
Abstract
Background
Diagnosis of acute mesenteric ischemia (AMI) in its early stages is important for reversing ischemic damage. The CRP to albumin (CRP/Alb) ratio has been defined as an inflammatory indicator and is associated with the severity of inflammation and mortality rates. However, the prognostic value of CRP/Alb has not been evaluated in patients with AMI. Here, we aimed to examine the prognostic significance of CRP/Alb and compare it with other inflammatory markers.
Materials and Methods
In this retrospective, case-control study, we included patients diagnosed with AMI at the emergency department between January 1, 2016, and December 31, 2020. In addition to demographic characteristics, lactate, D-dimer, white blood cell (WBC), CRP/Alb, and neutrophil/lymphocyte ratio (NLR) were recorded. Testing characteristics of CRP/Alb in predicting in-hospital mortality were studied.
Results
The mean age of 132 patients was 66.48 ± 15.95 years and 71 (53.8%) of them were male. The cut-off value obtained using the receiver operating characteristic (ROC) curve for in-hospital mortality was a CRP/Alb ratio of >1.32 (sensitivity, 93.65%; specificity, 69.57%; +LR, 3.08; −LR, .091; AUC, .782; 95% CI, .70-.85; P < .0001). The comparison of ROC curves between CRP/Alb and WBC, NLR, and lactate revealed a statistically significant difference (P < .05), whereas there was not any statistically significant difference between the ROC curves of CRP/Alb and D-dimer (P = .47).
Conclusion
C-reactive protein/albumin ratio is a powerful predictor of in-hospital mortality for AMI patients. It was superior to WBC, NLR, and lactate. It could be used to determine low-risk patients and help clinicians with treatment options.
Keywords
Key Takeaways
CRP/Alb ratio is a powerful predictor of in-hospital mortality. It is superior to WBC, NLR, and lactate. It could be used to determine the low-risk patients.
Introduction
Acute mesenteric ischemia (AMI) is a rare and fatal condition that can lead to intestinal necrosis, peritonitis, severe sepsis, and multi-organ failure. 1 The incidence increases by up to 18% in patients over 65 years of age. 2 Mortality rates are over 50% and often related to delayed admission to the emergency department (ED), non-specific clinical findings, and delayed differential diagnosis and surgical intervention. 3 Diagnosis of AMI in its early stages is important for reversing ischemic damage. The mortality rate can be decreased by 20% with surgical intervention in the first 6 hours; however, a 24-h delay in surgical intervention is associated with mortality rates reaching 79%–100%.4,5
The standard diagnostic tool for AMI is computed tomography (CT) with 94% of sensitivity and 95% specificity. 6 In addition to CT, the use of biochemical parameters may improve the diagnostic process, care provided, and prognosis of AMI. Citrulline, intestinal fatty acid-binding protein, α-glutathione S-transferase, L-lactate, D-lactate, D-dimer, white blood cell (WBC) count, neutrophil to lymphocyte ratio (NLR), and procalcitonin were examined as biomarkers of AMI.7-12
C-reactive protein (CRP) and albumin are acute phase reactants synthesized by the liver and associated with the severity and prognosis of inflammation.13,14 The CRP to albumin (CRP/Alb) ratio has been defined as an inflammatory indicator and is associated with the severity of inflammation and mortality rates. 15 Recent studies have reported that it may also be an inflammatory marker in acute pancreatitis, cancer, major abdominal surgery, ulcerative colitis, and hip fractures.16-20 However, the prognostic value of CRP/Alb has not been evaluated in patients with AMI. Here, we aimed to examine the prognostic significance of CRP/Alb and compare it with other inflammatory markers, such as WBC, NLR, lactate, and D-dimer.
Methods
This retrospective case-control study was carried out between January 2016 and December 2020 in the ED of Aksaray University Training and Research Hospital. Local ethical committee approval was obtained before starting the study (Decision no. 2021/04-25).
Study Design and Patient Selection
The medical data of patients diagnosed with AMI in the ED between January 1, 2016, and December 31, 2020, were retrospectively reviewed. Patients with missing data, those younger than 18 years, and those with a Glasgow Coma Scale score of 3 at admission to the ED were excluded from the study. In addition, patients who had inflammatory bowel disease, colorectal cancer, celiac disease, or hematological malignancies were excluded to avoid confounders in biomarker interpretation.
The demographic characteristics, body mass index (BMI, kg/m2), Charlson Comorbidity Index, history of any kind of embolism/thrombosis (deep vein thrombosis, pulmonary embolism, acute myocardial infarction, or ischemic stroke), history of abdominal surgery, electrocardiography (ECG), length of stay in an intensive care unit, the total length of stay in the hospital, and in-hospital mortality were recorded. Lactate, D-dimer, complete blood count, CRP, and albumin levels at the time of admission to the ED (earliest) were also evaluated, and CRP/Alb and NLR were calculated. Lactate levels were biochemically measured in venous blood gas (.3-1.3 mmol/L), and D-dimer (0-.5 μg/mL), CRP (0-5 mg/L), albumin (35-52 g/L), leukocyte (4-10 109/L), neutrophil (2-7 109/L), and lymphocyte (.8-4 109/L) levels were measured in blood plasma samples. The primary endpoint of the study was in-hospital mortality.
Statistical Analysis
Data were analyzed using MedCalc Statistical Software version 19.1 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2020). The Kolmogorov-Smirnov test was used to determine distribution normality. Continuous data were presented as mean ± SD for normally distributed variables and as median and interquartile range (IQR) for non-normally distributed variables. Categorical data were presented as n (%).
The primary endpoint was in-hospital mortality. Factors affecting mortality were compared using chi-square or Fisher’s exact test for categorical variables and using Student’s t test or the Mann-Whitney U test for numerical variables. The performance characteristics (area under the curve, sensitivity, specificity, predictive values, and likelihood ratios (LRs)) of WBC, NLR, CRP/Alb, lactate, and D-dimer levels in terms of predicting in-hospital mortality of AMI cases were analyzed using receiver operating characteristic (ROC) curves. The cut-off values were determined using Youden’s index. Receiver operating characteristic curves of these parameters were compared by the DeLong method using MedCalc Software version 19.1 (MedCalc Software Ltd). All patients were divided into 2 groups using the WBC, NLR, CRP/Alb, lactate, and D-dimer cut-off values. Univariate logistic regression analyses were performed to determine risk factors for in-hospital mortality. Parameters with P < .2 in the univariate logistic regression analyses were included in the multivariate model. P < .05 was considered statistically significant for all analyses.
Results
A total of 151 patients diagnosed with AMI in the ED were eligible for the study. Three patients with hematological malignancies, two patients with colorectal cancer, one patient with celiac disease, one patient with inflammatory bowel disease, and 12 patients with missing data were excluded from the study. Finally, 132 patients were included in the study.
Demographics and Laboratory Findings of the Study Population.
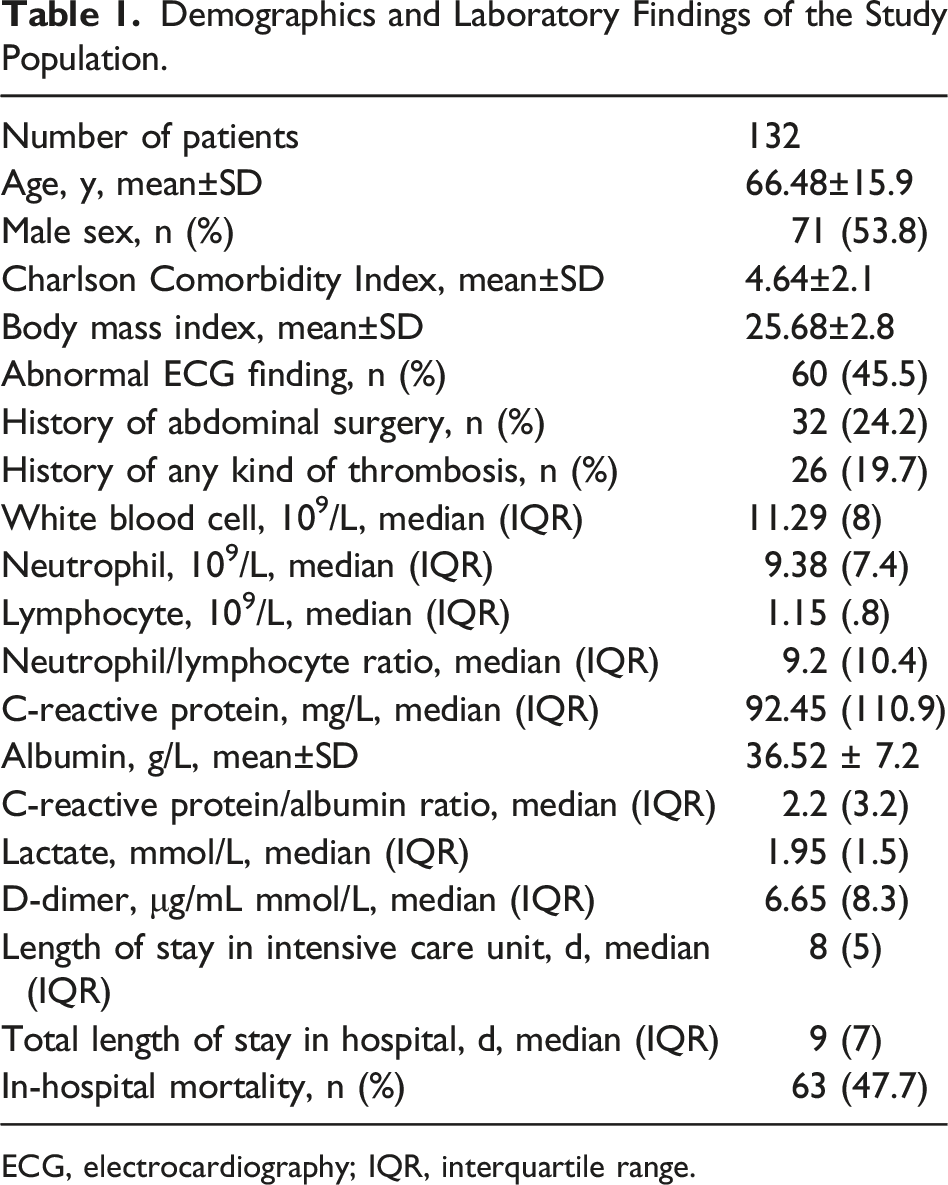
ECG, electrocardiography; IQR, interquartile range.
Comparison Between Patients Who Survived and Those Who Died.
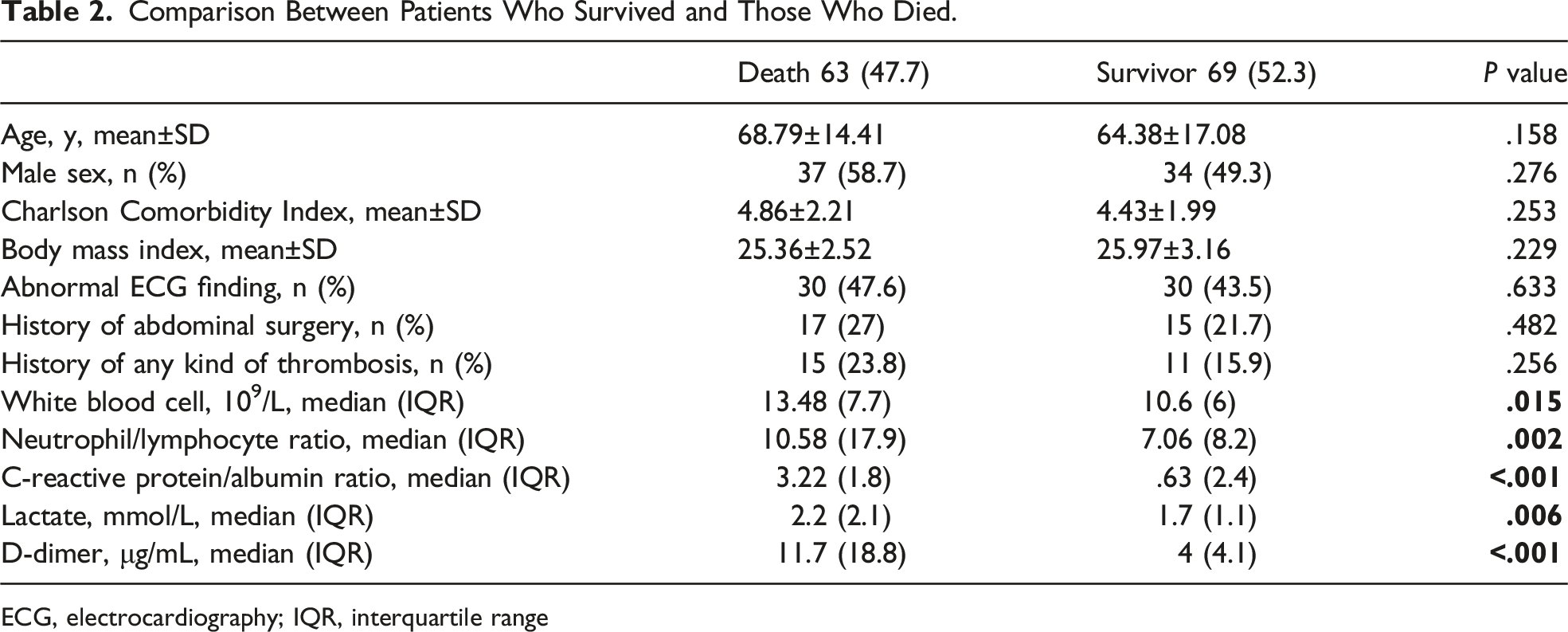
ECG, electrocardiography; IQR, interquartile range
The Performance Characteristics of WBC, NLR, CRP/Alb, Lactate, and D-Dimer in Predicting In-Hospital Mortality.
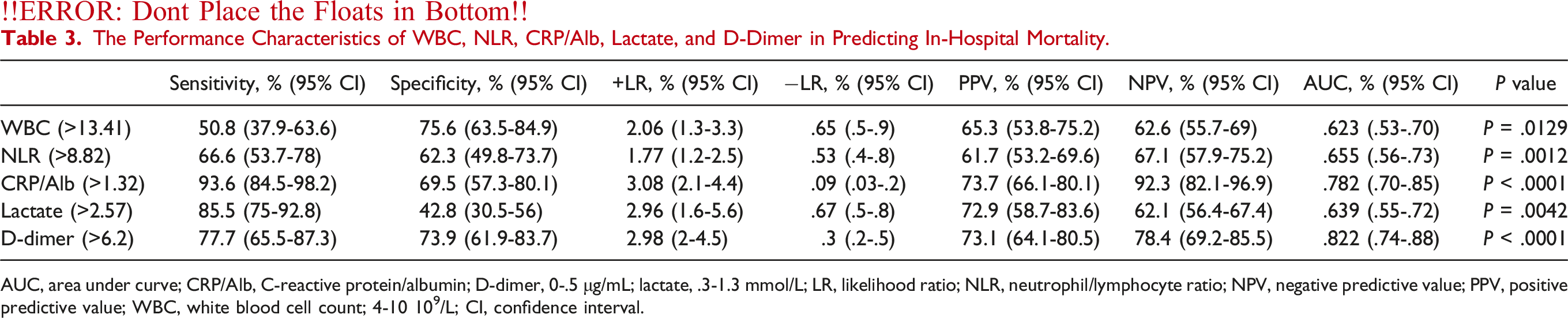
AUC, area under curve; CRP/Alb, C-reactive protein/albumin; D-dimer, 0-.5 μg/mL; lactate, .3-1.3 mmol/L; LR, likelihood ratio; NLR, neutrophil/lymphocyte ratio; NPV, negative predictive value; PPV, positive predictive value; WBC, white blood cell count; 4-10 109/L; CI, confidence interval.
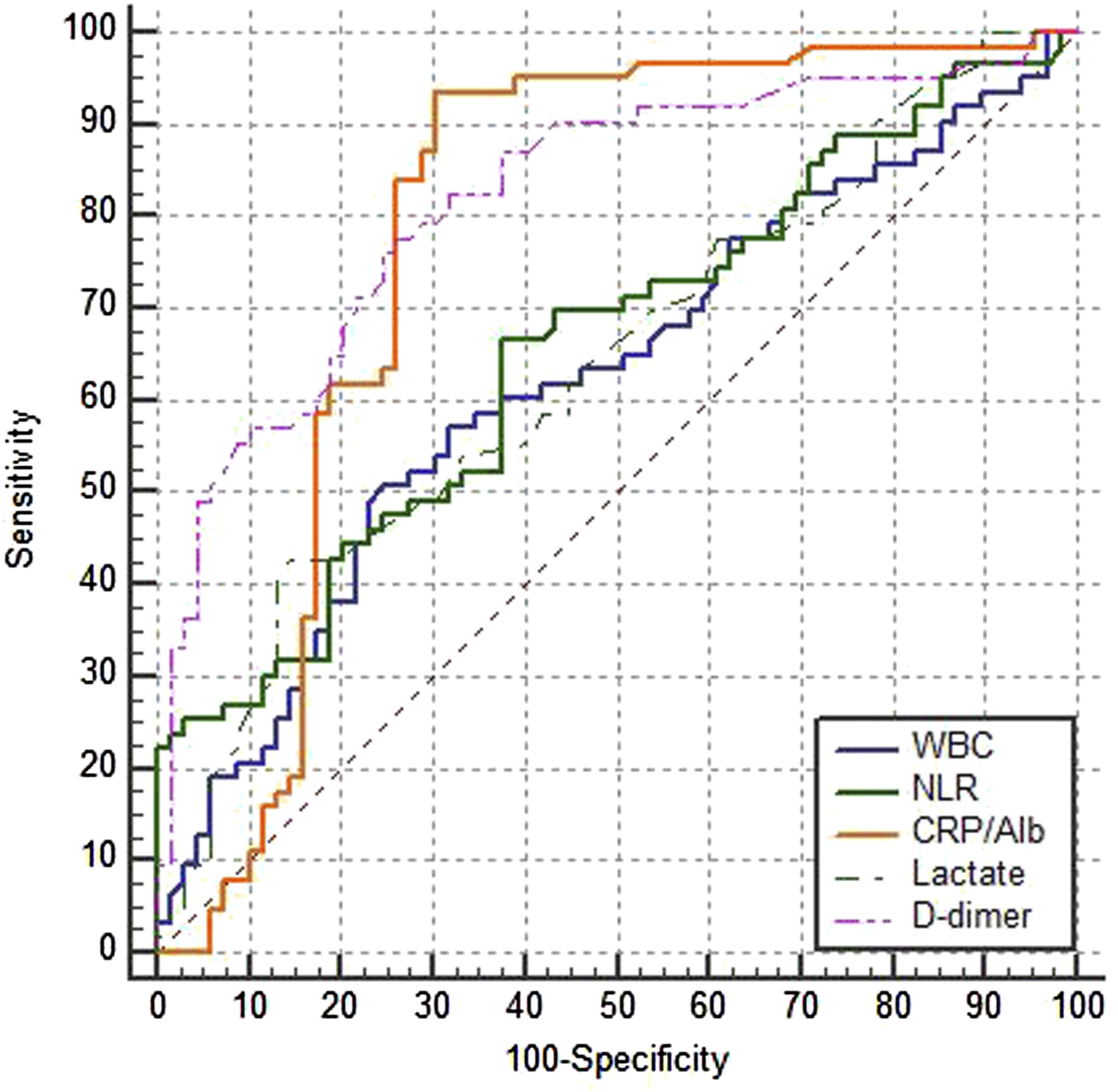
Comparison of ROC curves of WBC, NLR, CRP/Alb, lactate, and D-dimer. ROC, receiver operating characteristic; WBC, white blood cell; NLR, neutrophil/lymphocyte ratio; CRP/Alb, C-reactive protein/albumin.
Logistic Regression Analysis for Mortality Predictors.
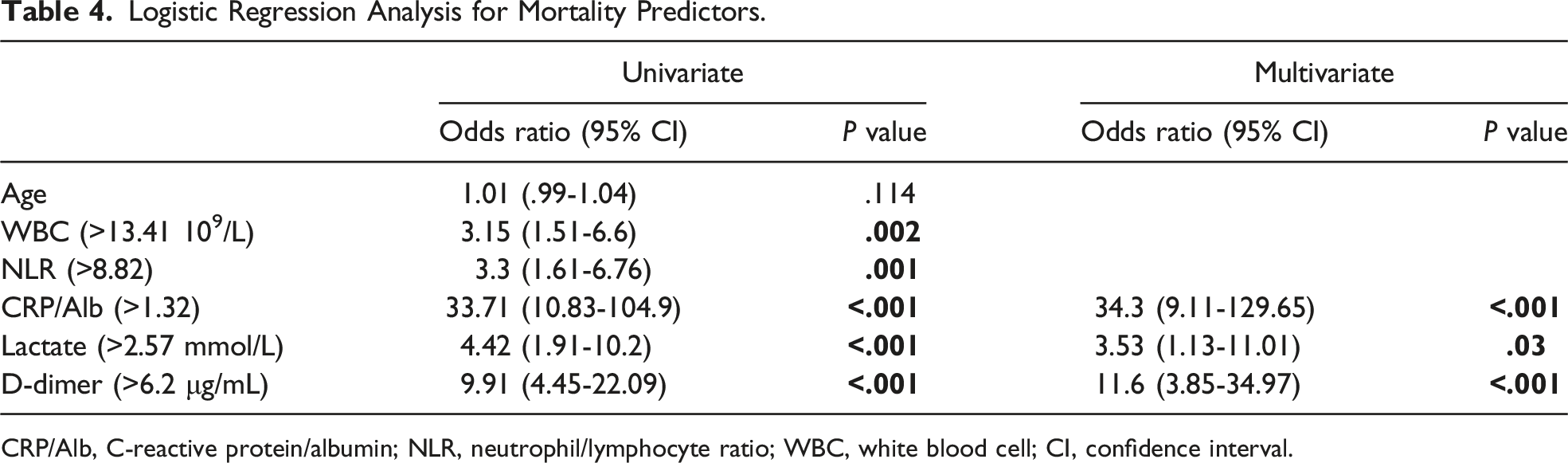
CRP/Alb, C-reactive protein/albumin; NLR, neutrophil/lymphocyte ratio; WBC, white blood cell; CI, confidence interval.
Discussion
In this study, we investigated the ability of CRP/Alb to predict short-term mortality of AMI patients diagnosed in the ED. Thus, CRP/Alb can be used to determine low-risk patients (negative predictive value 92.3%). In cases where CRP/Alb>1.32, there is an increased possibility of short-term mortality with high sensitivity [93.6% (95% CI, 84.5-98.2)] and a high +LR [3.08 (95% CI, 2.1-4.4)]. Both CRP and albumin are screened in patients with AMI, and they certainly have important individual roles in predicting AMI prognosis.7-9 According to the results of this study, they can be combined as a tool for risk stratification in AMI.
Kim et al 21 reported that CRP/Alb (with a cut-off value of 5.09) was superior to CRP level in predicting mortality in patients with septic shock. There was a significantly higher 180-day mortality rate in patients with CRP/Alb>5.09 compared with patients with lower CRP/Alb. Kaplan et al 17 investigated the prognostic value of CRP/Alb among patients with acute pancreatitis. They showed that patients with CRP/Alb≥16.28 had a 19.3 times higher risk of death compared with patients who had CRP/Alb<16.28. In our study, CRP/Alb>1.32 was an independent risk factor for in-hospital mortality. Patients with CRP/Alb>1.32 had a 34.3-fold higher risk of in-hospital mortality.
Acute mesenteric ischemia patients often present with leukocytosis, metabolic acidosis, and elevated serum D-dimer and lactate levels. All these parameters are important factors in the diagnosis and prognosis of AMI patients. Although leukocytosis is an important inflammatory response in AMI, it has poor sensitivity and specificity for AMI diagnosis. Aktimur et al 22 reported that a WBC value higher than 14.4 had 57.1% sensitivity and 69.3% specificity for diagnosis of AMI, but it was not correlated with ischemia length and poor prognosis. In our study, WBC had low sensitivity (50.8%), as expected; however, it had higher specificity (75.6%) compared with the literature. In addition, it was not a significant predictor of in-hospital mortality according to the multivariate logistic regression analysis.
In recent years, NLR has been investigated as a diagnostic and prognostic factor among AMI patients. Wang et al 11 reported that NLR (with a cut-off value of 11.05) had an 80.4% sensitivity and 82.6% specificity in predicting poor outcomes in AMI patients. In addition, they demonstrated that the relative risk of death was 7.57 among AMI patients who had NLR values >11.05 compared with patients who had NLR values <11.05 by multivariate logistic regression analysis. Tanrikulu et al 23 reported that NLR had a sensitivity of 74.1% and a specificity of 88.7% in comparison with the control group in the diagnosis of AMI. However, compared with non-vascular bowel disease patients, NLR had poor sensitivity and specificity of 50% and 66.1%, respectively. In the present study, NLR had low sensitivity (66.6%) and specificity (62.3%) in predicting in-hospital mortality. In addition, NLR had the lowest positive predictive value (61.7%) among the 5 parameters, and it was not a significant prognostic factor in the multivariate logistic regression analysis.
Similar to WBC values, it is considered that serum lactate levels are a helper in the diagnosis of AMI, but many factors can cause an elevated serum lactate level; therefore, it cannot be used effectively in the differential diagnosis of abdominal emergencies. Studer et al 10 investigated the predictive value of lactate levels on the amount of bowel affected by ischemia. Although serum lactate levels were significantly higher in the presence of necrotic bowel above 50 cm, there was not a statistically significant increase below 50 cm. Lactate levels often increase in the last stage of AMI. Thus, because of its lower specificity, L-lactate is not a potential candidate as an early diagnostic marker of AMI. 24 In this study, lactate drew our attention with its high sensitivity (85.5%), but it exhibited the expected low specificity (42.8%) in predicting in-hospital mortality of AMI patients. It had the lowest negative predictive value (62.1%) among the 5 parameters. Although the risk of death was predicted by lactate levels of 3.53 (with a cut-off value of 2.57), it was significantly lower than that of CRP/Alb (34.3).
D-dimer, a fibrin degradation product, is usually increased in arterial or venous occlusive conditions and in other inflammatory and infectious diseases; therefore, it has high sensitivity (96%) and low specificity (40%) in predicting a diagnosis of AMI. 24 A negative D-dimer value has a strong −LR and may be helpful in ruling out AMI, but the data are insufficiently robust to recommend full exclusion of the disease. 6 In this study, D-dimer had a lower sensitivity (77.7%) and a higher specificity (73.9%) compared with the literature. However, it had the second-highest negative predictive value of 78.4% and could be used for ruling out in-hospital mortality in AMI patients, according to our results.
Although the specificity of CRP/Alb was 69.5%, it had the highest sensitivity (93.6%), highest +LR (3.08), highest positive predictive value (73.7%), and highest negative predictive value (92.3%) in predicting in-hospital mortality among AMI patients. In line with these results, the testing characteristics of CRP/Alb for predicting an AMI diagnosis and the length of ischemic bowel among AMI patients can be the focus of future studies.
Limitations
Potential weaknesses of this study include its retrospective nature. Because of this, the time spent before admission and the time from admission to surgery could not be evaluated. Clearly, delayed admission to the ED and delayed surgical intervention are important risk factors for in-hospital mortality of AMI patients. 3 In addition, the length of the ischemic bowel could not be evaluated and correlated with CRP/Alb because of the lack of histopathologic data. The lack of data about the other laboratory evidence of multi-organ failure is another limitation of this study. The power of the CRP/Alb ratio in predicting mortality among AMI patients could have been better understood with multi-organ failure biomarkers. Further studies are needed to investigate the correlations between delayed admission and delayed surgical intervention and biomarkers and the length of the ischemic bowel.
Conclusions
C-reactive protein/albumin is a powerful predictor of in-hospital mortality for AMI patients. It was superior to WBC levels, NLR, and lactate levels. It could be used to determine low-risk patients and help clinicians decide on treatment options. It is a simple, cheap, and readily available test to aid in the early prediction of poor outcomes. The early identification of high-risk patients can help to reduce the time between admission and surgical intervention and avoid an increase in the length of the ischemic bowel.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.