
Abstract
Background
Surgical fields are historically dominated by male physicians. Increasing the diversity of the physician workforce improves training and patient experiences. We aim to investigate any differences in qualifications and match rates between male and female applicants to general surgery (GS) and orthopedic surgery (OS) residencies in the United States.
Methods
A retrospective cohort analysis was performed utilizing the Association of American Medical Colleges data regarding Electronic Residency Application Service (ERAS) applicants and matched Accreditation Council for Graduate Medical Education (ACGME) residents into GS and OS residencies from 2015 to 2019. Descriptive statistics and independent sample T-tests were performed with significance defined as P < .05.
Results
26 568 GS and 7076 OS ERAS applicants matched at a rate of 25.2% and 55.3%, respectively. Men and women matched into GS at rates of 23.0% and 29.2%, respectively. Men and women matched into OS at rates of 55.2% and 56.2%, respectively. Men aged ≥36 years matched into OS at a significantly higher rate than women aged years ≥36 (11.9% vs. 1.4%, P = .009). Female GS ERAS applicants and entering ACGME residents had a higher mean number of research experiences than male GS ERAS applicants (2.66 vs. 2.26, P < .001) and entering male GS ACGME residents (2.96 vs. 2.56, P = .008).
Conclusions
Male and female GS and OS applicants have similar qualifications. Women match into GS and OS at higher rates than men but comprise disproportionately lower numbers of applicants. Greater mentorship opportunities and recruitment of female applicants are needed to expand, diversify, and increase representation of women in surgery.
Keywords
Background
Despite a physician shortage in the United States (US), the competition for residency positions continually rises across almost all specialties. 1 United States Medical Licensing Examination (USMLE) Step 1 scores, USMLE Step 2 scores, Alpha Omega Alpha (AOA) status, research, and volunteer experiences have been previously cited as being highly influential in affecting the chances of applicants matching into their desired residency program.2,3 Therefore, closer investigation of the relationship between match rates and gender, medical degree type, age, and race/ethnicity is necessary to identify potential disparities and recommend strategic implementation of institutional and individual applicant interventions which can contribute to the most fair matching process possible.
The number of women matriculating into US medical schools has grown from 46.9% of the class in 2010 to 51.6% in 2018, indicating gender inequalities in the selection process are being reduced.4,5 However, surgical fields are still heavily male dominated.6,7 Specific specialties, such as general surgery (GS), orthopedic surgery (OS), and neurosurgery, have historically accepted low numbers of women.6-10 The number of women in these fields has not experienced the same growth as other specialties such as obstetrics/gynecology, family medicine, and pediatrics. 5 In fact, OS has recently been cited as the surgical subspecialty with the lowest proportion of women. 5 Consequently, substantial research has been devoted to understanding factors that are instrumental in increasing the diversity of surgical programs. During the years 2007-2014, female representation in OS rose from 11% to 14.4%. 10 Despite growth, this is significantly lagging behind other specialties. 10 Evidence shows OS residencies with increased gender diversity in their faculty and residents have a greater amount of female applicants. 6 Similarly, the amount of women in leadership roles, the option to do a research year, and having a women’s sports medicine program are all influential in determining how many women match into OS. 11
Although application characteristics such as being a US medical graduate, quantity and quality of research experiences, and first-time applicants have been positively associated with successfully matching, these variables are rarely stratified and compared by gender to determine whether the applicant selection process is equal.12-14 By investigating potential differences in the match process, we can identify areas to implement interventions that can increase the comfort and ability for female residents to focus on their surgical education and increase workforce diversity. Therefore, the primary aim of this analysis is to investigate gender differences and factors influencing National Residency Match Program (NRMP) match rates among male and female applicants into Accreditation Council for Graduate Medical Education (ACGME) GS and OS residency programs from 2015 to 2019. The secondary aim of this analysis is to investigate trends and factors influencing overall match rates for all GS and OS residency applicants from 2015 to 2019.
Methods
A retrospective cohort analysis was performed utilizing data from the Association of American Medical Colleges (AAMC) and NRMP regarding US-based GS and OS residency programs from 2015 to 2019. Aggregate level data from GS and OS Electronic Residency Application Service (ERAS) applicants and entering ACGME residents were obtained. As the matching process starts in the fall of the year before the start of the residency, the ERAS applications spanned the 2014-2015 year through the 2018-2019 year. Variables including age, underrepresented minority (URM) status, applicant degree type, first-time applicant vs. reapplicant status, USMLE Step 1 and Step 2 scores, and mean number of research experiences were stratified by gender from the AAMC and NRMP where possible. The age-groups in our study for gender-specific and gender-independent analysis were utilized based on predetermined divisions by the AAMC and presented in the same separations as data were received. Information regarding entering ACGME residents was obtained by the AAMC GME Track Resident Survey. To examine matched applicants, ERAS data are compared to data submitted from each program’s survey in the GME Track. Data regarding matched ACGME residents were compared to ERAS applicants to create relative mean match rates for variables for the 2015-2019 time frame as a whole, except for mean research activity, which was reported in its original format.
Descriptive statistical analysis was performed to investigate mean match rates into GS and OS. Independent sample T-tests with the Bonferroni correction were performed to determine any significant differences in (1) application metrics and match rates between male and female ERAS applicants and entering GME residents and (2) application metrics and match rates for all GS and OS ERAS applicants and entering GME residents. IBM SPSS Statistics version 26 (Armonk, New York) was used for data analyses. Statistical significance was defined as P < .05. This study was conducted in compliance with ethical principles, was reviewed by our institutional review board, and was deemed exempt.
Results
26 568 GS and 7076 OS applicants were evaluated and found to have overall match rates of 25.2% and 55.3%, respectively. There were a combined total of 10 591 general and orthopedic female ERAS applicants and 3390 women entering as matched ACGME residents. There were a combined total of 23 044 male general and orthopedic ERAS applicants and 7212 men entered as matched ACGME residents. Women comprised 31.4% of the total applicant pool, whereas men comprised 68.6%. Nine applicants declined gender identification and were not included in gender-specific analyses. Men matched into GS at a rate of 23.0% (3926/17 084), whereas women matched into GS at a rate of 29.2% (2763/9475). Men matched into OS at a rate of 55.2% (3286/5960), whereas women matched into OS at a rate of 56.2% (627/1116).
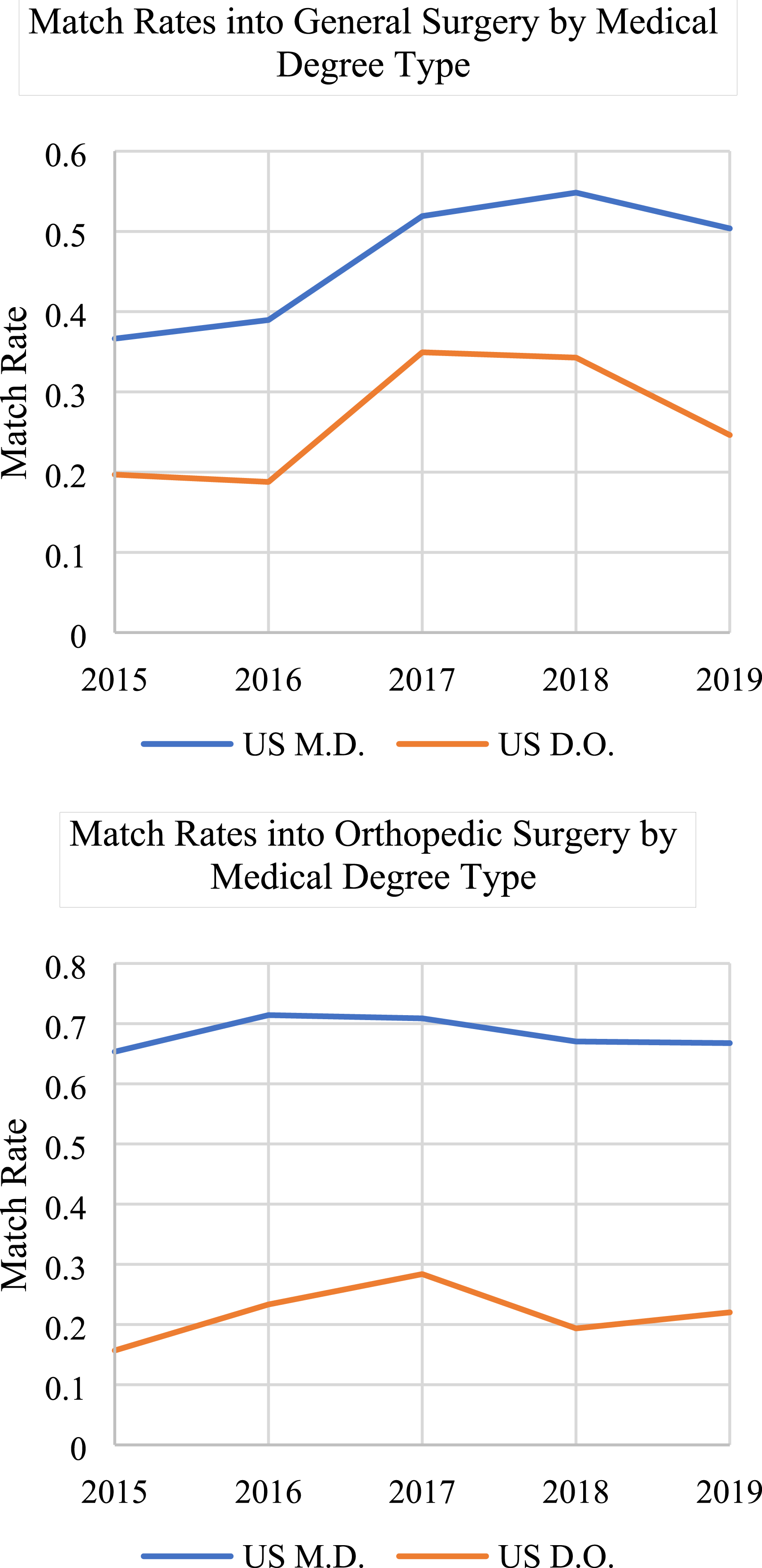
When comparing match rates by gender and applicant degree type, there were no statistically significant differences between men and women for both GS and OS, as shown in Figure 1 (P > .05). Within each gender, US MD men and women matched into GS at a significantly higher mean rate than US Doctor of Osteopathic Medicine (DO) men and women, respectively (eTable 1). When evaluating match rates among all applicants irrespective of gender, US MD applicants experienced significantly higher match rates into both GS and OS than US DO applicants (Figure 2). Mean GS and OS Match Rates by Gender and Applicant Type, 2015-2019. Shown are the mean match rates for male and female US MDs and US DOs into GS and OS. Abbreviations: US, United States; MD, Doctor of Medicine; DO, Doctor of Osteopathic Medicine. Medical Degree Type Match Rates into General and Orthopedic Surgery: (A) US MD applicants matched into general surgery at a significantly higher rate than US DO applicants (46.5% vs. 26.5%; P = .004); (B) US MD applicants matched into orthopedic surgery at a significantly higher rate than US DO applicants (68.3% vs. 21.8%; P < .001) and IMGs (68.3% vs. 8.6%; P < .001). Abbreviations: US, United States; MD, Doctor of Medicine; DO, Doctor of Osteopathic Medicine.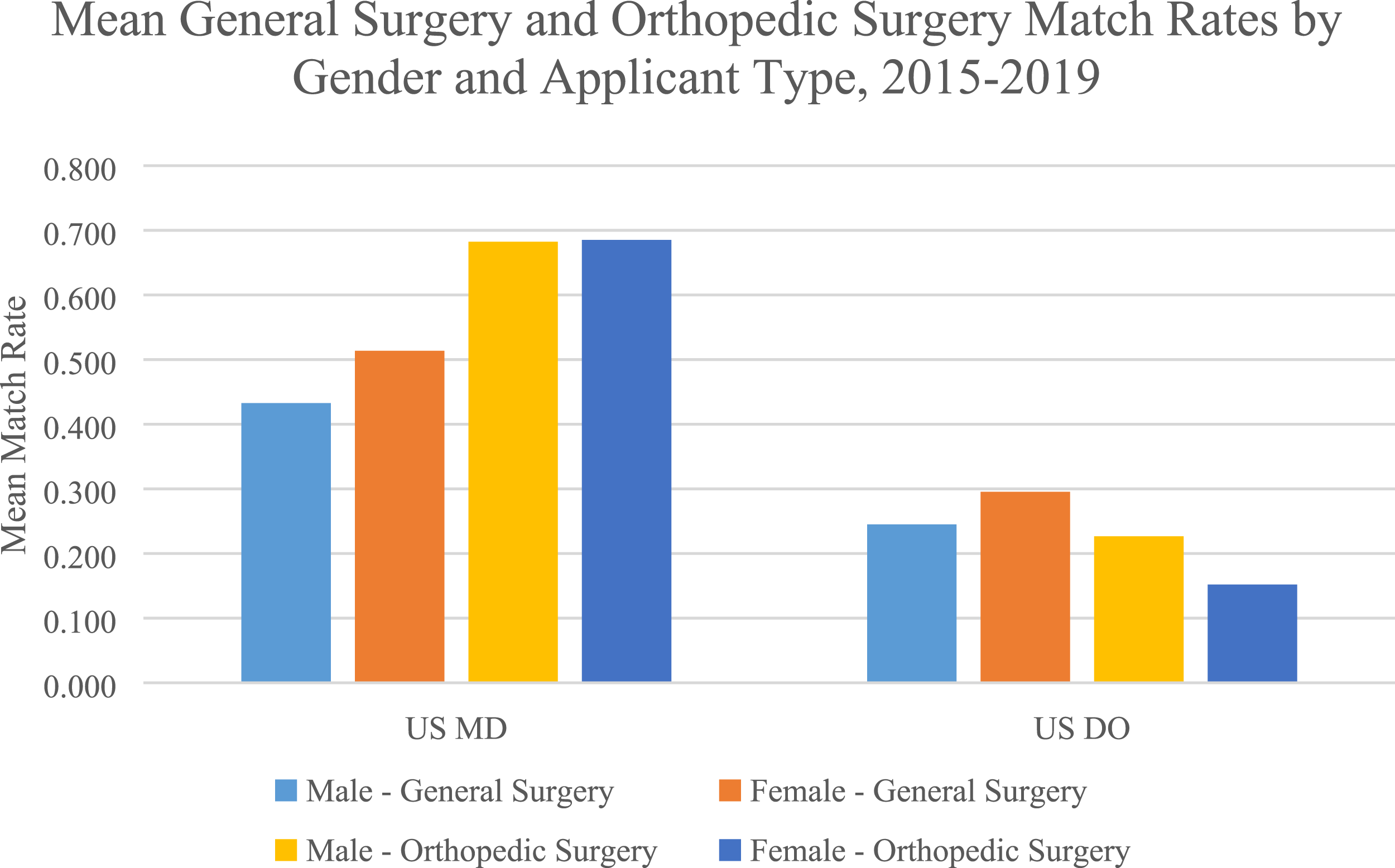
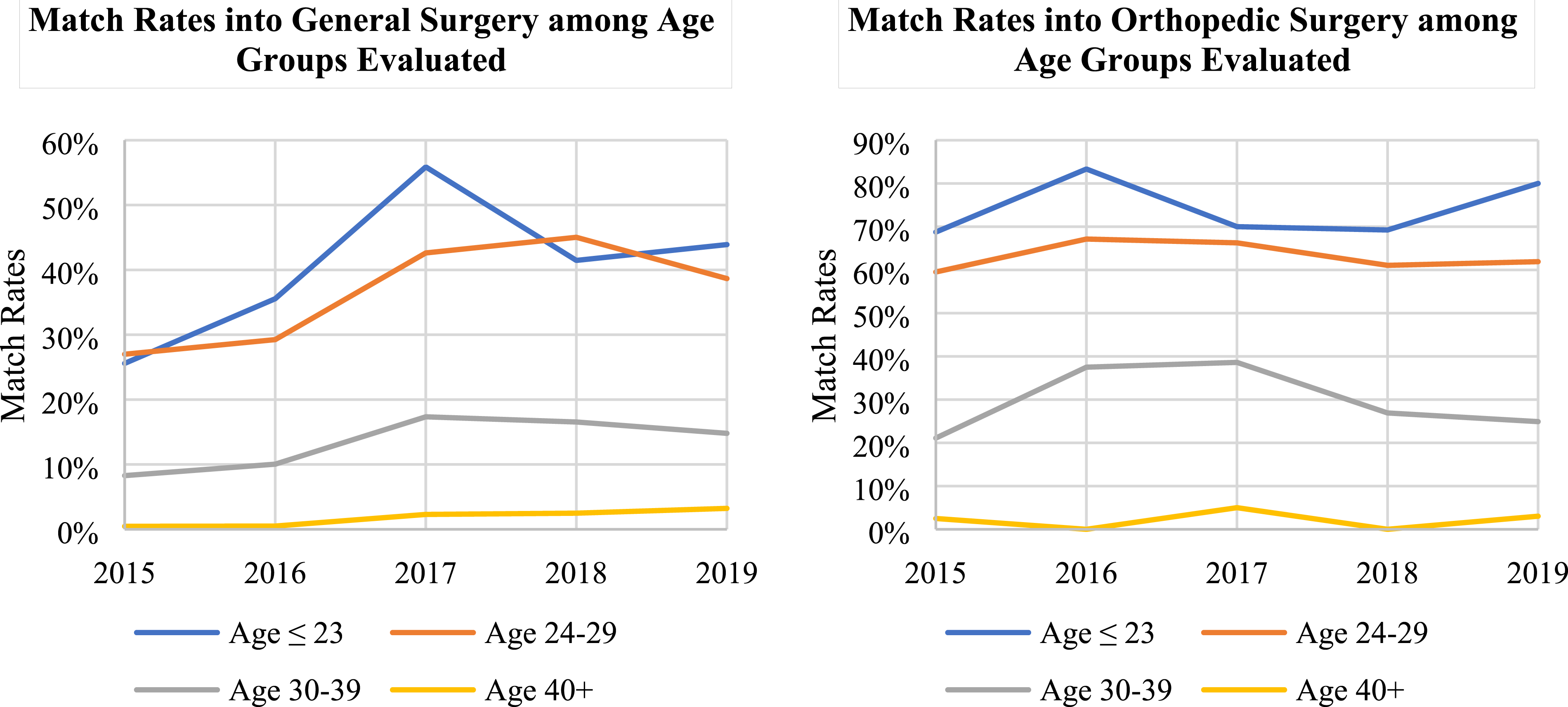
Men aged ≤23 years matched into GS at a significantly higher mean rate than the age-group of 30-35 years and age-group ≥36 years (Figure 3 and eTable 1). Men aged ≤23 years experienced significantly higher mean match rates into OS than the age-groups of 24-29 years, 30-35 years, and ≥36 years. Women aged ≤23 years experienced mean match rates into both GS and OS, which were significantly higher than age-groups of 30-35 years and ≥36 years (eTable 1). Men aged ≥36 years matched into OS at a significantly higher mean rate than women aged ≥36 years (11.9% vs. 1.4%, P = .009). When evaluating match rates among all applicant ages independently of gender, GS applicants ≤23 years matched significantly more than those aged 30-39 years (40.5% vs. 13.4%; P < .001) and those aged ≥40 years (40.5% vs. 1.8%; P < .001) (Figure 4A). A similar trend was seen for OS applicants, with those ≤23 years matching significantly higher than those aged 24-29 years (74.3% vs. 63.2%; P = .012), 30-39 years (74.3% vs. 29.8%; P < .001), and ≥40 years (74.3% vs. 2.1%; P < .001) (Figure 4B). Mean General Surgery and Orthopedic Surgery Match Rates by Gender and Age, 2015-2019. Shown are average match rates for men and women into GS and OS by each age cohort analyzed. A complete list of all age-related trends can be found in eTable 1. Age-Group Match Rates into General and Orthopedic Surgery: (A) general surgery applicants aged ≤23 years matched significantly more than those aged 30-39 years (40.5% vs. 13.4%; P < .001) and those aged ≥40 years (40.5% vs. 1.8%; P < .001). Ages 24-29 years matched more than ages 30-39 years (36.5% vs. 13.4%; P < .001) and ages ≥40 years (36.5% vs. 1.8%; P < .001). Ages 30-39 years matched more than ages ≥40 years (13.4% vs. 1.8%; P < .001); (B) orthopedic surgery applicants aged ≤23 matched more than those aged 24-29 (74.3% vs. 63.2%; P = .012), 30-39 (74.3% vs. 29.8%; P < .001), and ≥40 years (74.3% vs. 2.1%; P < .001). Ages 24-29 years matched more than ages 30-39 years (63.2% vs. 29.8%; P < .001) and ages ≥40 years (63.2% vs. 2.1%; P < .001). Ages 30-39 years matched more than ages ≥40 years (29.8% vs. 2.1%; P < .001).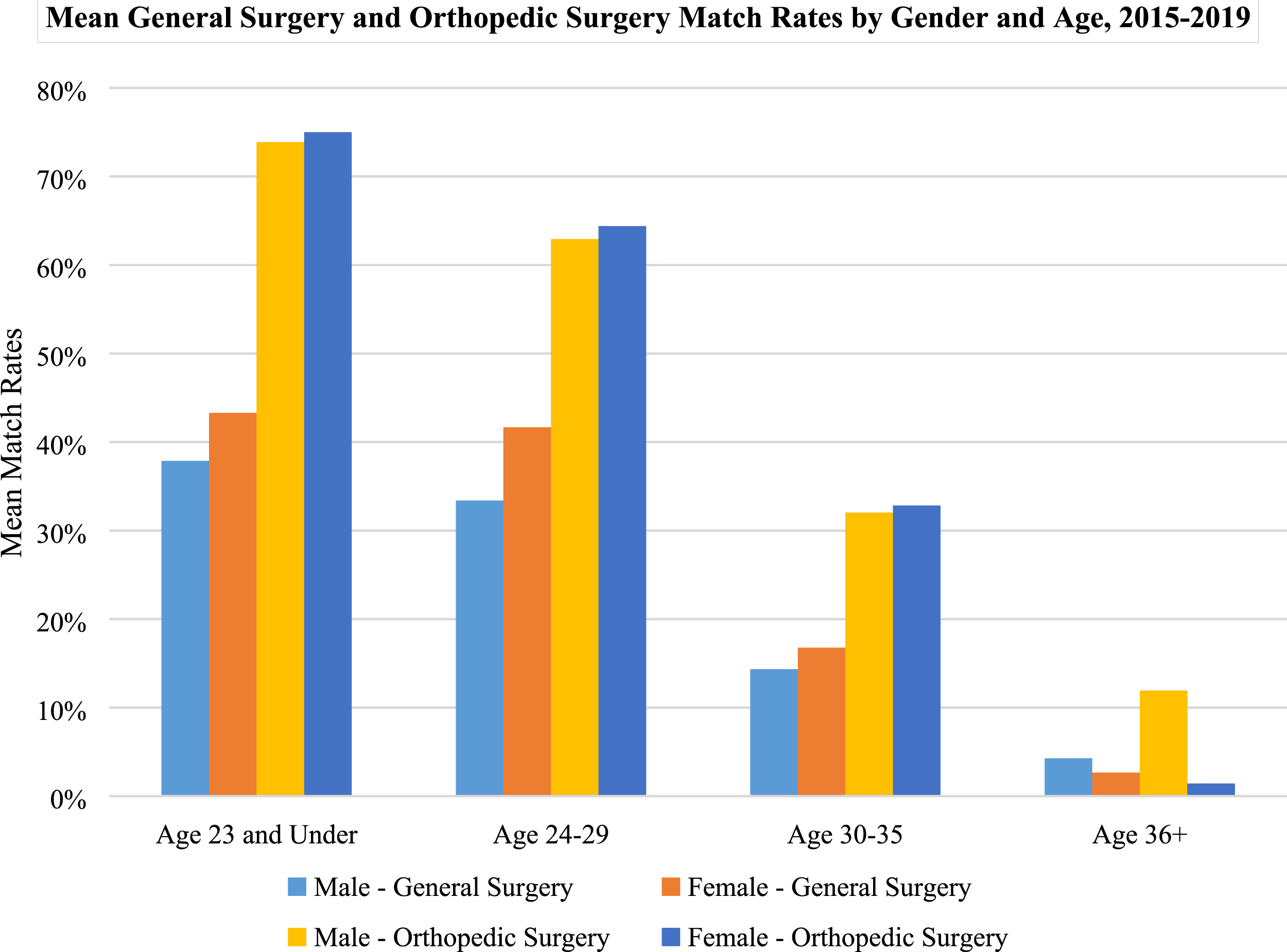
Both male and female first-time applicants experienced significantly higher match rates than reapplicants (Figure 5 and eTable 1). Irrespective of gender, first-time applicants matched at a significantly higher rate than repeat applicants for both GS (36.2% vs. 11.9%; P < .001) and OS (64.9% vs. 21.3%; P < .001). Mean General Surgery and Orthopedic Surgery Match Rates by Gender and Applicant Status, 2015-2019. It can be observed that first-time applicants match at a higher mean rate into general surgery and orthopedic surgery than repeat applicants for both men and women.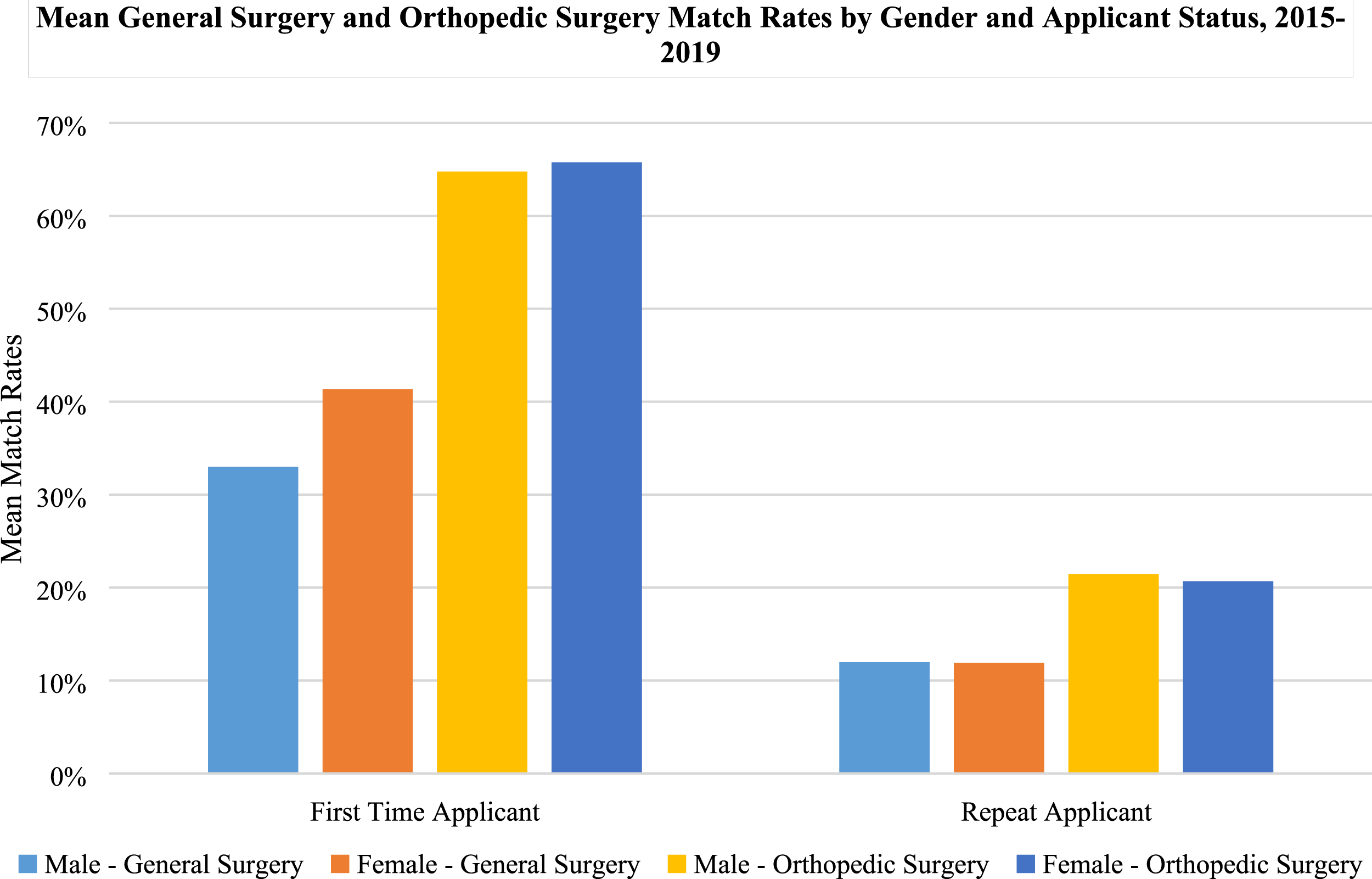
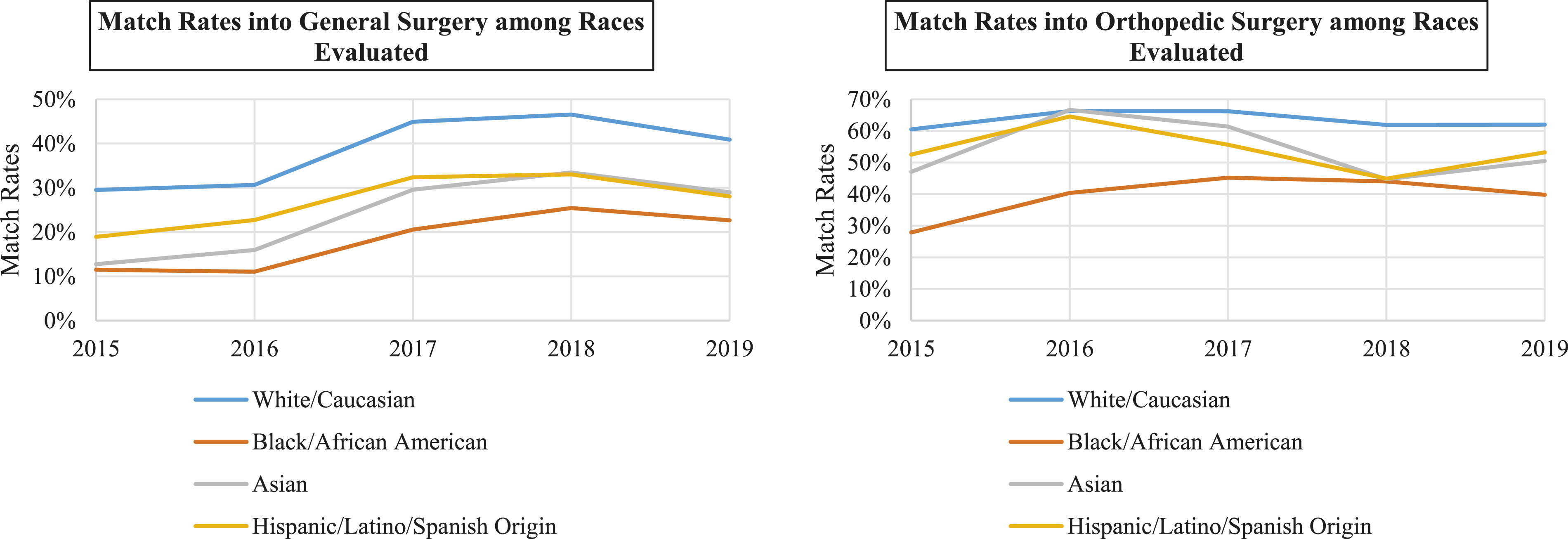
Male non-URMs matched into GS and OS at significantly higher mean rates than URMs (Figure 6 and eTable 1 Mean GS and OS Match Rates by Gender and URM Status, 2015-2019. It can be observed that male and female URMs matched into both general surgery and orthopedic surgery at a lower mean rate than non-URM equivalents. Abbreviation: URM, underrepresented minority. Race/Ethnicity Match Rates into General and Orthopedic Surgery: (A) white/Caucasians matched significantly more into general surgery than black/African Americans (38.5% vs. 18.2%; P = .002), Asians (38.5% vs. 24.2%; P = .03), and Hispanic/Latino/or of Spanish origin (38.5% vs. 27.0%; P = .03); (B) white/Caucasians matched into orthopedic surgery more than black/African Americans (63.4% vs. 39.5%; P < .001) and Hispanic/Latino/or of Spanish origin (63.4% vs. 54.2%; P = .026). Asians matched more than black/African Americans (54.1% vs. 39.5%; P = .024). Hispanic/Latino/or of Spanish origin matched more than black/African Americans (54.2% vs. 39.5%; P = .01).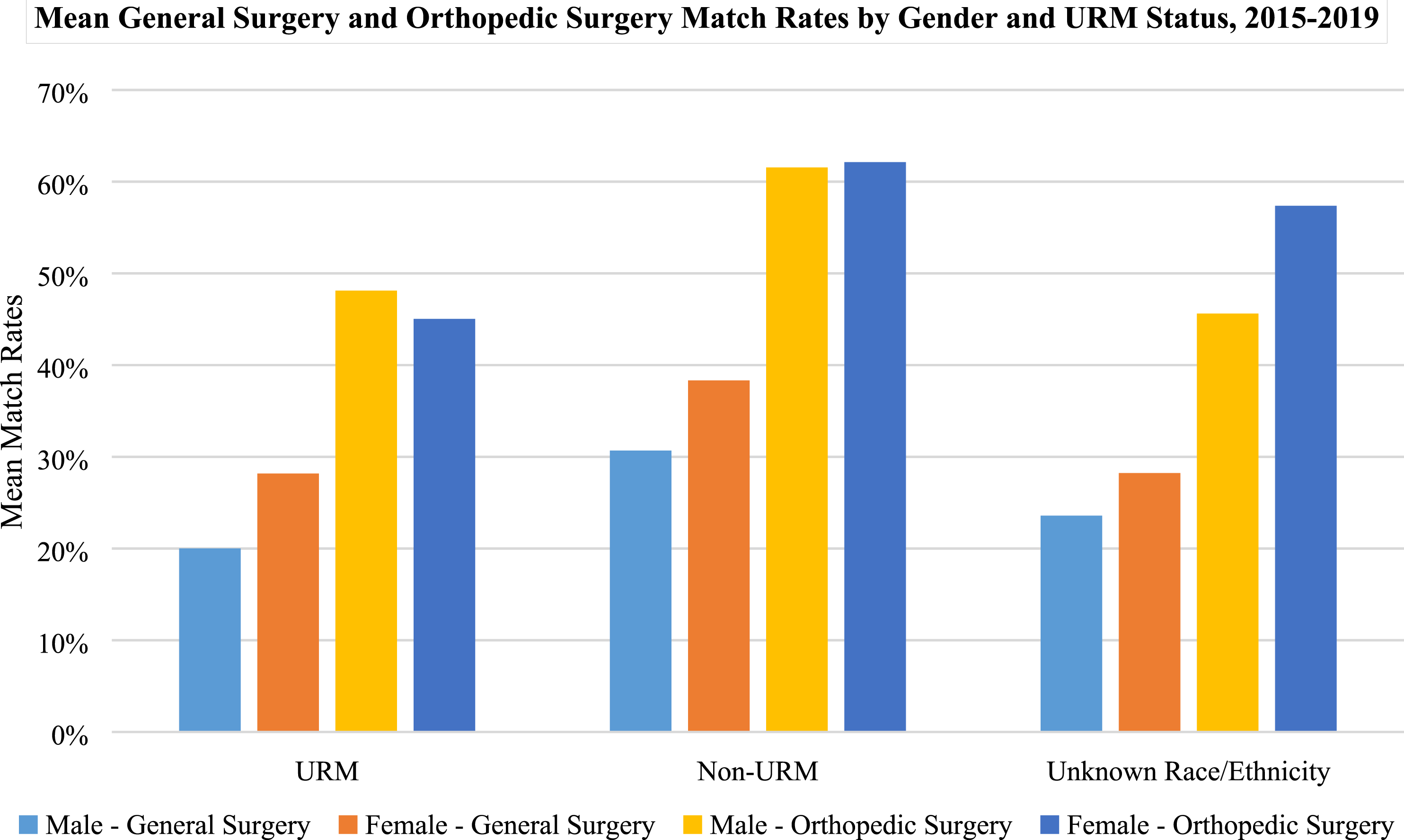
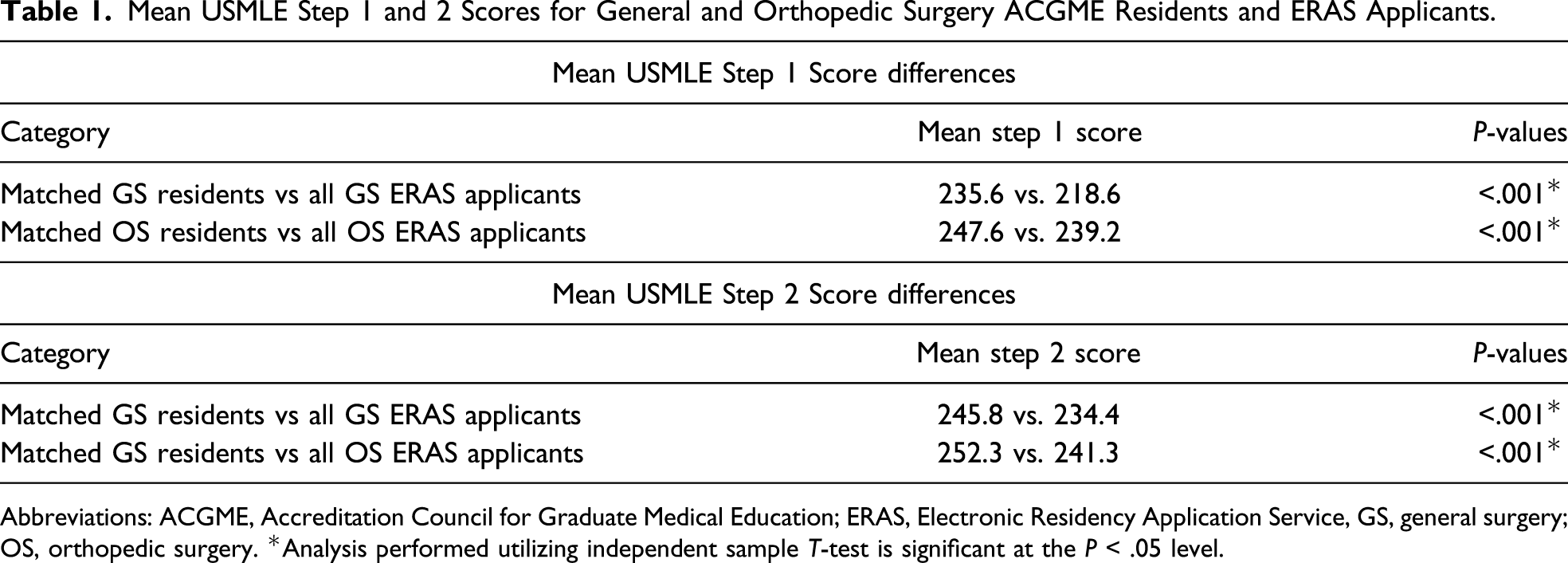
For GS, female ERAS applicants and entering ACGME residents possessed a higher mean number of research experiences than male counterparts (Figure 8 and eTable 1). Within each gender, entering GS male residents possessed a higher mean number of research experiences than male GS ERAS applicants (eTable 1). Entering GS female residents also possessed a higher mean number of research experiences than female GS ERAS applicants (eTable 1). There were no significant differences in the mean number of research experiences between male and female applicants in OS and no significant differences within each gender. Irrespective of gender, entering GS residents had a significantly higher number of research experiences than GS ERAS applicants (2.7 vs. 2.4, P = .014); however, there was no significant difference observed between these cohorts for OS (3.6 vs. 3.7, P = .59). Lastly, mean USMLE Step 1 and Step 2 scores were significantly higher among all entering GS and OS residents than all ERAS GS and OS applicants, respectively (Table 1). Mean Number of Research Experiences of ERAS Applicants and Entering ACGME Residents, 2015-2019. It can be observed that both men and women entering ACGME residents into general surgery and orthopedic surgery have a higher mean number of research experiences than ERAS applicant counterparts. Abbreviations: ACGME, American Council for Graduate Medical Education; ERAS, Electronic Residency Application Service. Mean USMLE Step 1 and 2 Scores for General and Orthopedic Surgery ACGME Residents and ERAS Applicants. Abbreviations: ACGME, Accreditation Council for Graduate Medical Education; ERAS, Electronic Residency Application Service, GS, general surgery; OS, orthopedic surgery. *Analysis performed utilizing independent sample T-test is significant at the P < .05 level.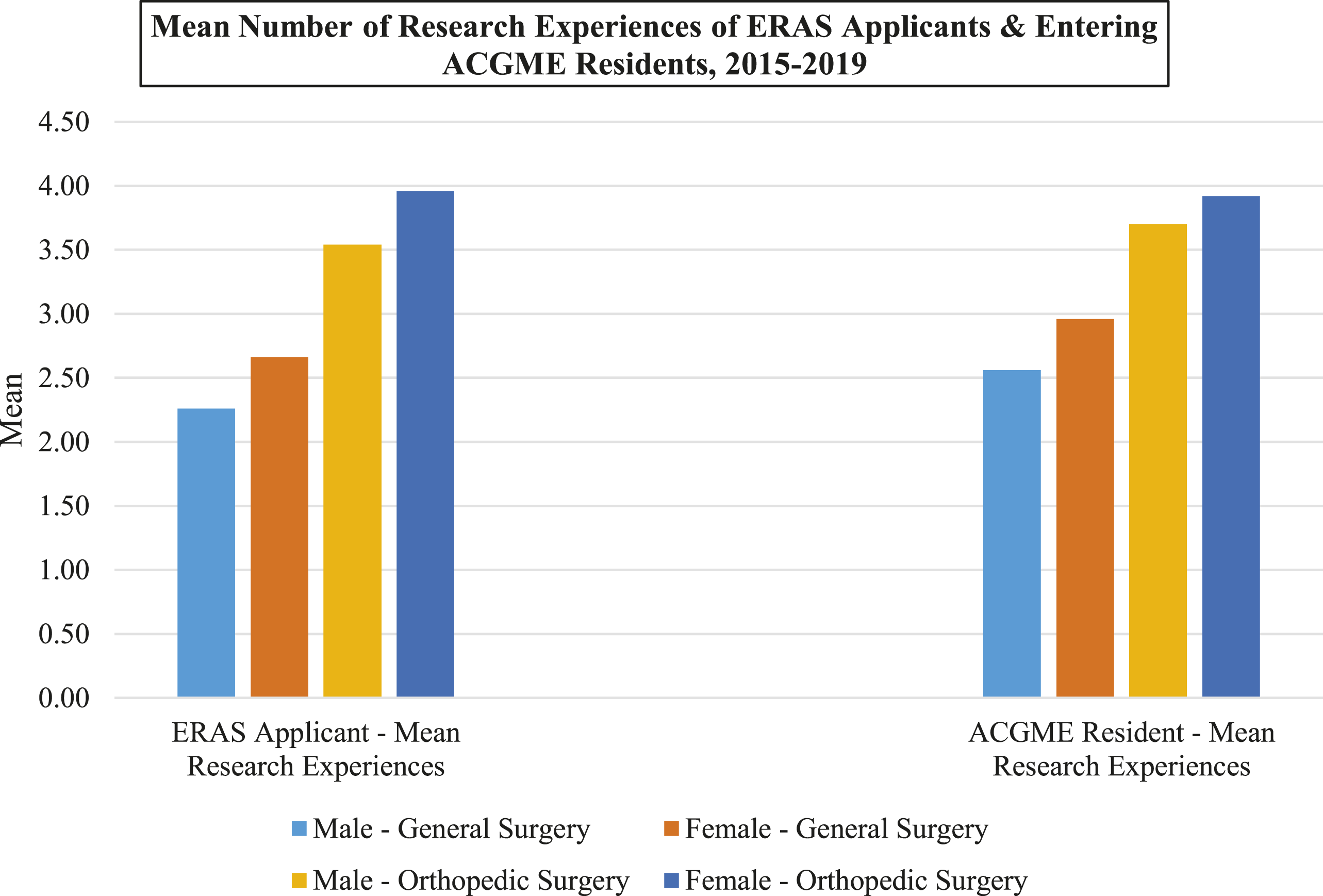
Discussion
It was found that those applicants with younger age, first-time applicant status, higher number of research experiences, higher USMLE Step 1 and Step 2 scores, and of white/Caucasian race matched into GS and OS at higher rates than other applicants. No significant differences were found between match rates of men and women according to applicant type, first-time applicant vs reapplicant status, and URM status in either GS or OS groups. However, it was found that women matched into GS and OS at a higher rate than men. Men aged ≥36 years matched into OS at a significantly higher mean rate than women aged ≥36 years. Finally, female ERAS applicants and entering ACGME residents had a significantly higher mean number of research experiences than male counterparts in GS.
Most of the existing literature investigating the match process primarily concentrates on aspects associated with successful matching. Female gender was associated with lower odds of matching into neurosurgery residency after controlling for relevant application metrics. 9 This is in contrast to investigations from ophthalmology and radiology that concluded there were no associations between gender and successful matching.15,16 Our findings that women matched at higher rates than men into GS and OS may imply that surgical fields may differ in a female applicant’s ability to successfully match and are specialty dependent. Similar analyses should be performed among all specialties to identify potential disparities.
Our data are consistent with the notion that competitive specialties are known to have higher expectations for applicant research experiences by finding that matched GS applicants have significantly more research experiences than GS applicants.14,17 However, our study also showed that female ERAS applicants and entering ACGME residents had a significantly higher mean number of research experiences than entering male counterparts in GS. These findings are in contrast to global trends which have shown that women in academic surgery have less research productivity than their male counterparts. 18 These findings are promising as entering female surgeons will likely serve as role models for prospective applicants and provide opportunities for medical students to participate in research.
Furthermore, our findings demonstrate similar determinants previously associated with matching.14,18,19 Younger age applicants have consistently been shown to be associated with successful matching. 18 The chance of matching into GS and OS decreases as applicants get older as the age-group of ≥40 years had significantly lower match rates than ages ≤23 years, 24-29 years, and ≥36 years. Studies analyzing matching trends in other specialties report similar findings and seem to be in opposition to the nondiscrimination policies established by the ACGME.18,20-22 In contrast to the trends observed in our analysis, a study of anesthesiology applicants found that older age was associated with successful matching, indicating that the role the applicant age plays in the matching process may be variable from specialty to specialty. 20 In our study, men aged ≥36 years experienced significantly higher matching into OS than their female counterparts. One explanation behind these differences could be similarities in the personality and applicant background as the majority of surgical residency program directors are older men. 23 However, the impact of age and differences among age-groups in matching into surgical residencies is a largely under-investigated issue which requires further investigation to elucidate trends observed in this analysis in greater detail.
First-time applicants experienced a higher match rate in both GS and OS than reapplicants. Many unmatched students go on to complete research fellowships or preliminary internships to increase their competitiveness.24,25 Our data show that although these applicants have had a year or more to improve their application, first-time applicants still hold an advantage. Reapplicants should focus on gathering a highly productive research year and develop meaningful faculty relationships at institutions they aspire to match at as it has been shown that 87.5% of successful reapplicants match in a region near their medical school or interim year. 24
Overall, the results from this study suggest that there are multiple factors that are significant for matching into GS and OS residencies of which several are non-modifiable factors such as race and age. Additionally, we found that female and male applicants who successfully match into GS and OS have similar qualifications. The low gender diversity in these fields may be because women comprise a smaller proportion of the applicant pool. Lifestyle considerations have been cited by women as an important factor when making career choices and surgical specialties entail significant time commitments.17,26 Another possible contributor to low numbers of women applying to surgical residencies may be unequal recruitment. Previous literature has mixed conclusions, with certain studies finding that having more women faculty increases the number of female trainees, and others finding no association.7,27-29 Mentorship by women attending surgeons can serve to increase the number of women applying for surgical residencies by fostering interest and insight into these fields.27,30-34 Equally as important as female recruitment is retention of female residents. Previous studies have indicated that women are at a higher risk of leaving GS training than men. 35 Therefore, the low number of female academic surgeons in GS and OS is multifactorial.
Our study has several limitations. We did not have access to individual application metrics which likely play a role in the match process including medical school grades, AOA status, awards, etc. Relatedly, as the AAMC does not directly collect information on unmatched applicants and the NRMP does not release individual data to the public, we were unable to access individual application metrics required for propensity matching multivariable regression. Lastly, the trends observed for GS and OS may not be generalizable to other specialties.
We offer several recommendations moving forward. The low gender diversity in GS and OS is still poorly understood and could be due to the lower numbers of women applicants than men. Future studies should focus on assessing the factors that may be affecting the number of female applicants to surgical fields through extensive surveys. This would help to implement effective new recruitment programs designed at increasing the number of women applying to surgical residencies. Programs sponsored by reputable and nationally recognized organizations such as the American Women Medical Association and Association of Women Surgeons can provide mentorship and research opportunities. Such programs may also aid in connecting medical students and residents to attending physicians remotely and/or in person. Additionally, there is demand for more studies on gender differences in ERAS applicants and entering ACGME residents in order to identify interventions that could reduce inequalities. The collection and release of de-identified applicant metrics such as USMLE scores for public research could allow for the elaboration of differing qualifications, which may allow certain cohorts to improve their application and become more competitive. Moreover, future studies should build upon our analysis by comparing surgical to nonsurgical specialties to determine any gender differences among the variables analyzed and implement interventions to address identified disparities. Relatedly, studies which focus on the applicant ranking process of residency program directors have the potential to elucidate many of the trends observed in this analysis.
Increasing the presence of women in these fields has the potential to foster a healthier and more encouraging environment that promotes women to focus on their surgical education. Additionally, increased representation of women in surgery has the potential to benefit patient outcomes. 36 With a more diverse physician workforce, patients have the ability to choose from a wider variety of diverse providers. Similarly, increased gender diversity and equity can promote the cultural competency of programs that would ideally lead to more effective training, increased patient satisfaction, and a better overall patient experience through greater understanding of, and compliance with, treatment plans.36,37
Conclusions
Although female applicants matched into American general surgery and orthopedic surgery programs at greater rates than their male counterparts from 2015 to 2019, they comprised only 31.4% of all applicants to these fields. Overall, female applicants to both GS and OS had similar qualifications as male applicants. Greater implementation of mentorship opportunities and programs specifically designed to increase the recruitment of female surgical trainees has the capability to reduce the disproportionately low representation of women in surgery. These initiatives have the potential to improve the diversity of the surgical workforce and ultimately improve patient experiences.
Supplemental Material
sj-pdf-1-asu-10.1177_0003134821991982 – Supplemental Material for Gender, Race, Age, Allopathic Degree, Board Score, and Research Experience Among Applicants Matching to General and Orthopedic Surgery Residencies, 2015-2019
Supplemental Material, sj-pdf-1-asu-10.1177_0003134821991982 for Gender, Race, Age, Allopathic Degree, Board Score, and Research Experience Among Applicants Matching to General and Orthopedic Surgery Residencies, 2015-2019 by Mason Sutherland, Carol Sanchez, Amanda Baroutjian, Aleeza Ali, Mark McKenney and Adel Elkbuli in The American Surgeon
Footnotes
Author Contribution
Study design and conception: Adel Elkbuli.
Data collection, interpretation, and analysis: Adel Elkbuli, Mason Sutherland, and Mark McKenney.
Manuscript preparation: Adel Elkbuli, Mason Sutherland, Carol Sanchez, Amanda Baroutjian, Aleeza Ali, and Mark McKenney.
Critical revision of the manuscript: Adel Elkbuli, Mason Sutherland, Carol Sanchez, Amanda Baroutjian, Aleeza Ali, and Mark McKenney.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online