
Abstract
Background
The role of the intersphincteric space in the pathogenesis of fistula-in-ano is being increasingly recognized. Submucosal and intersphincteric rectal abscesses have been surgically managed by laying open and draining the intersphincteric space as well as by the modified ligation of intersphincteric fistula tract (LIFT) procedure. In 2017, the transanal opening of intersphincteric space (TROPIS) technique was reported for the treatment of high, complex anal fistulae.
Aim
We aim to investigate the advantages of performing the TROPIS procedure in patients with fistula-in-ano.
Methods
This was a prospective cohort study investigating the outcomes in patients who had undergone a procedure using the TROPIS technique for the treatment of fistula-in-ano. Preoperative magnetic resonance imaging scans and electronic colonoscopies were performed on all patients. A clinical database evaluating the following variables was constructed: age, gender, body mass index (BMI), previous fistula surgery, type of fistula, postoperative complications, duration of follow-up, success rate, and incontinence scores pre- and postoperatively.
Results
The TROPIS procedure was performed on 41 patients with fistula-in-ano with a follow-up time of 6-23 months. The characteristics of the patients were as follows: 36 males, 6 females, mean age 38.6±13.2 years, and mean BMI 23.5±3.9 kg·m−2. All patients (41) had transsphincteric fistulae, and 90.2% (37) had high fistula. Of the 41 patients, 22% (9) had recurrent fistulae, 29.27% (12) had horseshoe fistulae, 7.3% (3) had supralevator fistulae, and 14.6% (6) had an associated abscess. The fistula healed completely in 85.3% (35) of patients and failed to heal in 14.7% (6) of patients, and the healing of high fistula was 86.5% (32). Of those patients who had not healed completely, 2 were found to have contracted iatrogenic infections due to foreign residues and underwent surgery with the passing of a loose seton. The additional 4 patients who had not healed underwent a fistulotomy and healed completely thereafter. There were no significant changes in incontinence scores. The incontinence scores were .15 ± .36 preoperatively and .22 ± .47 3 months postoperatively (t = −1.438, P = .16).
Conclusions
The TROPIS technique is a novel sphincter-preserving procedure, which can be effectively used in treating fistula-in-ano.
Introduction
Anorectal surgeons have been seeking a procedure that provides both fistula healing and preserved anal function for the treatment of anal fistulae. An indisputable fact is that treatment by fistulotomy has a satisfactory success rate. However, it increases incontinence. This has resulted in the innovation of sphincter-preserving procedures, tools, and methods such as loose seton, 1 over-the-scope clip, 2 anal fistula plug, 3 fibrin glue, 4 ligation of intersphincteric fistula tract (LIFT), 5 and video-assisted anal fistula treatment. 6 However, long-term results have been controversial. Therefore, it is undeniable that the treatment of fistula-in-ano, especially complex high fistulae, remains an enormous challenge for surgeons.
In the late 1960s, the theory of a cryptoglandular etiology in fistula-in-ano was formed by Parks and Eisenhammer.7,8 Subsequently, the Parks’ classification was developed, 9 and it was regarded as the “compass” for guiding fistula treatment. A recent study had demonstrated that the posterior deep intersphincteric space was more susceptible to being involved in the formation of complex cryptoglandular fistulae than the deep postanal space. 10 This finding was considered an important complement to the cryptoglandular theory. 11 The role of the intersphincteric space in the pathogenesis of fistula-in-ano is being increasingly recognized.12,13
Garg 12 suggested that the infection in the intersphincteric space was walled off and that proper healing of the fistula would only occur if it was sufficiently drained and kept open. Thus, he proposed the transanal opening of intersphincteric space (TROPIS) technique. The TROPIS procedure consists of opening the intersphincteric space into the rectum and managing the external tracts effectively. We performed TROPIS procedure and excised the external tracts, aiming to evaluate the success of this technique.
Method
This prospective study consisted of 41 patients, diagnosed with fistula-in-ano on preoperative perianal magnetic resonance imaging (MRI), who had undergone the TROPIS procedure in a hospital between April 2017 and June 2019. The study was approved by the ethics committee of the hospital, and all patients provided written informed consent. Informed consent was also obtained for the surgery.
Inclusion Criteria
Patients with the following fistulae were included in the study: 1. Transsphincteric cryptoglandular fistula 2. Horseshoe fistula 3. Supralevator fistula
Exclusion Criteria
Patients with the following fistulae were excluded from the study: 1. Intersphincteric cryptoglandular fistula 2. Neoplastic fistula 3. Tuberculous fistula 4. Fistula-in-ano associated with inflammatory bowel disease (Crohn’s disease and ulcerative colitis)
Operative Procedure
Preoperative perianal MRI scans were performed on all patients. The location and type of fistula were identified based on MRI images via detailed discussion between the surgeon and the radiologist. Preoperative electronic colonoscopy was performed on patients with colorectal tumors, intestinal tuberculosis, and inflammatory bowel disease (Crohn’s disease and ulcerative colitis).
The TROPIS procedure was performed as described by Garg,
12
which is shown in the schematic diagram (Figure 1). A bowel preparation consisting of a polyethylene glycol-electrolyte solution was given to all patients preoperatively. An intravenous dose of an antibiotic, ornidazole 500 mg, was administered 30 minutes before surgery. Patients were placed in the prone jackknife position after a spinal epidural was successfully performed. The internal opening of the fistula was confirmed by injecting hydrogen peroxide solution through the external opening or with the assistance of a probe. A 1-2 cm curved incision was made using the examination finger at the intersphincteric groove after it was identified. The fistula in the intersphincteric space was laid open and adequately drained after the mucosa and internal sphincter over the fistula were incised by electrocautery with the guidance of the probe or dye. Occasionally, the incision would require outward extension by 1 cm in order to achieve adequate drainage. (A) Schematic drawing of the transsphincteric fistula. (a) The internal sphincter; (b) the intersphincteric space and longitudinal muscle; (c) the puborectalis muscle; (d) the external sphincter; (e) perianal space. A curved incision was made at the intersphincteric groove, and an internal sphincterotomy was performed along the fistula tract. Then, the residual fistula was removed using a tunnel-based method, and the defect of the external sphincter at the intersphincteric space was sutured ultimately. Sometimes, a loose seton was also passed between the external orifice and the intersphincteric space (B).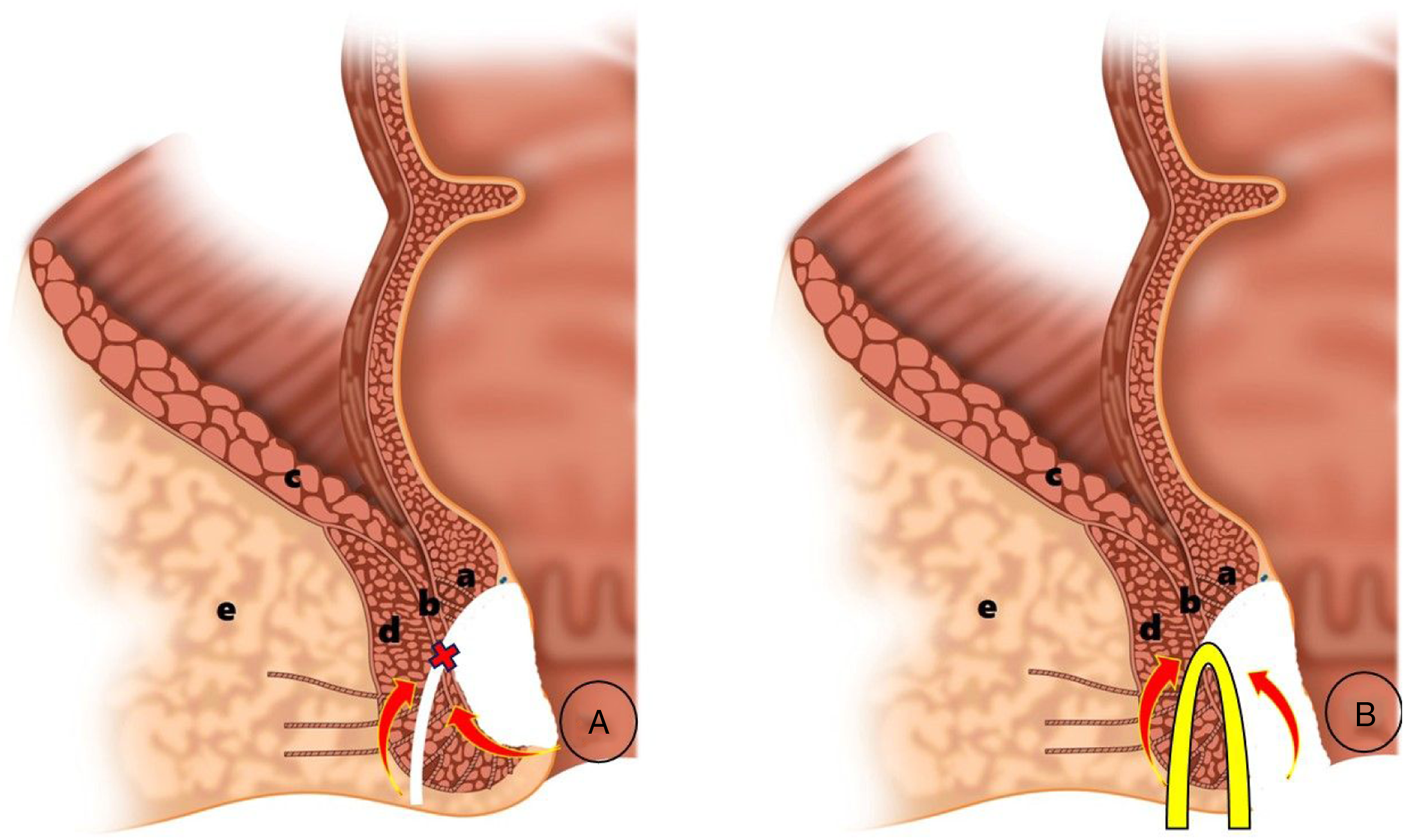
Thereafter, the residual fistula was removed between the external opening and the intersphincteric space using a tunnel-based method. An external sphincter defect of <1 cm in diameter was then sutured using 3/0 Tyco absorbable sutures at the intersphincteric space using a transanal approach (Figures 1A and 2A). The external opening was then opened to allow drainage. Moreover, a loose seton was passed if the diameter of the defect of the external sphincter was >1 cm or if an associated abscess was present (Figure 1B). This often fails due to the tension, blood supply, and infection that occurs as a result of the tautness. The fistula tissues were sent for histopathology testing and polymerase chain reaction testing in order to determine whether Mycobacterium tuberculosis was present. A 35-year-old woman with a high transsphincteric fistula treated by the TROPIS procedure and followed up after 6 months. Operative photographs showing the draining intersphincteric space (A), followed by the removal of the residual fistula using a tunnel-based method (B), immediate suturing of the defect in the external sphincter at the intersphincteric space (A), and the complete operation.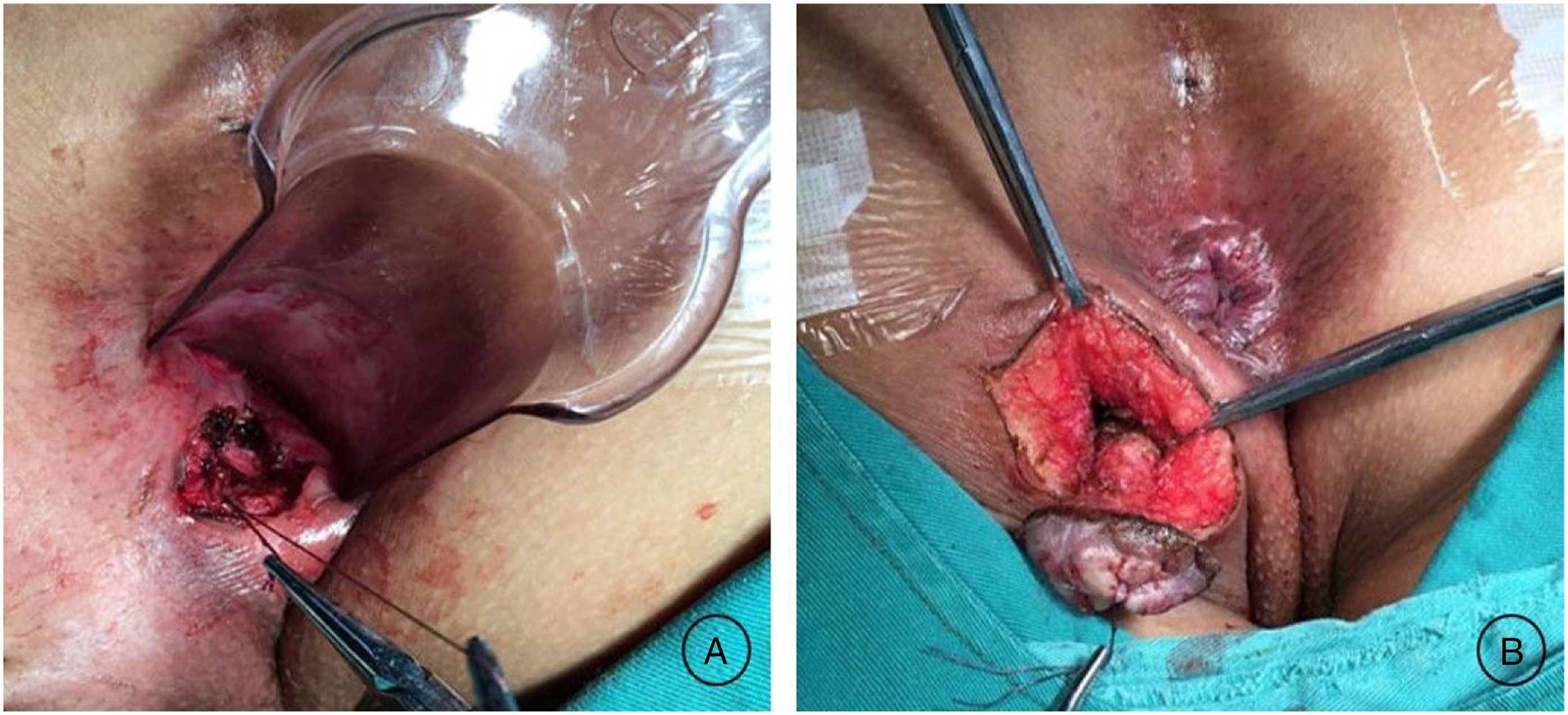
Postoperative Care
All procedures were performed in an inpatient department. Postoperatively, the patients were prescribed a normal diet and were advised to resume normal activities. They were instructed to have sitz baths twice a day with the addition of a traditional Chinese medicine, “Kulao Decoction.” The wound was then cleaned with povidone-iodine and kept open for drainage. Patients were reviewed in the outpatient clinic once a week until the fistula healed. Anal function was assessed preoperatively and 3 months postoperatively using the Wexner score. The scores represent the severity of the incontinence. Those who are fully continent obtain a score of 0, and those with complete anal incontinence obtain a maximum score of 24. The fistula was considered healed when the wound had completely healed and no pus was discharged from the fistula or anus. Conversely, if any pus was discharged from the fistula, it was considered as a failure. A clinical database evaluating the following variables was constructed: age, gender, body mass index (BMI), previous fistula surgery, type of fistula, postoperative complications, duration of follow-up, and success rate.
Statistical Analysis
Statistical software Statistical Package for the Social Sciences 22.0 was utilized in the present study. The categorical variables were analyzed using chi-square or Fisher’s exact tests. The continuous variables were analyzed using t-tests or analysis of variance. A value of P < .05 was considered statistically significant.
Results
The TROPIS procedure was performed on 41 patients with fistula-in-ano, and no surgical complications occurred. The ratio of male and female patients was 35:6, the mean (± standard deviation) age was 38.6 ± 13.2 years, and the mean BMI was 23.5 ± 3.9 kg m−2. The median (range) follow-up time was 22.2 (6-35) months. No patients were lost to follow-up.
All patients (41) had transsphincteric fistulae, and 90.2% (37) had high fistula (involving more than 1/3 of external sphincter). Of the total patients, 22% (9) had recurrent fistulae, 29.27% (12) had horseshoe fistulae, 7.3% (3) had supralevator fistulae, and 14.6% (6) had an associated abscess. No patients tested positive for Mycobacterium tuberculosis on pathology examination. At the end of the follow-up period, complete healing of the fistula was found in 85.3% (35) of patients, 14.7% (6) of patients had not healed, and the healing of high fistula was 86.5% (32). Among the 6 failed procedures, 1 had a supralevator fistula and 5 had high transsphincter fistulae. An iatrogenic infection was found during surgical exploration in 2 patients who then underwent further irrigation, drainage, and the passing of a loose seton. The additional 4 failed cases underwent a fistulotomy. All fistulae had healed in these 6 patients following the second intervention. There was no significant change in incontinence scores. Preoperative incontinence scores (±standard deviation) were .15 ± .36, and 3-month postoperative scores were .22 ± .47 (t = −.79, P = .43).
Discussion
The results of this study showed that the TROPIS procedure was effective at curing fistula-in-ano with a cure rate of 85.3%. This was particularly true in cases with high fistula with a cure rate of 86.5% and associated abscesses. Figures 1 and 2 highlight examples of these.
In our opinion, there are 3 key aspects in treating fistula-in-ano. First, the infection should be excised and the crater left open. Sepsis in the intersphincteric space is similar to a concealed abscess. Therefore, it should be drained adequately and kept open in order to promote fistula healing by secondary intention. 12 Second, resection of the track should be performed as extensively as possible while minimizing sphincter injury. Failure occasionally occurs as a result of fibrosis or the incomplete clearance of secretion residues in the fistula. Third, the surgical wound should be cleaned and drained sufficiently in order to create a favorable environment for fistula healing. Fistulotomies, with the consideration of the above 3 aspects, are associated with a high cure rate. However, this is at the expense of significant sphincter injury. The TROPIS procedure also adheres to all of the above aspects by laying open the intersphincteric space transanally and removing the fistula (Figure 1). This technique has solved a vital problem, that is often neglected, by highlighting the advantageous effects of healing by secondary intention, rather than primary intention, following infective fistula surgery.
An intersphincteric approach is beneficial when performing a sphincter-preserving procedure. In 1993, Matos et al 14 reported a sphincter-preserving procedure using the intersphincteric approach. This approach was quite similar to LIFT which was later defined by Rojanasukal et al. 5 However, the technique has not been widely used. Recently, the LIFT procedure, described by Rojanasakul, seems to be one of the most popular sphincter-preserving procedures performed as it ensures minimum sphincter damage. Furthermore, it adheres to the first aspect we have stated above but falls short in addressing the second and third aspects. Subsequent studies have shown that the success rate of this procedure has been decreasing,15-17 and many improvements have been made.18,19 There are vital differences in principle between the TROPIS and LIFT procedures. Although both of them resect the fistula tract in the intersphincteric space using an intersphincteric route, LIFT mainly focuses on the ligation of the fistula tract, while TROPIS mainly emphasizes the opening of the intersphincteric space for drainage.
The anatomical structure of the area inevitably results in the inclusion of the sphincter during anal fistula surgery. Transanal drainage of rectal abscesses (submucosal and intersphincteric), fistulotomy of intersphincteric fistulae, and dividing the internal sphincter using the modified LIFT 19 have been proven to be safe and effective treatments. The results of the TROPIS procedure reported by Garg 12 showed an overall healing rate as high as 90.4%, without incontinence occurring. Therefore, we emphasize that this sphincter-preserving procedure is not without sphincter injury but preserves anal function as much as possible in order to avoid fecal incontinence. Acceptable success rates should include minimum rates of sphincter damage.
A recent study showed that removing residual fistula tissue during the LIFT procedure could improve the success rate without increasing the rate of fecal incontinence. 20 Enlightened by this research, we removed residual fistula tissue using a tunnel-based method instead of scraping the tissue. The results of the study, which has a follow-up period of 6-35 months, highlighted the effectiveness of the TROPIS procedure as it had a healing rate of 85.3%, without incontinence occurring. Therefore, transanal laying open of the intersphincteric space and removal of the fistula are theoretically effective.
The postoperative management of fistula-in-ano is as important as the procedure. Secretions on the surface of the incision should be frequently cleaned, and false healing and iatrogenic infection should be avoided. It is particularly necessary to prevent false healing of the wound as a result of closure due to sphincter contraction postoperatively. The fistula was resected using the TROPIS procedure in this study, which further encourages open drainage of the wound and the avoidance of foreign matter residues. In this study, there were 2 cases of iatrogenic infection caused by residual medical material, which resulted in failure. Therefore, effective drainage and avoiding foreign matter residue are the key points of effective wound nursing postoperatively.
In conclusion, a satisfactory healing rate (85.3%) has been shown in the present study, which consisted of >90% of patients having high fistula. The results were similar to those reported by Garg, 12 in which there were over 80% of patients with multiple and recurrent fistulae. Furthermore, both studies have reported no incontinence experienced by patients following the procedures. The preliminary advantages of the TROPIS procedure in the treatment of fistula-in-ano have been demonstrated. This technique, which minimizes incontinence by avoiding incision of the external sphincter, was considered a novel sphincter-preserving procedure. However, this study had a small sample size and occurred in a single center. Further research evaluating the long-term effects of the procedure in a larger number of patients across varying centers is required.
Footnotes
Acknowledgements
We thank every patient who participated in this research because they provided us with materials and gave us full trust. At the same time, we also thank reviewers and editors for their deep and careful work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data available on request from the authors: The data that support the findings of this study are available from the corresponding author De-gang Li, upon reasonable request.