
Abstract
Peritoneal tuberculosis is a rare form of tuberculosis, which involves parietal and visceral peritoneum, omentum, and intestinal mesentery. Its incidence is increasing in developed countries due to HIV infection and immigration. We present a case of peritoneal tuberculosis in a twenty two-year-old patient misdiagnosed with appendicitis. A laparoscopic surgery was performed showing multiple implants on serosal surfaces and adhesions. Laparoscopic appendectomy and peritoneal biopsies were performed. As peritoneal tuberculosis was suspected, an early antituberculous treatment was initiated. A pathological examination of the samples revealed epithelioid granulomas with a centrale caseous necrosis and acid-fast bacilli. Peritoneal tuberculosis is a challenging diagnosis that can mimic other pathologies and should be kept in mind to establish an early antituberculosis treatment avoiding the high morbidity and mortality associated with a late treatment initiation. In case of suspicion of peritoneal tuberculosis, laparoscopy with guided biopsies is useful for the establishment of a correct diagnosis.
Peritoneal tuberculosis is the most common form of abdominal tuberculosis and involves parietal and visceral peritoneum, omentum, and intestinal mesentery. Peritoneal tuberculosis has a prevalence of 4-10% within cases of extrapulmonary tuberculosis. It is uncommon in developed countries, but its incidence has increased due to human immunodeficiency virus infection and an increase number of immigrants from developing countries. 1 It occurs commonly following reactivation of latent tuberculous foci in the peritoneum due to hematogenous spread from a primary lung focus. 2
There are 2 types of peritoneal infection: The exudative type (with ascites) which is the most frequent type present in the 90% of patients with peritoneal tuberculosis and the more advanced “dry” phase with fibro-adhesive type of lesions, present in the other 10% of patients. 3
We report a case of a 22-year-old African man from Mali who presented to the emergency department with a 1 week history of abdominal pain and distension. Laboratory analysis showed a high protein C reactive of 163.7 mg/L. Abdominal ultrasonography revealed findings compatible with acute appendicitis, so a laparoscopic appendectomy was performed.
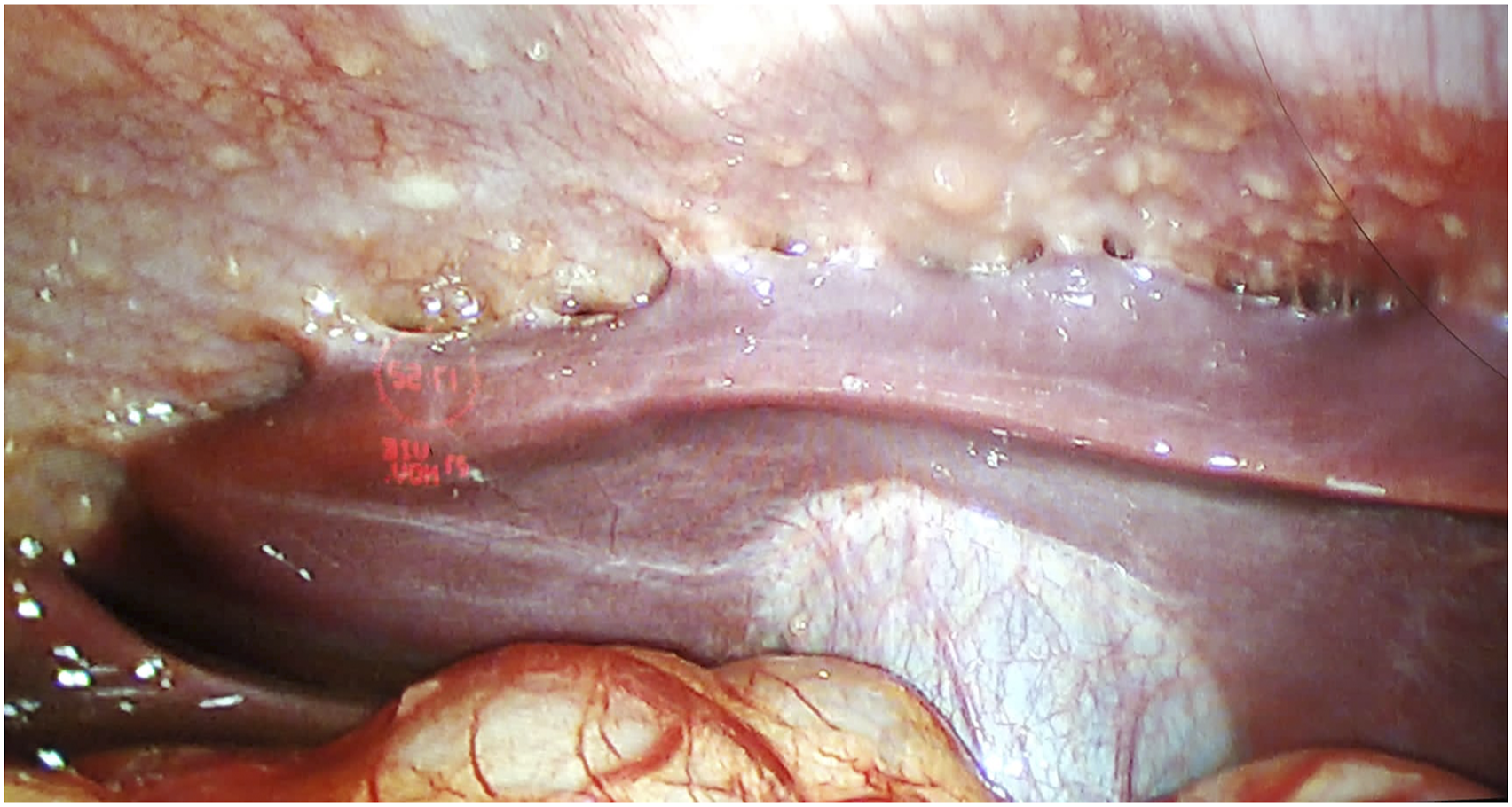
During laparoscopy, multiple nodular implants on the parietal and visceral peritoneal surface were found with adhesions between intestinal loops and the abdominal wall (Figures 1 and 2). Laparoscopic appendectomy and peritoneal biopsy were performed. Peritoneal miliary nodules with adhesions between the small bowel and the parietal peritoneal surface. Miliary nodules and adhesions between the liver and the right subdiaphragmatic surface.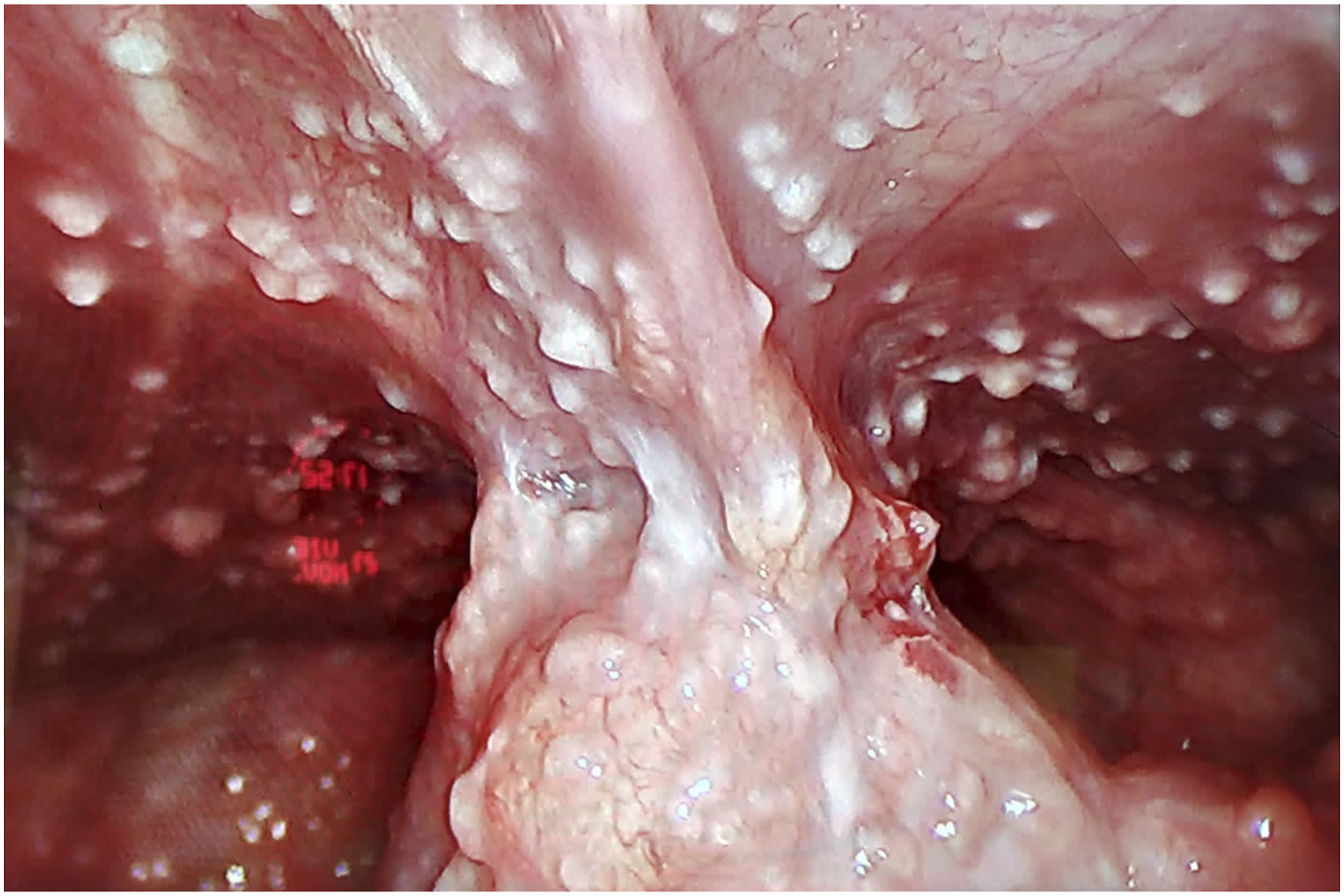
After surgery, a computed tomographic scan with contrast administration showed an extensive peritoneal thickening with ascitic fluid. Sputum analysis and chest radiography were negative. Analysis of ascitic fluid revealed lymphocytosis and a high adenosine deaminase level of 113 U per liter. The results of acid-fast staining and polymerase chain reaction (PCR) testing for Mycobacterium tuberculosis were negative in the ascitic fluid. Pathological examination of the peritoneal implant biopsy sample revealed epithelioid granulomas with a central caseous necrosis with acid-fast bacilli (AFB).
A more exhaustive anamnesis from the patient revealed a previous positive Mantoux test a month previously that was treated with isoniazid. Prompt treatment with a four-drug antitubercular regimen was initiated.
A high suspicion index is needed for an early diagnosis of peritoneal tuberculosis. Symptoms could vary from acute (perforation or obstruction) to chronic nonspecific symptoms such as fever, weight loss, or abdominal distension. Early diagnosis is difficult due to peritoneal tuberculosis mimicking other pathologies such as appendicitis, perforated peptic ulcer, advanced malignancy, or Crohn’s disease. 4
Computed tomography may show ascites and thickening of the parietal and visceral peritoneum. Lymphadenopathy and inflammatory masses may suggest tuberculosis, but there are no pathognomonic radiological findings.
The diagnosis of abdominal tuberculosis may be definitively established by demonstration of Mycobacterium tuberculosis in ascites fluid or in a biopsy sample of an involved site. Histopathology demonstration of caseating granulomas with or without AFB is suggestive but not pathognomonic of tuberculosis. 2
Patients with suspected peritoneal tuberculosis and nondiagnostic ascites fluid analysis should undergo a peritoneal biopsy.
Laparoscopy could be a useful tool for the diagnosis with exploration of abdominal cavity and the performance of a guided biopsy. Classical laparoscopic findings are peritoneal miliary nodules over the visceral and parietal peritoneum, omental thickening, exudative ascites, and adhesions. 1
Guided biopsy samples should be sent for microbiological evaluation as well as histopathology evaluation. The sensitivity of AFB smear and mycobacterial culture for biopsy is low (less than 50%). 2 Polymerase chain reaction is more sensitive and specific for diagnosis of tuberculosis. Histology may show only epithelioid necrotizing gigantocellular granulomas that are suggestive of tuberculosis but not pathognomonic.
In the presence of clinically suspected peritoneal tuberculosis, treatment initiation is recommended without waiting for culture results, which could take a long time. 4 A three-drug regimen with isoniazid, rifampin, and pyrazinamide during 2 months, followed by 4 months of isoniazid and rifampin, is the standard treatment. A fourth drug, usually ethambutol, or a fifth, such as streptomycin, may be added to the initial 2-month intensive phase if drug resistance is suspected as was in our case due to previous treatment with isoniazid alone. Compliance with medical treatment is sometimes a problem and may alter the outcome. 1
Peritoneal tuberculosis is a challenging diagnosis that can mimic other pathologies and should be kept in mind to establish an early antituberculosis treatment avoiding the high morbidity and mortality associated with a late treatment initiation. In case of suspicion of peritoneal tuberculosis, laparoscopy with guided biopsies is useful for the establishment of a correct diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.