
Abstract
Objective
The present study conducted a meta-analysis to forecast the risk factors associated with level-VII lymph node metastases in case of thyroid neoplasms, intending to assist in determining the requirement for level-VII lymph node lymphadenectomy during the surgery.
Methods
Electronic databases, PubMed, Embase, the Cochrane Library, CNKI, Wanfang Data, VIP, and CBM electronic databases were searched for studies focused on level-VII lymph node metastases in thyroid neoplasms, published up to April 2021. Stata 13.1 software was used for analyses.
Results
The literature search identified a total of 997 studies. Among these, 8 studies, involving 1813 patients, were included in the present case. All these studies were case-control studies. Results for meta‐analysis showed that male (OR = 1.340, 95% CI: 1.018-1.764, P = .037), age < 45 years (OR = 4.178, 95% CI: 1.601–10.908, P = .003), tumor size ≥ 2.0 cm (OR = 1.960, 95% CI: 1.079-3.562, P = .027), extrathyroidal extension (OR = 2.037, 95% CI: 1.578-2.630, P < .001), distant metastasis (OR = 2.775, 95% CI: 2.005-3.840, P < .001), central lymph node metastasis (OR = 3.500, 95% CI: 1.127-10.874, P = .03), contralateral cervicolateral metastasis (OR = 2.119, 95% CI: 1.514-2.965, P < .001), and bilateral nodal metastasis (OR = 4.651, 95% CI: 2.697-8.020, P < .001) acted as risk factors for level-VII lymph node metastases. In addition to this, sensitivity analyses and bias test showed that the results of meta‐analysis were reliable and stable and involved no publication bias.
Conclusion
In the present study, male gender, age < 45 years, tumor size ≥ 2.0 cm, extrathyroidal extension, distant metastasis, central lymph node metastasis, contralateral cervicolateral metastasis, and bilateral nodal metastasis were identified as risk factors for level-VII lymph node metastases in case of thyroid neoplasms.
Introduction
According to the latest update on global cancer burden, thyroid cancer ranked ninth in terms of cancer incidence in 2020. Concerning new numbers, it accounted for 3% of global incidence. 1 Thyroid cancer is generally prone to regional lymph node metastasis (LNM). Incomplete lymphadenectomy has been shown to increase the postoperative recurrence rate. Level-VII lymph node metastases, also known as upper mediastinal lymph nodes, are located behind the sternum and represent the extension of central lymph node metastasis. 2 Lymphadenectomy of the upper mediastinal lymph node is usually more complicated, primarily owing to its lower location. In cases where no obvious metastasis is reported/observed in preoperative imaging, lymphadenectomy of the upper mediastinal lymph node is generally not necessary. Previous studies have shown that upper mediastinal lymph node metastasis is usually not associated with a poor prognosis. However, it was found to be related to tumor recurrence.3,4 Therefore, there is an urgent need to define the risk factors associated with level-VII lymph node metastases in case of thyroid neoplasms. Besides this, it must be determined whether it is important/essential to perform lymphadenectomy of the upper mediastinal lymph node during the surgery. However, the significance of such investigation in clinical guidance is limited, primarily owing to the limitation of the studies and discrepancy in the results obtained for risk factors of the disease. The present study conducted a meta‐analysis of relevant studies that fulfilled the inclusion criteria and systematically evaluated the risk factors associated with level-VII lymph node metastases in thyroid neoplasms. The results of the study would further assist in determining the requirement for level-VII lymph node lymphadenectomy during the surgery.
Materials and Methods
Data Sources and Search Strategy
Data searches of the PubMed, Embase, the Cochrane Library, CNKI, Wanfang Data, VIP, and CBM electronic databases were performed using specific criteria for each database published until April 2021. The search subjects included thyroid neoplasms, mediastinal lymph node, and neoplasm metastasis. The retrieval method used was a combination of subject headings (MesH table) and free terms, for example, “thyroid neoplasms,” “thyroid carcinoma,” “mediastinal lymph node,” and “neoplasm metastasis” among others.
Diagnosis Criteria
The following were the diagnostic criteria for this study: (1) Confirmed thyroid cancer through postoperative pathology, including differentiated thyroid cancer, undifferentiated thyroid cancer, and medullary thyroid carcinoma. (2) Diagnostic criteria for level-VII lymph node established by the American Otolaryngology-Head and Neck Surgery and Oncology Committee (AAO-HNS): Level-VII lymph node metastases, also known as the upper mediastinal lymph node, are the extension of the central lymph node metastasis. The upper boundary is at the level of the sternal notch, the lower and the right boundaries form the upper rim of the innominate artery, the left boundary forms the medial rim of the left common carotid artery, the anterior boundary forms the sternal stem, and the posterior boundary forms the pre-vertebral fascia and the outer wall of the trachea. 2
Inclusion Criteria and Exclusion Criteria
The patient inclusion criteria included the following: (1) publicly published case-control studies with complete data; (2) the experimental group of the case-control studies included thyroid cancer patients with exposure factors; and the control group included patients without exposure factors. The included literature involved at least 2 exposure factors; (3) the outcome was measured by using odds ratio (OR) and 95% confidence interval (95% CI); and (4) the literature language was either Chinese or English.
The patient exclusion criteria include the following: (1) case reports, editorials, reviews, and fundamental investigation; (2) abstracts without full text; (3) low quality of the literature ((NOS) score <5 points); (4) repeated publications or studies with overlapping subjects; and (5) OR value and 95% CI of the exposure factors not obtained from the literature.
Definition and Grouping of Exposure Factors
Definition and grouping of the exposure factors: (1) Gender (male or female); (2) age (<45 years or ≥45 years); (3) tumor size (≥ 2.0 cm or <2.0 cm); (4) extrathyroidal extension (present or absent); (5) multifocality (single or multifocal); (6) lymphovascular invasion (present or absent); (7) distant metastasis (present or absent); (8) central lymph node metastasis (present or absent); (9) contralateral cervicolateral metastasis (present or absent); (10) bilateral nodal metastasis (present or absent); (11) reoperation (present or absent); and (12) tumor differentiation (poor or good).
Data Extraction and Quality Assessment
The Basic Characteristics and Quality Evaluation of the Included Literature.
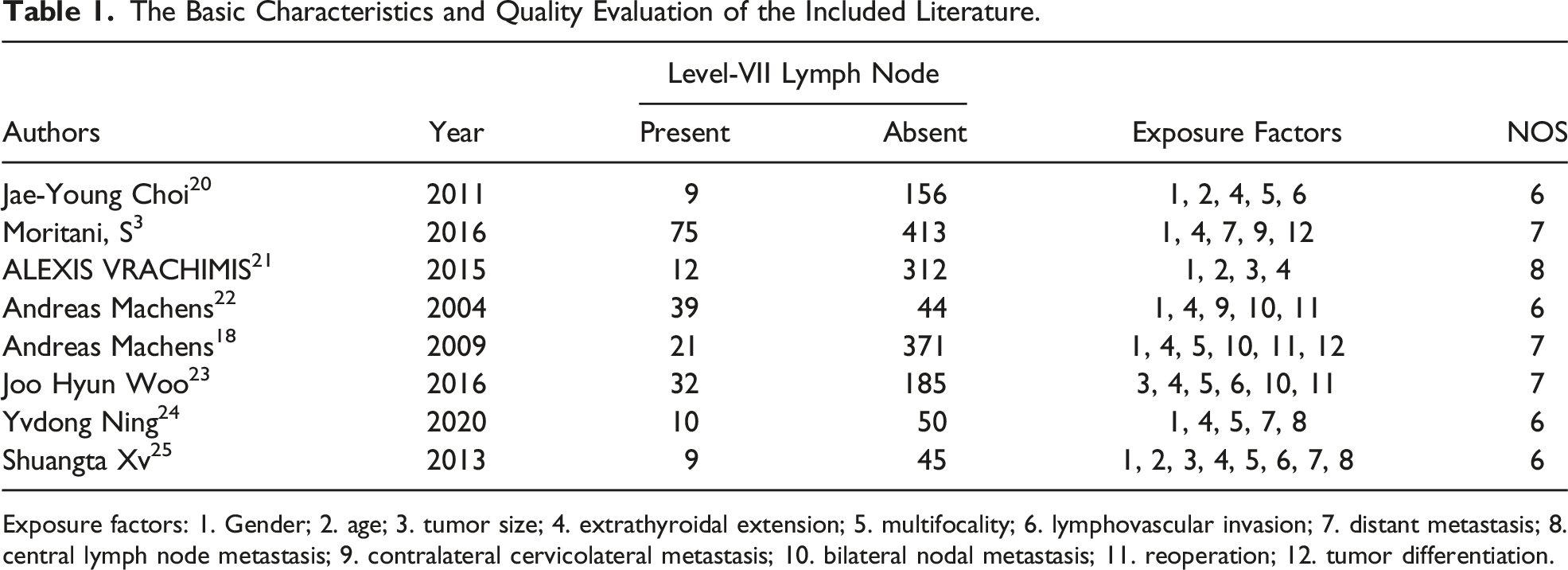
Exposure factors: 1. Gender; 2. age; 3. tumor size; 4. extrathyroidal extension; 5. multifocality; 6. lymphovascular invasion; 7. distant metastasis; 8. central lymph node metastasis; 9. contralateral cervicolateral metastasis; 10. bilateral nodal metastasis; 11. reoperation; 12. tumor differentiation.
Statistical Analysis
Statistical analyses of the included studies were performed with the Stata 13.1 software. I2 test and Q statistic test were performed to examine the heterogeneity, with I2 > 50% or P < .10 considered to indicate statistical significance. If I2 <50% and P > .1, the fixed-effects model was employed for meta-analyses. Otherwise, sensitivity analysis was performed to exclude the heterogeneous data. In case of no heterogeneity, a fixed-effects model was adopted. In the case of heterogeneity, all data included adopting a random-effects model. Publication bias was examined through the funnel plot and Egger’s test; when the funnel chart was symmetrical or Egger’s test >.05, it indicated no publication bias; otherwise, it indicated a publication bias.
Results
Results for Literature Search
Various electronic databases were searched to identify relevant studies. A total of 997 articles were identified. After the removal of duplicate articles, the remaining studies were evaluated, and 8 studies were included in the present study. Among these, 6 studies were written in English and 2 were in Chinese. The flow diagram followed for the selection of articles is shown in (Figure 1). Literature screening flowchart.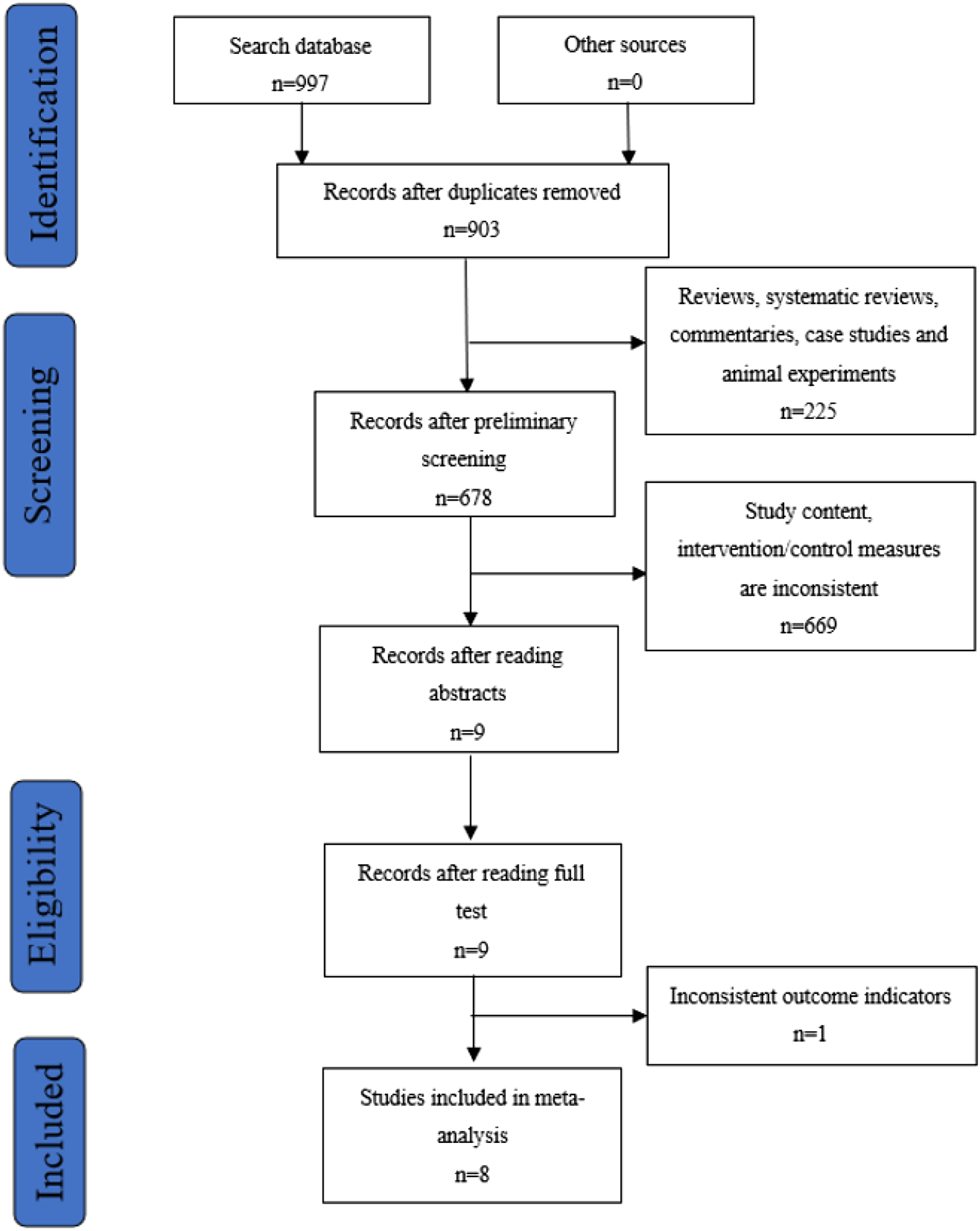
Basic Characteristics and Quality Evaluation
All the 8 studies included in the present meta‐analysis were case‐control studies that involved 1813 patients, of which 207 patients were included in the level-VII lymph node metastases group and 1606 in the non-metastases group. A total of 12 exposure factors that might cause level-VII lymph node metastases were extracted/assessed. The quality of these 8 studies was assessed using NOS. The basic characteristics and quality evaluation for the included studies are shown in Table 1.
Meta‐Analysis Results
Heterogeneity Test
Meta-Analysis of Exposure Factors for Level-VII Lymph Node Metastases.
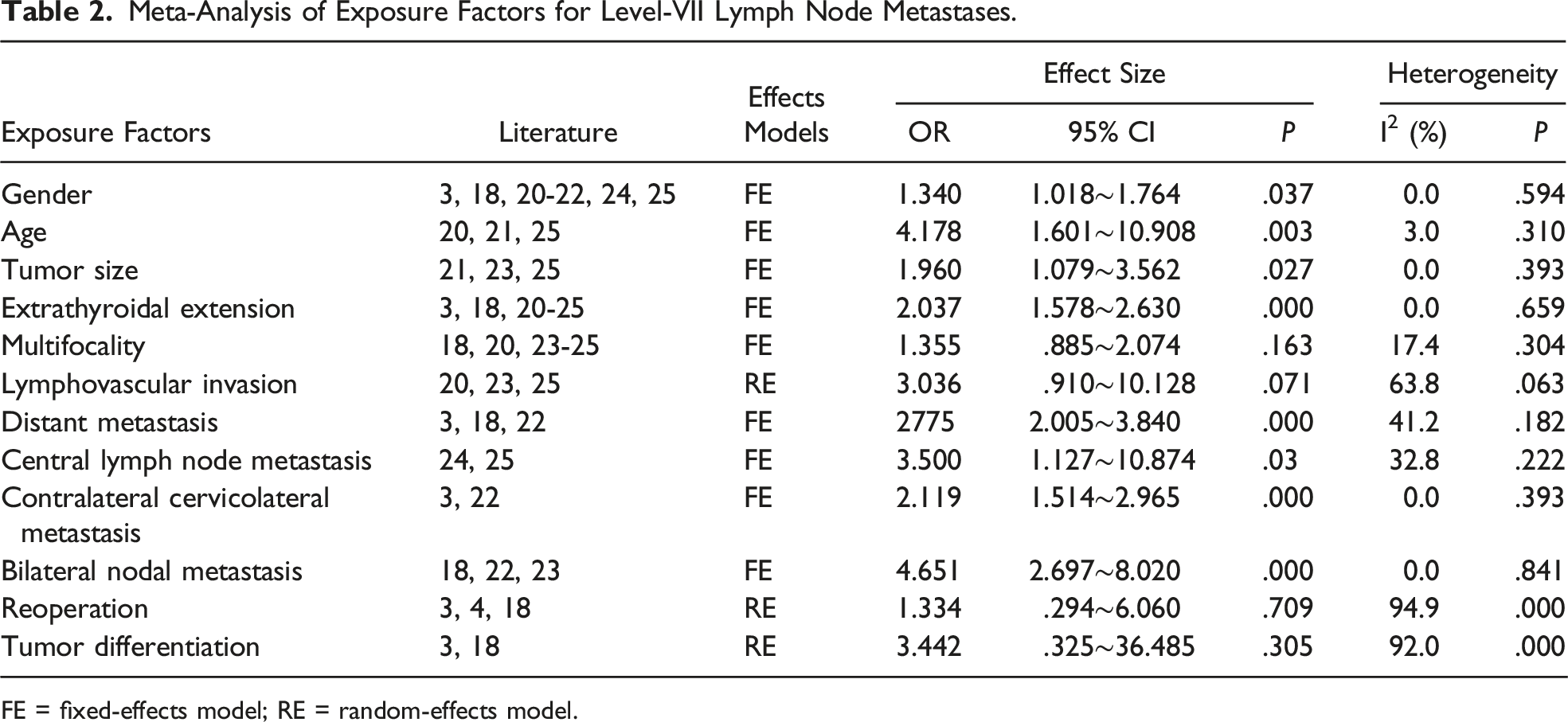
FE = fixed-effects model; RE = random-effects model.
Effect of Gender and Age
In this study, gender (OR = 1.340, 95% CI: 1.018-1.764, P = .037) was included as an exposure factor in 7 of the studies. After testing, no heterogeneity was observed, and a fixed-effects model was used for further analysis. Age (OR = 4.178, 95% CI: 1.601-10.908, P = .003) was included in 3 articles, and following testing, it was found to be heterogeneous. The study conducted by Choi and co‐workers was excluded by Rabe diagram, star diagram, and sensitivity test, following which fixed-effects model was adopted for this factor. The P values calculated for male gender and age <45 years were found to be smaller than .05, which indicated that these 2 factors acted as risk factors for level-VII lymph node metastases (Figure 2). Forest plots in gender and level-VII lymph node metastases.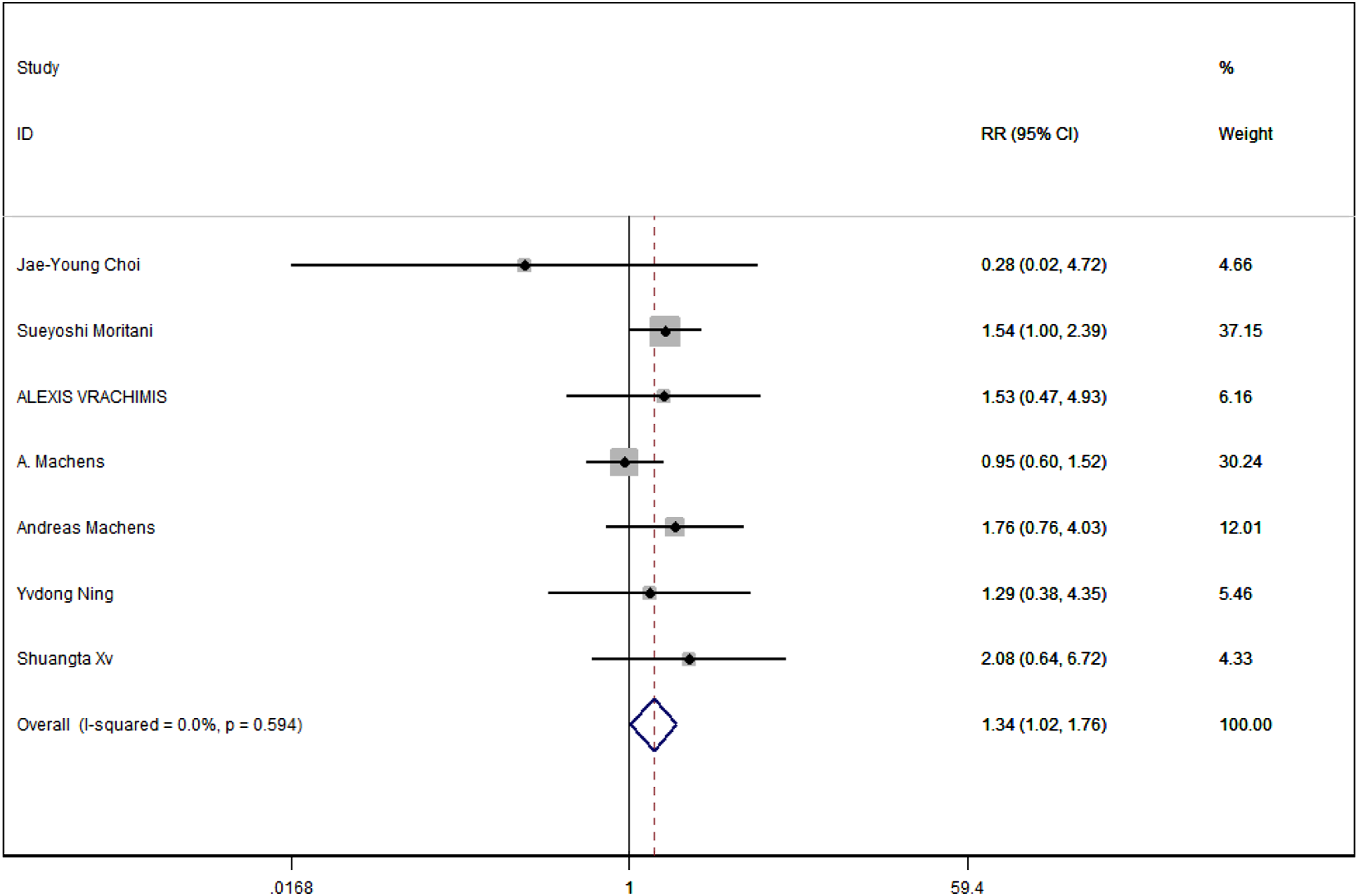
Effect of Tumor Size and Multifocality
Among the 8 articles included in the present study, 3 articles included the factor of tumor size (OR = 1.960, 95% CI: 1.079-3.562, P = .027) and 5 articles included the factor of multifocality (OR = 1.355, 95% CI: .885-2.074, P = .163). After heterogeneity analysis, these 2 factors did not show any heterogeneity. Consequently, the fixed-effects model was adopted for these factors. The P value for tumor size was found to be <.05, while for multifocality, it was >.05. These results showed that tumor size ≥2.0 cm acted as a risk factor for level-VII lymph node metastases in case of thyroid neoplasms, while multifocality did not exert any such effect (Figure 3). Forest plots in multifocality and level-VII lymph node metastases.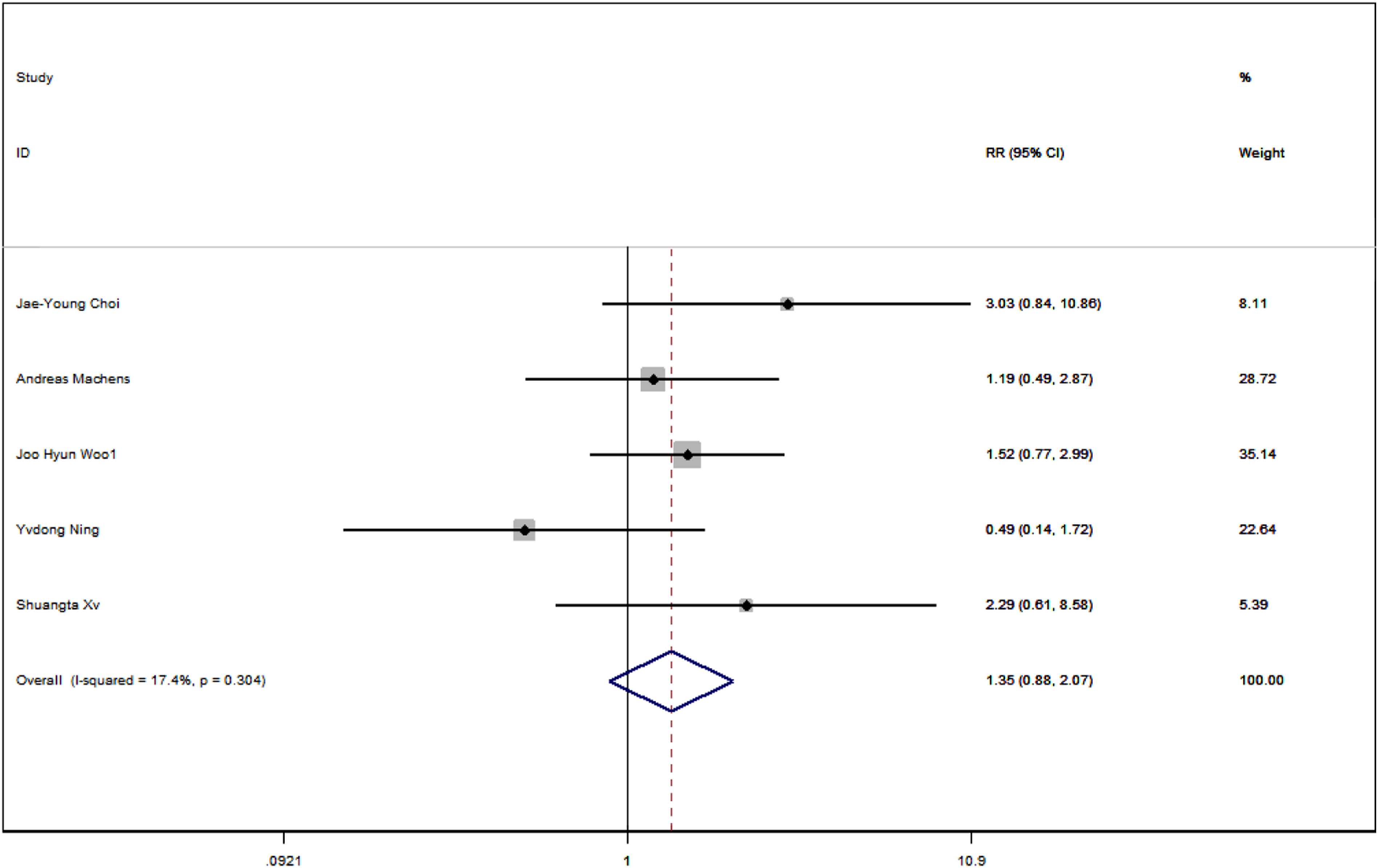
Effect of Extrathyroidal Extension and Lymphovascular Invasion
Extrathyroidal extension (OR = 2.037, 95% CI: 1.578-2.630, P < .001) was included in 8 studies, and no heterogeneity was identified after testing. Further, a fixed-effect model was used and the P value was recorded to be < .05, which indicated that extrathyroidal extension might act as a risk factor for level-VII lymph node metastases for thyroid neoplasms (Figure 4). However, only 3 studies included lymphovascular invasion (OR = 3.036, 95% CI: .910-10.128, P = .071), and it was found to be heterogeneous. Following the exclusion of most heterogeneous studies, the remaining studies still exhibited heterogeneity. Besides this, the inclusion data were less than the original data, as calculated by the random-effects model. The P value was calculated to be > .05, indicating the absence of statistically significant differences between lymphovascular invasion and no invasion. Forest plots in extrathyroidal extension and level-VII lymph node metastases.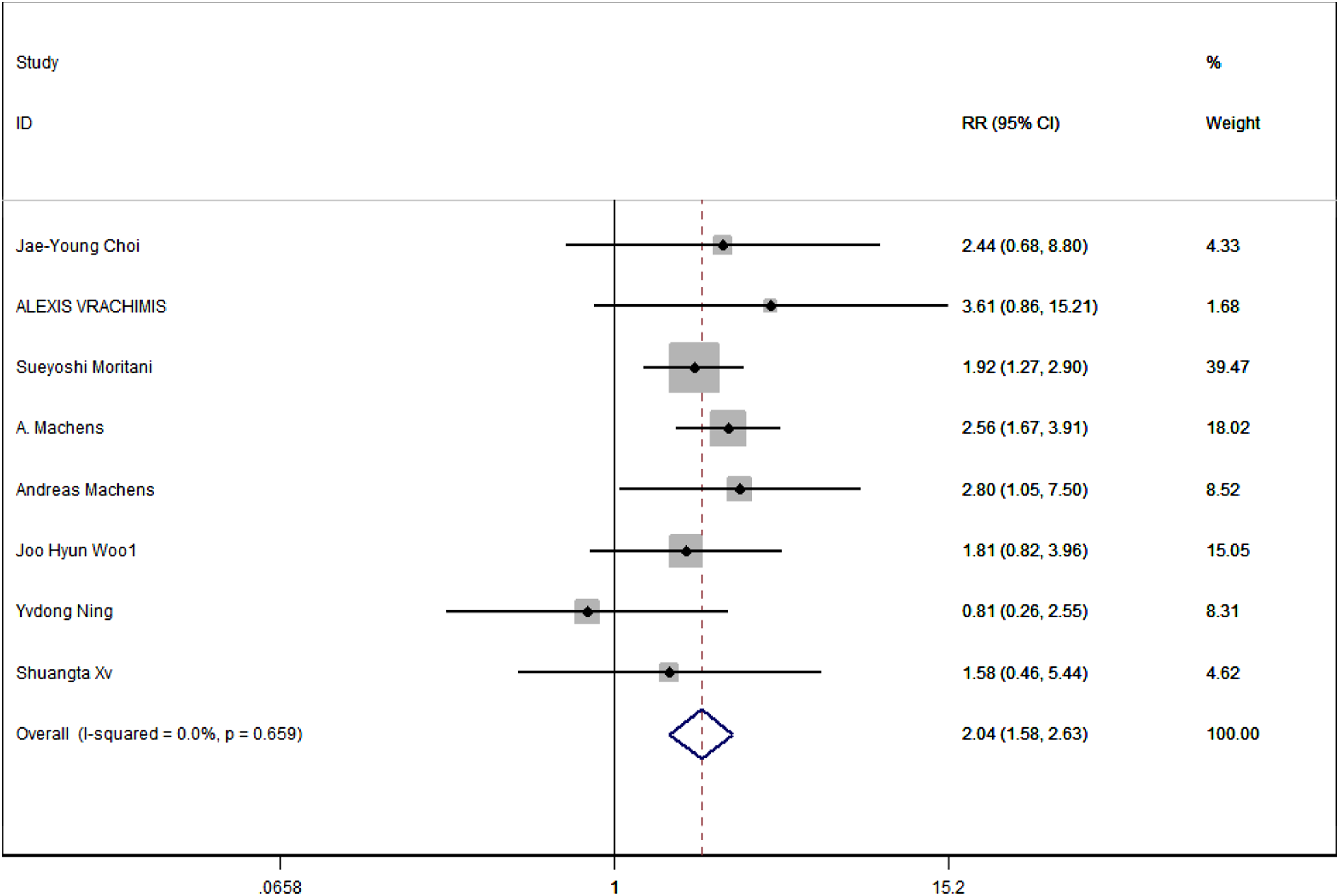
Effect of Central Lymph Node Metastasis, Contralateral Cervicolateral Metastasis, Bilateral Nodal Metastasis, and Distant Metastasis
Central lymph node metastasis (OR = 3.500, 95% CI: 1.127-10.874, P = .03) was included in 2 studies, contralateral cervicolateral metastasis (OR = 2.119, 95% CI: 1.514-2.965, P < .001) was included in 2 studies, and distant metastasis (OR = 2.775, 95% CI: 2.005-3.840, P < .001) was included in 3 studies. Since no heterogeneity was observed following testing, these 3 factors adopted fixed-effects models. Bilateral nodal metastasis (OR = 4.651, 95% CI: 2.697-8.020, P < .001) was included in 3 studies. For this factor, the fixed-effects model was used after the exclusion of a heterogeneous study. Based on the calculations, the P values for these 4 exposure factors were found to be smaller than .05, which indicated that the differences were statistically significant. Thus, central lymph node metastasis, contralateral cervicolateral metastasis, bilateral nodal metastasis, and distant metastasis might be related to the risk for level-VII lymph node metastases in case of thyroid neoplasms.
Effect of Reoperation and Tumor Differentiation
In the present study, tumor differentiation (OR = 3.442, 95% CI: .325-36.485, P = .305) was included in only 2 studies. The test further confirmed the existence of heterogeneity. Reoperation (OR = 1.334, 95% CI: .294-6.060, P = .709) included a total of 3 studies. Following the star chart, Rabe diagram, and sensitivity test, these 3 studies were found to exhibit great heterogeneity. Therefore, these 2 exposure factors adopted a random-effects model. The P values for both these factors were found to be > .05, which confirmed that the difference was not statistically significant. These results indicated that poor tumor differentiation of thyroid neoplasms and reoperation did not act as risk factors for level-VII lymph node metastases.
Sensitivity and Bias Test
Following the use of a Rabe diagram, star diagram, and sensitivity analysis, some of the studies were excluded in the case of age and bilateral nodal metastasis. In cases where less than 5 groups were included in the data, Egger’s test was used, whereas a funnel chart was drawn/used when more than 5 groups were included in the data. It was reported that none of the risk factors exhibited publication bias.
Discussion
In comparison to the seventh edition of the American Joint Committee on Cancer (AJCC), level-VII lymph node metastases of thyroid neoplasms were juxtaposed with unilateral and bilateral central lymph nodes in the eighth edition of the AJCC. In particular, all these belonged to N1a, and the risk stratification for age changed from 45 years to 55 years. This showed that the eighth edition of the AJCC reduced patients to a lower stage as compared to the seventh edition, which suggested that level-VII lymph node metastases and central lymph node metastases possessed similar significance. Although no clear relationship exists between level-VII lymph node metastases and reduction of patient survival, several previous studies showed that level-VII lymph node lymphadenectomy could reduce the recurrence rate of tumors. 5 A retrospective study previously showed that patients with upper mediastinal lymph nodes exhibited shorter 10‐year disease‐specific survival and shorter disease‐free survival. 3 The level-VII lymph nodes are usually located behind the breastbone. The use of both traditional sternum splitting and endoscopy increases the complexity and difficulty level of the surgery. The surgery is known to exert a greater impact on the patient’s postoperative recovery and postoperative complications (pneumothorax, mediastinitis, and others). Thus, it is very important to judge/identify level-VII lymph node metastases for lymphadenectomy during the surgery.
For patients with thyroid nodules, preoperative ultrasound is routinely performed in clinical practice. However, the level-VII lymph node is under‐assessed, primarily owing to the limitations of ultrasound. In comparison to this, enhanced CT could more objectively evaluate lymph node metastasis in the upper mediastinum group. In case of allergies to iodine or thyrotoxicosis, enhanced MR could be used for evaluation. 2 Following the prediction of the risk factors associated with level-VII lymph node metastases of thyroid cancer, the resulting information can be combined with preoperative examination and intraoperative situation to accurately estimate the status of metastases, which would further provide a reference for level-VII lymph node lymphadenectomy.
Several previous studies reported that male gender, age < 45 years, and large tumor size acted as risk factors for central lymph node metastasis.6,7 The results for the present meta‐analysis also showed that male gender, age < 45 years, and tumor size ≥ 2.0 cm were related to level-VII lymph node metastases. However, since the studies included in this meta‐analysis were published earlier, most of these still used 45 years for age stratification. Consequently, the cut‐off point for the present study was 45 years instead of 55 years, which has been recommended by the eighth edition of the AJCC. Since the present study involved small data and differences were observed in the classification of tumor sizes, when compared with other studies, a definite relationship of age < 45 years, male, and tumor size ≥ 2.0 cm with cervical lymph node metastasis of thyroid cancer could not be confirmed.
At this stage, an extrathyroidal extension of thyroid cancer is defined as the invasion of cancer cells beyond the thyroid capsule. The results of this meta‐analysis showed that extrathyroidal extension acted as a risk factor for level-VII lymph node metastases. Previous studies confirmed that extrathyroidal extension was related to lymph node metastasis 8 ; however, most of these studies lacked a specific grouping of lymph node metastasis. Since the present study included only 8 groups of data, the reliability of conclusions was low. Importantly, none of the studies explained the association between extrathyroidal extension and level-VII lymph node metastases.
In a previous study, Tam and co‐workers reported that an increase in the number of tumors would lead to a higher rate of lymph node metastasis. 9 In another study, Cai and co‐workers reported an association between unilateral multifocality and central lymph node metastasis. 10 When compared with 2 cancer foci, 3 cancer foci were reported to be more prone to central lymph node metastasis. 11 Previous studies showed that multifocality could easily lead to central lymph node metastasis, primarily owing to the coexistence of multiple histological subtypes. 12 In comparison to this, not much information is available regarding the association between several lesions and level-VII lymph node, which is known to be the continuation of the central lymph node. The results for meta-analysis in the present case revealed the absence of any correlation between several lesions and level-VII lymph node metastases. However, the use of fewer data might lead to errors in the analysis. Thus, more data are still required to verify the relationship between these 2.
Lymphovascular invasion in thyroid cancer is defined as the movement of cancer cells into the blood vessels and/or lymphatic vessels, as observed in histopathology. 13 In a previous study, Kim and co‐workers confirmed the existence of a significant correlation between lymphatic vessel invasion and lateral neck lymph node metastasis, as revealed by an analysis of 662 patients with papillary thyroid cancer. 14 Meta‐analysis performed by Yoon and co‐workers also showed that lymphovascular invasion was significantly related to metastasis of contralateral cervical lymph nodes, especially in the case of level-III and -IV lymph node. 15 In a previous study, Merdad and co-workers confirmed that lymphatic vessel invasion was related to level-V lymph node metastasis; however, it did not exhibit any significant association with level-II lymph node metastasis. 16 In addition to this, previous studies confirmed that lymphovascular invasion in primary tumors exhibited an independent positive correlation with local lymph node metastasis. For primary non‐small cell lung cancer, lymphatic vessel invasion was found to be associated with mediastinal lymph node involvement. 17 However, no previous studies confirmed the relationship between primary thyroid cancer and upper mediastinal lymph nodes.
In a previous study, Machens and co‐workers observed that poor tumor differentiation and distant metastasis acted as significant predictors for mediastinal lymph node metastasis. In comparison to this, tumor differentiation exhibited higher accuracy and positive rate for the prediction than distant metastasis. 18 It is generally considered that MLNM involves metastasis from paratracheal or pretracheal lymph nodes and lateral neck lymph nodes, which is mediated via lymphatic circulation. However, some of the studies previously showed that primary tumor directly metastasizes to the mediastinum, without the involvement of central or lateral neck LNM. 19 Therefore, the specific mechanism responsible for the association of metastasis in level-VII with contralateral neck lymph node, bilateral lymph node, and central lymph node requires further research.
The present study was associated with certain limitations. In particular, the number of exposure factors included in this study was small. The present study is further limited by the limitations of the studies included in the present analysis. The studies included in the present study were written either in Chinese or English, which might affect the comprehensiveness of the data to a certain extent. Currently, only a few studies are available on the prognosis of level-VII lymph node metastases. Consequently, no study is available for meta‐analysis of prognosis after screening. Therefore, the current study is only an observational study. Since the limitations of this study might affect the results of meta‐analysis and promotion of the conclusions, the present study can be used only as a reference for the prediction of risk factors associated with level-VII lymph node metastases of thyroid neoplasms, and more case‐controlled experiments are required for demonstration/verification in the future.
Supplemental Material
sj-pdf-1-asu-10.1177_00031348211069801 – Supplemental Material for Risk Factors for Level-VII Lymph Node Metastases of Thyroid Neoplasms: A Meta-Analysis
Supplemental Material, sj-pdf-1-asu-10.1177_00031348211069801 for Risk Factors for Level-VII Lymph Node Metastases of Thyroid Neoplasms: A Meta-Analysis by Wang Zhi Ruo, Sun Han Xiao, Feng Zhe Ming, Zhu Chun Yue, Meng Zhi Wen, and Zhang Feng Hua in The American Surgeon
Footnotes
Acknowledgments
This study would not have been possible without insightful guidance, enthusiastic encouragement, and valuable reference materials from my tutors.
Author Contributions
Proposed ideas, conceived and designed: Zhi-Ruo Wang and Han-Xiao Sun; screened the literature data: Zhi-Ruo Wang, Zhe-Ming Feng, and Chun-Yue Zhu; analyzed the results: Zhe-Ming Feng, Chun-Yue Zhu and, Zhi-Wen Meng; and writing—original draft: Han-Xiao Sun and Zhi-Wen Meng and writing—review and editing: Feng-Hua Zhang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.