
Abstract
Background
Accurate and timely injury identification is critical but difficult to achieve in trauma patients who die shortly after arrival to the hospital. Autopsy has historically been used to detect injuries, but few undergo formal autopsy. This study investigates the utility of post-mortem computed tomography (PMCT) for injury identification in a diverse trauma population.
Methods
Cross-sectional study of adult trauma patients who died within 24 hours of arrival to a Level I trauma center were included. Among patients with PMCT, injury severity score (ISS) and number of injuries (NOI) were calculated either from physical exam alone (pre-PMCT) or exam and imaging (post-PMCT). ISS and NOI before and after PMCT were compared. A cause of death analysis was performed for patients who underwent comprehensive (ie, head, neck, and torso) PMCT. Non-parametric repeated measures tests were used, as appropriate.
Results
7.3% (N = 28) of patients received PMCT. Compared to pre-PMCT, median ISS (21 vs 3.5) and NOI (5 vs 2) were greater post-PMCT (P < .001, respectively). Autopsy rate was 13.2% overall; 82.5% of autopsies were due to a penetrating mechanism, and median time to autopsy reporting was 38.5 days. Among 17 patients who received comprehensive PMCT, 64.7% had a single cause of death identified, and the remaining were classified as either multiple potential contributors or unknown.
Discussion
PMCT is a readily available method to identify injuries in trauma patients who expire shortly upon presentation. Given the low autopsy rate for blunt trauma and delay in reporting, PMCT is an important adjunct for trauma providers.
Keywords
Introduction
Computerized tomography (CT) imaging is a widely available modality that provides prompt injury diagnosis. Patients who expire shortly after arrival to a trauma center often do not undergo imaging. Their calculated injury severity score (ISS) is determined solely by physical exam findings. This significantly underestimates the severity of their injury burden. Historically, autopsy reports have been a useful resource in identifying specific injuries in this patient population. However, very few cases undergo formal autopsy in current practice, and there is often a significant delay in receiving the reports from the medical examiners (ME) office.1,2 Furthermore, formal autopsies are much more likely to be performed when the cause of death is suspected to be homicide or suicide, which biases autopsy rates and injury classification towards penetrating injuries. Post-mortem CT (PMCT) imaging has been shown to accurately identify cause of death (COD) in other populations, but its utility in the trauma population is not well known. 3
Timely and accurate injury identification is a fundamental part of a successful trauma program. Identifying injuries and COD in a time-sensitive manner plays an invaluable role in performance improvement (PI) discussions, which are most productive when held within hours to days of the initial incident.4,5 CT imaging in trauma patients is integral to this process and is a critical component of modern trauma protocols. 6 A secondary role of CT is to augment the accuracy of the abbreviated injury scale (AIS) and ISS classification, which is essential in trauma system resource classification, accreditation and performance improvement.7-9 Both the American College of Surgeons (ACS) trauma center verification and state designation process rely on meeting certain trauma volume and acuity per year.7,10 PMCT offers the potential to extend this more detailed injury assessment to trauma patients that expire before traditional CT imaging is feasible.
This study evaluates the use of PMCT at a single-institution Level I trauma center. We hypothesized that PMCT would result in a higher ISS and an increased number of injury diagnoses compared to those who did not receive PMCT imaging. We also hypothesized that PMCT would result in a similar number of injury diagnoses when compared to autopsy reports, when available. Although there is literature exploring the use of PMCT in radiology and forensic science journals in diverse patient populations, to our knowledge this study is one of the first to examine the utility of PMCT in trauma patients.
Methods
Study Design and Materials
This is a retrospective observational cross-sectional study of patients who died on arrival to the trauma bay or within 24 hours of admission and received a PMCT scan. Patients who arrived between 2015 and 2020, were 16 years of age or older, and presented as either a trauma activation or were entered into the trauma registry were eligible for inclusion. There were no exclusion criteria. Study procedures were reviewed and approved by the WakeMed Health and Hospitals Institutional Review Board.
Non-contrasted PMCT scans were either chest/abdomen/pelvis, head, face, or cervical spine and were ordered at the discretion of the trauma attending of record. Demographic information including gender, patient age, and race, as well as trauma and clinical information, such as Emergency Department (ED) vital signs, comorbid conditions, mechanism of injury, level of trauma activation, and blood product administration were obtained from the institutional trauma registry and the electronic medical record (EMR). Pattern of injury was determined by the AIS. Cause of death was determined by author consensus after examination of the post-mortem imaging and results. Categories were based on existing literature defining common causes of death and injury patterns among blunt trauma death.11,12 Central nervous system (CNS) injuries included devastating brain injury and cervical spine injury; thoracic injuries included vascular, esophageal, and lung injuries; abdominal injuries included significant spleen, liver, mesenteric, and pelvic hemorrhage; and multi-trauma included multiple significant injuries without a clear underlying cause of death.
The primary outcome of interest was change in ISS and number of injuries (NOI) among patients with PMCT scans. Post-imaging ISS and NOI were obtained from the trauma registry for all patients and were calculated based on the physical exam, available imaging, and autopsy report findings. For patients who were taken for PMCT, pre-imaging ISS and NOI were calculated based on physical exam alone. Secondary outcomes included a cause of death analysis among patients with blunt injury who received at least a post-mortem head, cervical spine, and chest/abdomen/pelvis CT, as well as rate of successful identification of cause of death among patients with PMCT and autopsy. Rates of autopsy and PMCT scans, rates of referral for PMCT scans, time to autopsy reporting, and comparison of ISS and NOI between PMCT scans and autopsy were additional outcomes of interest.
Statistical Analyses
Distributions of patient demographics and clinical characteristics were examined by PMCT scan status (PMCT vs no PMCT scans). Means, medians, standard deviations, and interquartile ranges (IQR) were calculated for continuous variables, and percentages were calculated for categorical variables. Bivariate analysis of demographics and clinical characteristics were conducted using chi-squared tests for categorical data and Wilcoxon rank sum tests for continuous variables. ISS and NOI exceeded our a priori threshold for skewness; therefore, nonparametric tests were used for analysis.
To explore our primary outcome of interest, we compared pre-imaging ISS and NOI to post-imaging ISS and NOI using Wilcoxon matched-pair sign rank sign tests. Similarly, pre-autopsy (ie, post-imaging) ISS and NOI and post-autopsy ISS and NOI were compared using Wilcoxon matched-pair sign rank sign tests. Cause of death analyses were reported as frequency and proportions. Autopsy rates were calculated as a percentage of trauma deaths with completed autopsies. Median number of days and IQR were calculated for time to autopsy reporting. Statistical significance was defined as P < .05. All analyses were performed using Stata v17 (StataCorp 2021, College Station, TX).
Results
Comparison of Patients With and Without Post-Mortem Computed Tomography
Demographics and Injury Characteristics Among All Trauma Deaths.
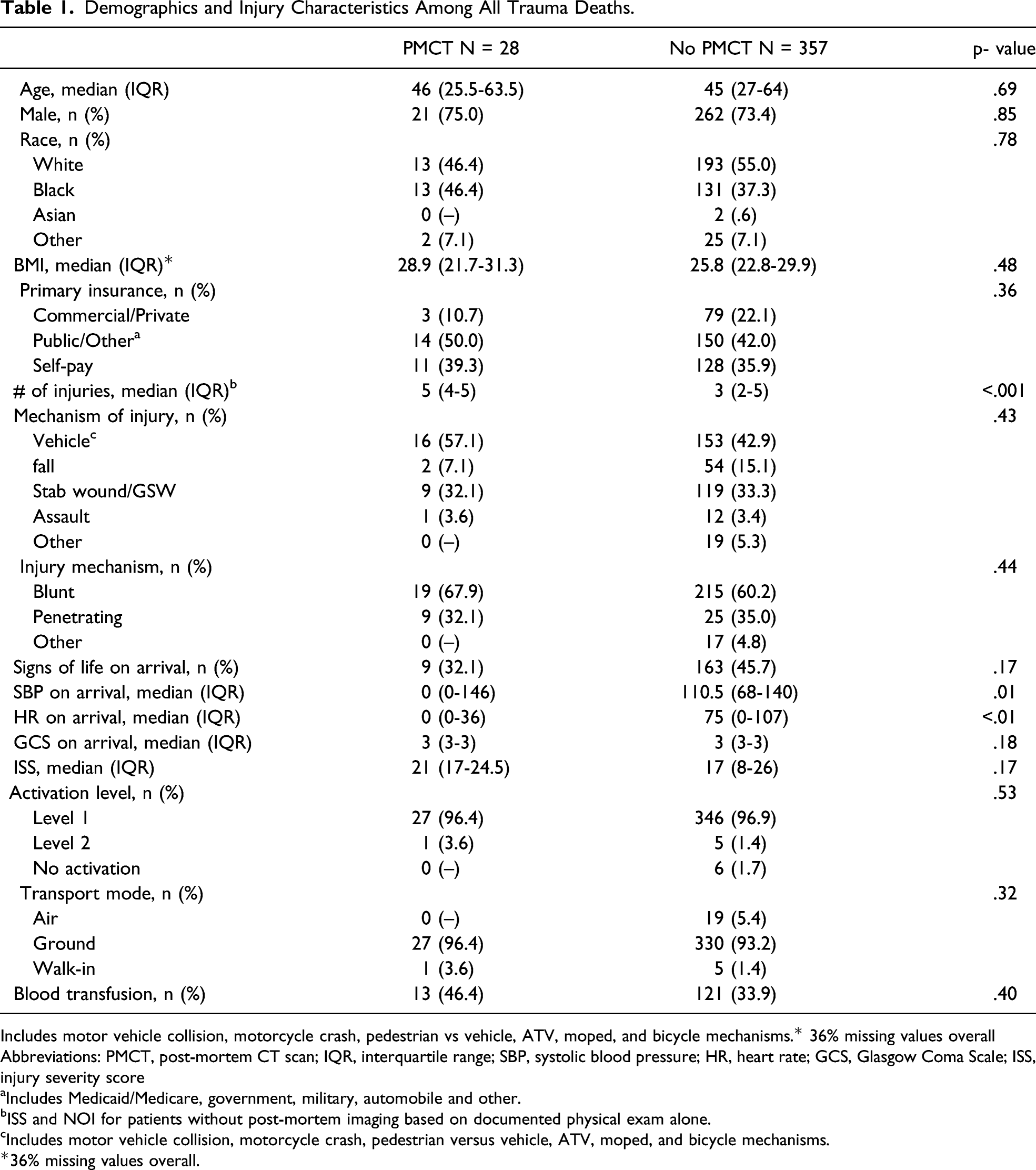
Includes motor vehicle collision, motorcycle crash, pedestrian vs vehicle, ATV, moped, and bicycle mechanisms.* 36% missing values overall
Abbreviations: PMCT, post-mortem CT scan; IQR, interquartile range; SBP, systolic blood pressure; HR, heart rate; GCS, Glasgow Coma Scale; ISS, injury severity score
aIncludes Medicaid/Medicare, government, military, automobile and other.
bISS and NOI for patients without post-mortem imaging based on documented physical exam alone.
cIncludes motor vehicle collision, motorcycle crash, pedestrian versus vehicle, ATV, moped, and bicycle mechanisms.
*36% missing values overall.
Autopsy Rates
Among all 385 patients, 51 (13.2%) underwent autopsy, and the majority of these (N = 42, 82.5%) suffered penetrating mechanisms. Only 6 (21.4%) patients underwent both PMCT and formal autopsy, of which all had penetrating mechanisms. Median time to autopsy reporting for all patients was 38.5 days (IQR: 33.3-43 days).
Injury Severity Score Calculations
Injuries Identified Before and After PMCT Among Example Patients with Blunt Injury.†
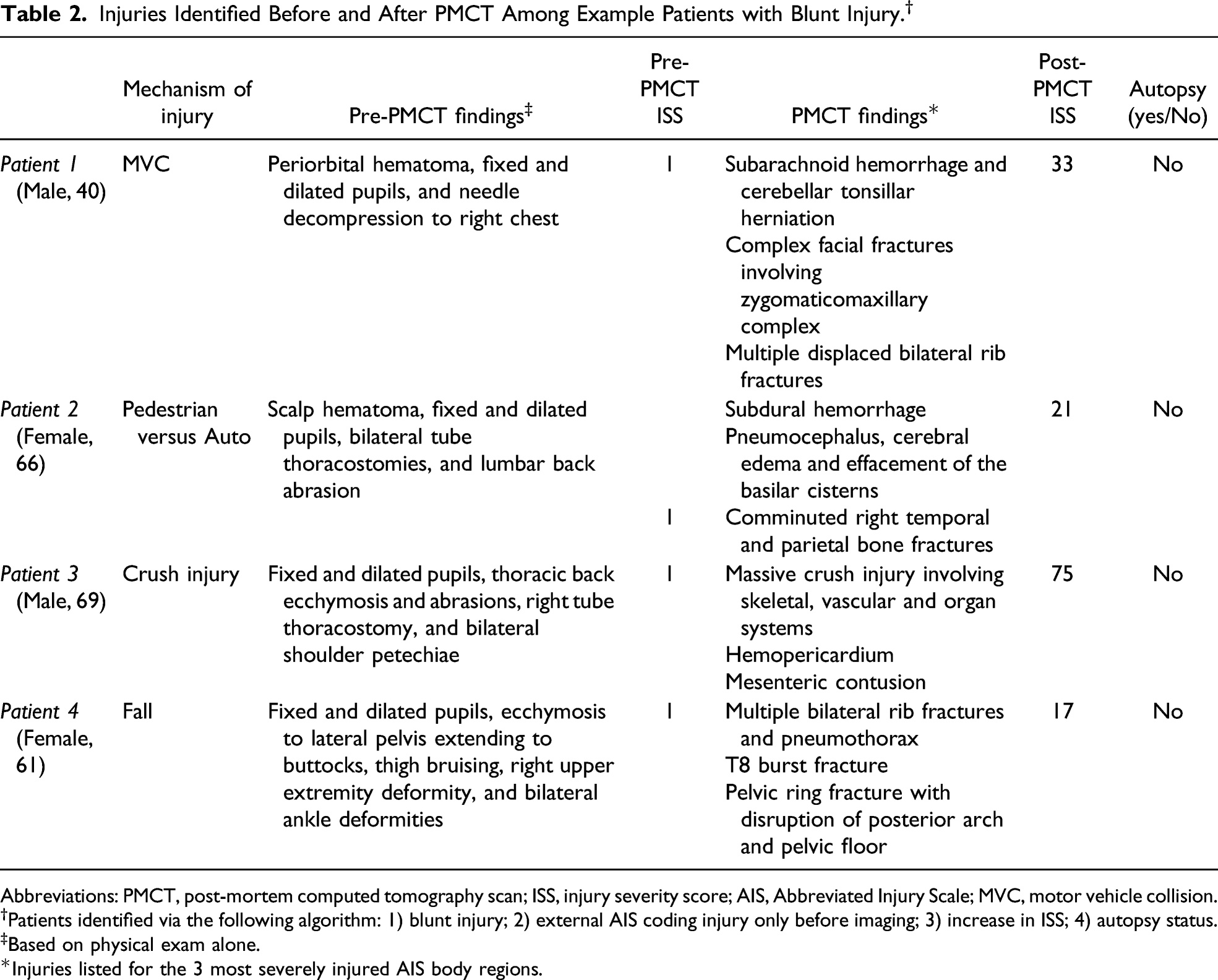
Abbreviations: PMCT, post-mortem computed tomography scan; ISS, injury severity score; AIS, Abbreviated Injury Scale; MVC, motor vehicle collision.
†Patients identified via the following algorithm: 1) blunt injury; 2) external AIS coding injury only before imaging; 3) increase in ISS; 4) autopsy status.
‡Based on physical exam alone.
*Injuries listed for the 3 most severely injured AIS body regions.
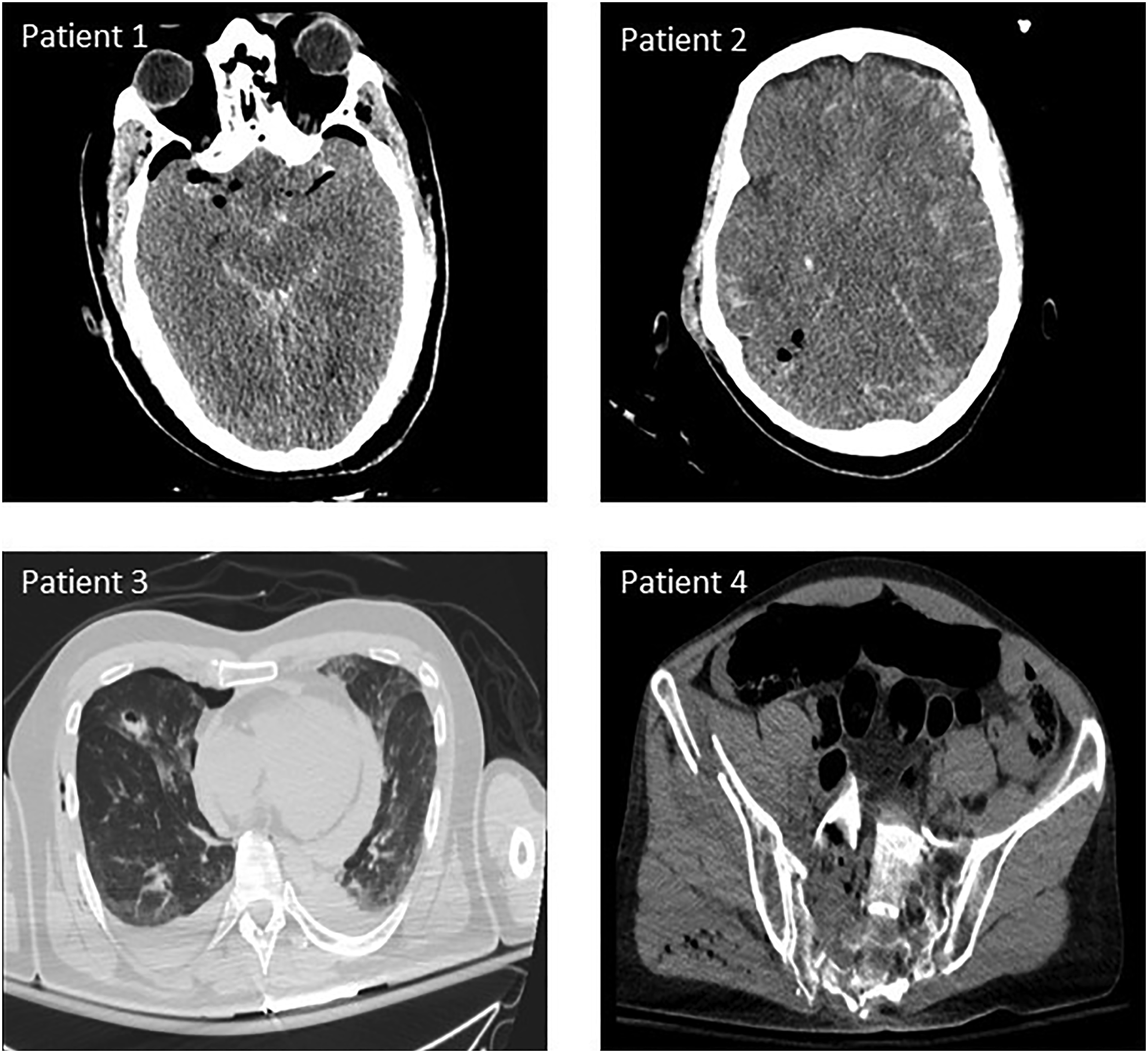
Representative PMCTs. Patient (1) extensive pneumocephalus and subarachnoid hemorrhage with cerebellar tonsillar herniation. Patient (2) extensive subarachnoid and subdural hemorrhage, pneumocephalus, cerebral edema, and effacement of the basilar cisterns. Patient (3) hemopericardium, multiple displaced bilateral rib fractures, and right pneumothorax. Patient (4) anterior protrusion of right hemi sacrum with associated small bowel injury and displaced coccyx fracture. Abbreviations: PMCT, postmortem computed tomography.
In addition, among the 6 patients who received autopsy, median ISS was greater when autopsy findings were included in calculations: 19 (IQR 16-25) pre-autopsy versus 31.5 (IQR 22-41) post-autopsy. However, this did not reach statistical significance (P = .50).
Number of Injuries Calculations
Median pre-imaging and post-imaging NOI increased from 2 (IQR 1-3) to 5 (IQR 4-5) for the 28 patients who received PMCT (P < .001). Similarly, median NOI increased among patients who underwent formal autopsy from 5 (IQR 5-5) to 6.5 (IQR 6.5-7), although this was not statistically significant (P = .09).
Cause of Death Analysis
Cause of death among PMCT patients, stratified by injury type.
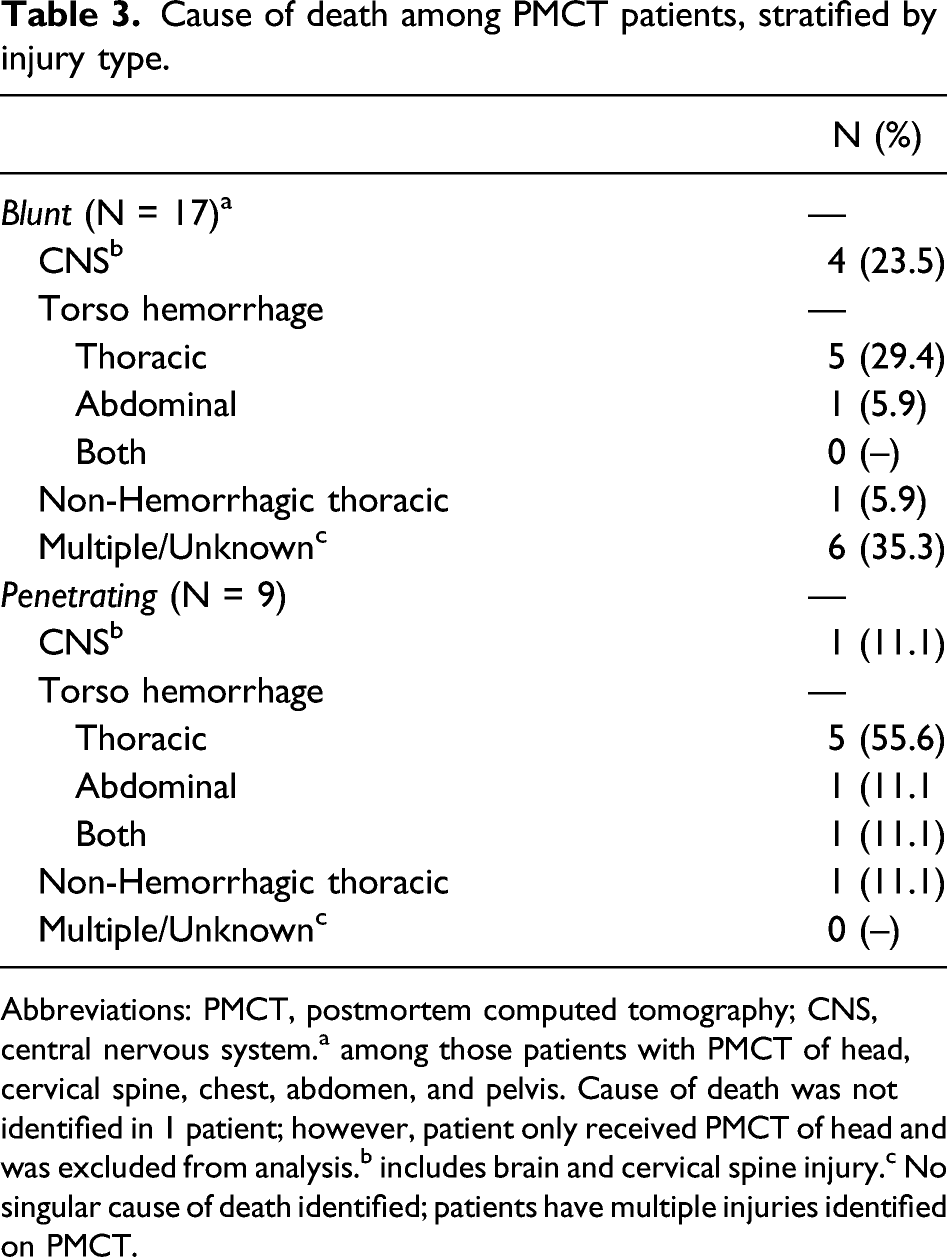
Abbreviations: PMCT, postmortem computed tomography; CNS, central nervous system.a among those patients with PMCT of head, cervical spine, chest, abdomen, and pelvis. Cause of death was not identified in 1 patient; however, patient only received PMCT of head and was excluded from analysis.b includes brain and cervical spine injury.c No singular cause of death identified; patients have multiple injuries identified on PMCT.
Discussion
PMCT is a valuable tool that allows for expeditious injury diagnosis in trauma patients who expire shortly upon arrival to the hospital. Trauma systems have traditionally relied on formal autopsy to diagnose injuries in this patient population, but additional methods are needed as autopsy rates decline. 2 Our results demonstrate that PMCT provides improved and timely injury identification that translates to more accurate ISS and NOI metrics. Our study also suggests that PMCT is comparable to autopsy in terms of injury and cause of death identification.
Accurate injury identification is essential in assessing the performance and necessity of trauma centers on the regional and national level. 13 The ACS verification process specifies that a Level I trauma center must see a minimum of 1,200 trauma patients or 240 patients with an ISS > 15 annually. 8 The current reliance on autopsies tends to bias towards more severe injuries with penetrating mechanisms. This patient population is perhaps more likely to undergo autopsy compared to patients suffering blunt mechanisms for legal reasons (ie, homicide investigations). Indeed, we found that the majority of autopsies completed in our study were secondary to a penetrating mechanism. Additionally, these results demonstrate that blunt trauma patients had a notable increase in ISS when PMCT was used as an adjunct in injury identification. This suggests that centers who have high blunt trauma volume combined with low autopsy rates may be at risk for underestimating their trauma population’s injury severity. PMCT aids in correct classification of those individuals who may have otherwise scored an ISS < 15. If the prevalence of PMCT increases, this may lead to an initial “ISS inflation” phenomenon. This could lead to adjustments in the minimum numbers required to maintain verification status but may also provide better insight into injury patterns and support research and PI initiatives that rely on an accurate trauma registry. 13
There has been a steady decline in autopsy rates in recent years, which has negative implications for PI initiatives and training efforts within individual trauma centers.2,14 Further, there may be significant delays in autopsy reporting of weeks to months, which renders the results much less useful from a training perspective. The quick turnaround time of PMCT in comparison to autopsy allows for prompt feedback in the setting of meaningful PI and educational discussions. Such discussions play a critical role in improving patient care, and previous studies have shown that these PI efforts are most beneficial when done soon after the trauma death.14–15 Finally, PMCT can provide a very useful alternative in settings where particular cultures or religions may prohibit invasive autopsy examinations. 16
Studies have described superior features of PMCT compared to autopsy for some injuries, such as skeletal trauma and gas detection in air emboli and pneumomediastinum.17–18 We were not able to draw any conclusions from our study regarding superiority in diagnosing specific injury patterns when comparing the 2 modalities, but we did find that PMCT and autopsy may offer complementary and synergistic results.19,20 For example, PMCT revealed a grade V blunt cerebral vascular injury that was not noted on autopsy report in 1 patient. In another patient, conversely, autopsy revealed an esophageal and aortic perforation that PMCT identified as a left hemothorax with rightward mediastinal shift. The improved accuracy of autopsy in detecting aortic injury is supported by the literature. 18
There are several limitations to this study. First, some analyses may be underpowered due to the inclusion of only 28 patients undergoing PMCT during the study period. PMCT use increased substantially from 3 patients in 2015-2017 to 25 patients in 2018-2020, which was subsequent to a more efficient ordering process. A follow-up analysis with more recent data that reflects this trend may help to increase sample size. Second, our secondary outcomes comparing PMCT to autopsy only included 6 patients, and all 6 of these patients sustained penetrating mechanisms of injury, which is a potential source of sampling bias. Another limitation of PMCT is the inability to precisely classify the severity of particular injury patterns. This is in part due to the inability to administer intravascular (IV) contrast, which is especially relevant for vascular and solid organ injuries that are graded by severity. However, formal autopsies are also not able to provide grading for solid organ injuries. Additionally, given that AIS coding is a semi-subjective process, there may be some coding differences between raters; however, this potential measurement bias is likely small and not clinically significant.
An important aspect of PMCT use at our institution is ensuring that patients and families do not get charged for these studies, which was made possible through collaborations with hospital administration and the radiology department. We recommend that other institutions interested in implementing routine PMCT consider similar collaborations, as well as consideration of institution-specific costs. Medicolegal concerns regarding procedural consent, automated release of imaging results, missed injuries, and mispositioned devices may also be potential barriers to a successful PMCT program. However, state laws typically protect medical PI discussions from legal discoverability, and framing the use of PMCT within PI initiatives has proved vital to our institution’s successful implementation of this technology. This is in contrast to death certificates, and in some states autopsy reports, which are part of the public record and are less amenable to medicolegal protections. Future directions will include a prospective quality improvement project that evaluates cost comparisons of PMCT and formal autopsy.
In conclusion, this study demonstrates that PMCT is a reliable method to identify injuries and cause of death in a timely fashion. Low autopsy rates and delayed reporting, especially among blunt trauma patients, underscore the role of PMCT as an important adjunct to formal autopsy. Implementing routine PMCT may allow for more productive PI initiatives and may have a role in trauma center verification.
Footnotes
Acknowledgments
We would like to express thanks to the WakeMed Health and Hospitals trauma research team, clinical nurse specialists, and trauma registrars for their support and assistance with data collection. In addition, we would like to thank WakeMed Radiology who are instrumental in reporting expedited CT results.
Author Contributions
LP and JPT contributed equally to the study design, literature search, data analysis, data interpretation, writing, and critical revision, and final review.
JN, SMM, EJR, POU contributed to study design, data analysis, critical revision, and final review.
AB contributed to literature review, data collection, data interpretation, and final review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.