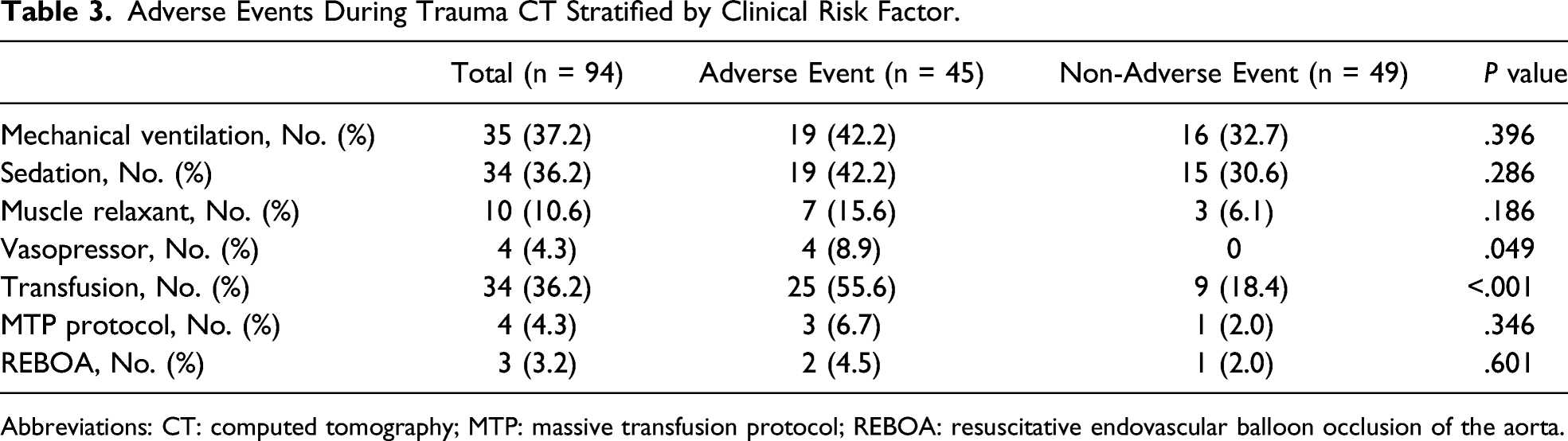
Abbreviations: CT: computed tomography; MTP: massive transfusion protocol; REBOA: resuscitative endovascular balloon occlusion of the aorta.
Discussion
In the current study, we reviewed prospectively collected data from 94 trauma patients who met TTA criteria and underwent an emergent trauma CT. Our findings indicate that a longer duration away from the resuscitation bay is associated with more AE. Patients receiving vasopressor support at the time of transfer to the CT suite or those requiring ongoing blood product transfusion had the highest incidence of complications. In certain high acuity cases, patients were away from the resuscitation bay for upward of 38 minutes.
The first large study to assess WBCT in hemodynamically unstable patients included 6101 trauma patients with moderate or severe shock, of which 3498 (57%) underwent WBCT. 9 When compared to similar cohorts who did not undergo WBCT, they observed a significant mortality benefit for both categories of shock in favor of WBCT. The authors concluded that this imaging modality is safe, feasible, and justified as long as it performed quickly and in an experienced trauma center. A more recent retrospective, single-center study assessing the use of CT in hemodynamically unstable patients with blunt and penetrating injuries found no mortality difference between those who were taken straight to the operating room and those who were first taken to the CT suite prior to admission or operative intervention. Of the 80 patients (47%) in the CT group, they reported no episodes of cardiac arrest or death in the CT scanner. 10 A limited number of other studies involving mostly stable trauma patients have described rates of AE while scanning from 0 to 1%.5,8,12 In contrast, our findings revealed an AE in 47.9% of TTA cases. This must be interpreted within the context of our defined AE, as non-life-threatening complications were also included.
An important factor in determining whether to subject an unstable patient to diagnostic imaging is the rapidity in which it can be performed. In the present series, patients were away from the resuscitation bay for a median of 24 minutes (20-30), and those noted to have an AE were away for a longer period of time when compared to those without any events recorded. It is unclear whether this was due to extra time required to address the event or whether the events were the result of being away from critical resources in the resuscitation bay. In our institution, the CT suite is located adjacent to the resuscitation bay, allowing for short transport times. The median scan time was 14 minutes, which is within the reported range in the literature for a non-contrast CT of the head and neck followed by a contrast scan of the chest, abdomen, and pelvis.13-15 This is, however, an area where potential time saving interventions can be implemented, as the AE group had significantly longer scan times. It also represents the period during which the patient is arguably at most risk given the lack of direct bedside access and limited equipment or medications necessary for escalation of care. Several studies have examined techniques which reduce overall scan time.15-20 Since Ptak et al first described a three-minute WBCT using a single-pass protocol, others have similarly demonstrated shorter scan times using this method when compared to conventional segmented protocols without significant compromise in image quality.16,18,20 Others have shown quicker scan times when eliminating patient arm repositioning between the head and torso series; however, consensus is lacking on whether this significantly alters image quality.15,19 Regardless of the exact specifications, the existence of a standardized protocol can likely improve efficiency and potentially affect outcomes.
It is worth highlighting that our study included AE which were not patient related and thus did not present a direct risk of harm, but merely increased time from arrival to diagnosis. These included incorrect CT orders, delay in CT availability, and interruptions during the CT scanning process. Issues with peripheral or central IV access occurred in 22.3% of all cases and represented the most common AE. This is after ensuring all patients had adequate IV access prior to transport as is standard at our institution. Malfunctioning peripheral IVs can lead to contrast extravasation or simply a delay in completing the scan if occluded; however, loss of central venous access in a patient undergoing large volume resuscitation can have significant effects on patient outcome. Hypotension occurred in 37.8% of cases in the AE group and in 1 patient was associated with arrhythmia. These events were captured on the portable monitoring device which accompanies all patients during transport. Issues related to the ET tube (13.8%) and agitation (17%) were also relatively common among all cases. Collectively, these AE represent a wide range on the spectrum of issues encountered during the transport and imaging of severely injured patients with variable potential morbidity.
Throughout the CT scanning process, certain precautions can be considered to mitigate the risk of AE. 8 This begins with the ultimate decision of whether to proceed to the CT suite rather than the operating room or interventional radiology suite depending on the patient’s overall clinical status—a question which has been debated extensively and must be taken on a case-by-case basis.9,21-23 Once the decision has been made to proceed with imaging, we advocate for ensuring adequate pressure-rated IV access prior to transfer. Members of the trauma, emergency department, and respiratory therapy teams should accompany the patient to the CT suite along with a portable monitoring device. Lines should be accounted for and secured during transfer to the scanning table. The monitoring device should be positioned in full view of the providers while the scan is ongoing. As described in the American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) Best Practice Guidelines in Imaging, radiology suites should be equipped with emergency airway supplies and suction devices as well as vasoactive, sedative, and paralytic medications. 7 Scanning should proceed according to a standardized protocol so that all personnel involved are well versed, and disposition should take place as quickly as possible.
The following study limitations must be acknowledged. While prospectively collected, we relied on the accuracy of documentation by different members of the trauma team. Along these lines, we attempted to reduce inconsistency by providing pre-specified definitions for AE; however, these were subject to individual interpretation. Finally, the layout of the ED and the proximity of the CT suite to the resuscitation bay is institution dependent. Despite these limitations, we believe our findings highlight the importance of ensuring safe imaging practices, especially when treating severely injured patients. Our next task is to modify our existing protocol and perform a follow-up study to assess how these changes affect the number of AE and the duration of the scanning process. Similar quality improvement studies at other trauma centers could help create the foundation for evidence-based guidelines, which currently do not exist.
Conclusions
Injured patients undergoing trauma CT on arrival are at risk for a number of AE during transport and imaging. Those requiring vasopressor support and blood product transfusion were significantly more likely to experience AE. The trauma CT scanning process, as a whole, can require a prolonged duration during which patients are away from the resuscitation bay.
Footnotes
Acknowledgments
The authors would like to thank Disha Jariwala, Christine Khabbaz, Fernando Lucchini, Ani Misirian, Caitie Reck, and David Belson, PhD from the University of Southern California Viterbi School of Engineering for their support in conducting this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.