
Abstract

Introduction
Schwannomas are benign, often asymptomatic, slow-growing mesenchymal tumors. 1 Schwannomas are mainly located in the deep muscular layer. 2 Approximately .2% of gastric cancers are schwannomas. 3 They are difficult to differentiate from other submucosal tumors of the stomach preoperatively with a differential including gastrointestinal stromal tumors (GISTs), leiomyomas, and leiomyosarcomas. 1 Due to 10-30% of GISTs showing malignant behavior and the difficulty in preoperatively diagnosing these tumors, surgical resection is recommended to accurately diagnose and treat this spectrum of spindle cell tumors of the stomach. 3 In this study, we present a patient with a mass of the greater curvature of the stomach with a preoperative concern for a neurofibroma who was found to have a gastric schwannoma after robotic-assisted laparoscopic partial gastrectomy.
Presentation
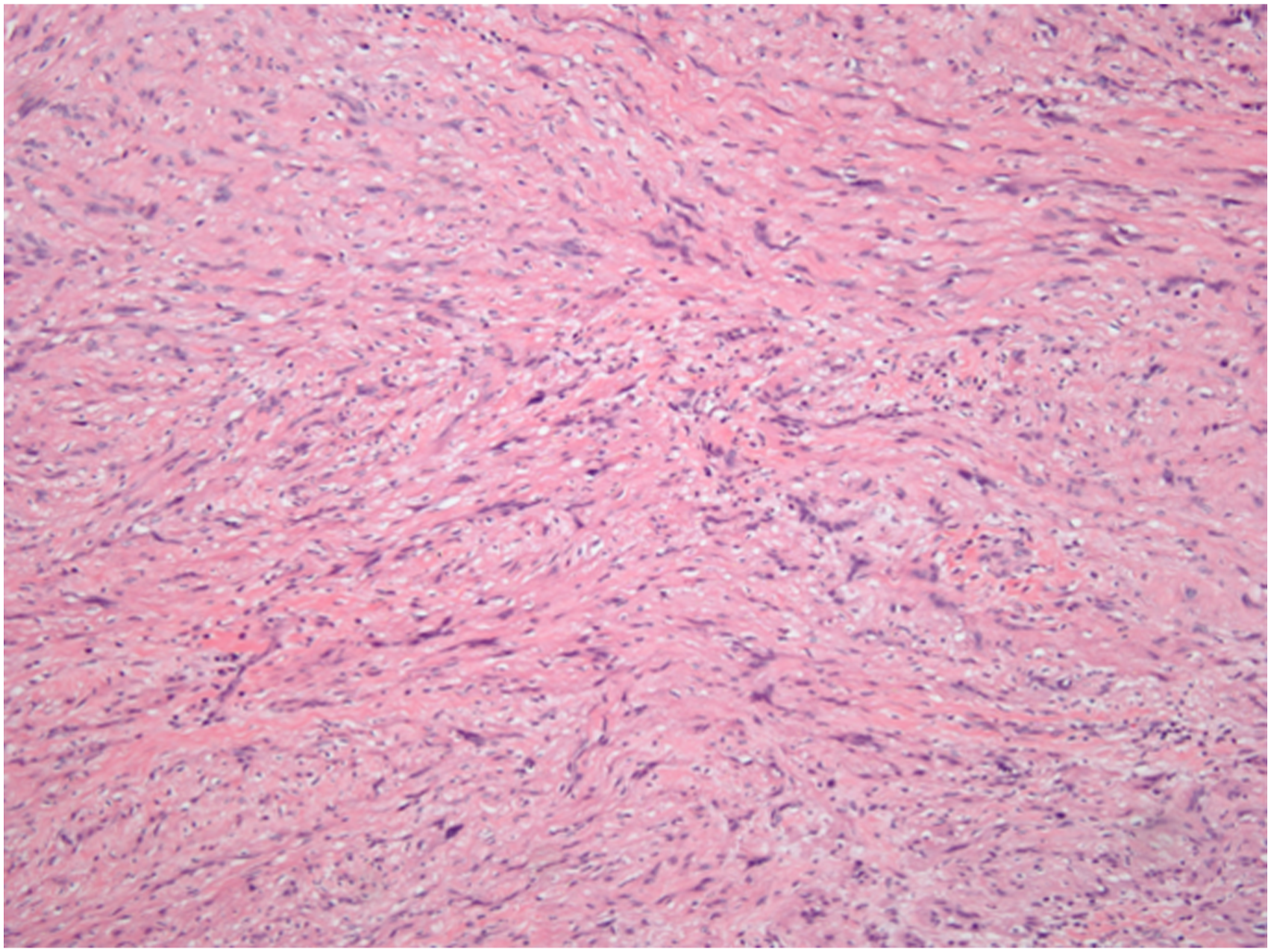
A 35 year-old male patient with past medical history significant for hepatitis C, hypertension, type 2 diabetes mellitus, and gastroparesis presented to his primary care physician for symptoms of fatigue, unintended weight loss, nausea, vomiting, and decreased ability to tolerate solid foods. He had a CT abdomen pelvis with contrast that demonstrated a 3.4 × 2.6 × 2.8 cm oval mass at the greater curvature of the stomach. (Figure 1) He then underwent esophagogastroduodenoscopy (EGD) with biopsy and was found to have grade 2 esophagitis and a 3 cm mass in the gastric body. Biopsies were taken at this time and found to be normal gastric tissue, but there was no submucosal tissue present so it was determined that a repeat biopsy was needed. A repeat EGD with endoscopic ultrasound was performed and showed an intramural lesion that appeared to originate from within the muscularis propria. Fine needle aspiration was performed, and pathology showed spindle cells with wavy serpentine nuclei separated by wire-like collagen fibrils. (Figure 2) The tumor cells stained positive for S100 and negative for CD34 and CD 117. It was determined that this was a neural tumor that favored neurofibroma. CT scan with arrow pointing to gastric mass. Spindle cells.
The patient then underwent genetic testing for neurofibromatosis and was found to be negative. He was then referred to our surgery clinic and was scheduled to undergo laparoscopic resection of this mass. An EGD and robotic-assisted laparoscopic partial gastrectomy was performed without complication.
Pathology of the resected gastric mass showed a 4.6 × 3.2 × 2.8 cm pale tan, well-circumscribed nodule with whorled cute surfaces deep to the mucosa that involves the gastric wall and abuts the pale firm serosa. The nodule was 2 cm from the closest stapled margin. Sections of the specimen showed an unencapsulated spindle cell tumor within the gastric wall composed of elongated spindle cells with tapered nuclei within a collagenous stroma. Mitotic activity was not increased, and a lymphoid cuff partly surrounded the tumor. The tumor stained diffusely positive for S100 and negative for CD117 with only blood vessels staining positive for CD34 and residual smooth muscle staining positive for smooth muscle actin. This all supports a diagnosis of completely excised gastric schwannoma.
The patient did well postoperatively with improvement of his gastroparetic symptoms. His case was discussed at our multidisciplinary tumor board, and it was determined that he required no further treatment.
Discussion
As in our case, preoperative diagnosis of a gastric schwannoma is difficult. Radiographic and endoscopic findings are nonspecific. 3 Gastric schwannomas and GISTs both appear similarly on gross examination and occur predominantly in middle-aged persons. 3 Immunohistochemical studies are required to provide the definitive diagnosis, which necessitates surgical resection. 3
Although gastric schwannomas are benign tumors, surgical resection is considered the mainstay of treatment due to their similarity to GISTs that have a much higher malignant potential. 3 Resecting these tumors also helps prevent complications such as bleeding or pyloric stenosis. 1 Endoscopic resection of gastric schwannomas has been described to be a safe and effective treatment; however, due to the tumor’s location in the deep muscular layer, caution must be exerted as this leads to full-thickness resection of the gastric wall. 2 Surgical resection is based on the anatomical location and size of the tumor. Our patient’s tumor size of 4.6 cm and location on the greater curvature of the stomach made it conducive to a minimally invasive surgical approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.