
Abstract
We hypothesize that obesity is a common diagnosis in those with achalasia at our institution but time to diagnosis and treatment is longer compared to normal weight counterparts due to implicit bias. We retrospectively reviewed all adult patients between 1/1/2013 and 6/31/2020 with a diagnosis of achalasia. Demographics, comorbidities, Eckardt scores, interventions, complications, time to consult, duration of symptoms, and follow-up were evaluated. More than half of the patients were seen in the most recent 2 years following POEM introduction and 138 had available BMI data. 46 were obese (33%) and 92 were non-obese (67%). Obese patients reported a shorter duration of symptoms prior to seeking treatment 12 versus 24 months. There was no difference in time to intervention or procedure offered. There was a non-significant trend toward higher leak (11 vs 5%) and overall complication rate (19 vs 17%) in obese patients. In follow-up 98 patients had BMI data. There was a a significant difference in mean BMI change -1.2 +/- 4.2 kg/m2 in obese patients and +0.1 +/- 2.1 kg/m2 in normal weight patients. One year follow-up was available in 16 (47%) obese and 25 (33%) non-obese patients and showed a non-significant trend toward greater weight gain in the normal/overweight group (+3.2 +/- 1.1 kg/m2) compared to obese (+2.0 +/- 3.5 kg/m2). Obese patients with achalasia have unique considerations. Duration of symptoms may be shorter in the obese patient with esophageal dysphagia. We noted trends toward greater weight gain following interventions in non-obese patients with equivalent complication rates
Introduction
Though the precise etiology remains unknown, achalasia affects approximately 20,000 to 40,000 patients a year in the United States. 1 Inhibitory neurons that coordinate esophageal body peristalsis and lower esophageal sphincter relaxation are selectively destroyed, leading to the classic presenting symptoms of progressive dysphagia, regurgitation, chest pain, and weight loss. Autoimmune disorders and infectious agents such as herpes simplex virus 1 and varicella zoster virus have been inconclusively implicated, and no racial or gender predilection is evident. Much of our historic and current data for management comes from populations where obesity is far less common. Even in large series there is a scarcity of data regarding patient’s starting BMI. 2 Clinically patients with achalasia who are also overweight or obese may constitute a specific subtype of disease presenting with differing underlying pathophysiology, and outcomes after operative intervention may differ when compared to non-obese patients. There are various effective interventions for achalasia including pneumatic dilation, botulinum toxin injection, Per Oral Endoscopic Myotomy (POEM) and surgical Heller myotomy with partial fundoplication. 3 With newer techniques such as POEM post procedural gastroesophageal reflux disease can be seen at higher rates in some series. 4 We seek to investigate differences in disease presentation, progress, and treatment outcomes in patients referred to our academic hospital for achalasia and categorized as obese versus non-obese.
Materials and Methods
Following expedited IRB approval, we retrospectively reviewed all adult patients evaluated in our health system between 1/1/2013 and 6/31/2020 with a diagnosis of achalasia by ICD codes. We reviewed patient demographics, comorbidities, Eckardt scores, interventions, complications, time to consult, duration of symptoms, and follow-ups. We then compared our findings between patients with obesity (BMI 30 kg/m2) and without (<30 kg/m2). Standard univariate statistics were used to identify statistical differences in primary and secondary outcomes based on weight. Standard linear and logistic regression methods were used to adjust for differences in baseline patient characteristics and type of intervention on outcomes. Data is presented as mean (SD) when parametric, median (IQR) when non-parametric, or frequency (%). A P-value of <.05 was considered statistically significant.
Results
We identified 205 patients, with 140 (70%) seen by our thoracic surgery service. More than half of the patients were seen in the most recent 2 years following POEM introduction and 138 had available BMI data. (Figure 1) Patient BMI’s were categorized obese ≥30 kg/m2 in 46 (33%), overweight 25-29.9 kg/m2 in 39 (28%), normal 18.5-24.9 in 53 (38%), and 1 underweight BMI <18.5 (1%). Obese patients were more likely to be female 69 versus 40% (P < .01), have diabetes mellitus 22 versus 9% (P = .06), and obstructive sleep apnea 24 versus 2% (P < .01). They also reported a shorter duration of symptoms prior to seeking treatment 12 versus 24 months (P = .03). There was no difference in initial Eckardt scores (6.7 Patient Characteristics. Patient results (n=139).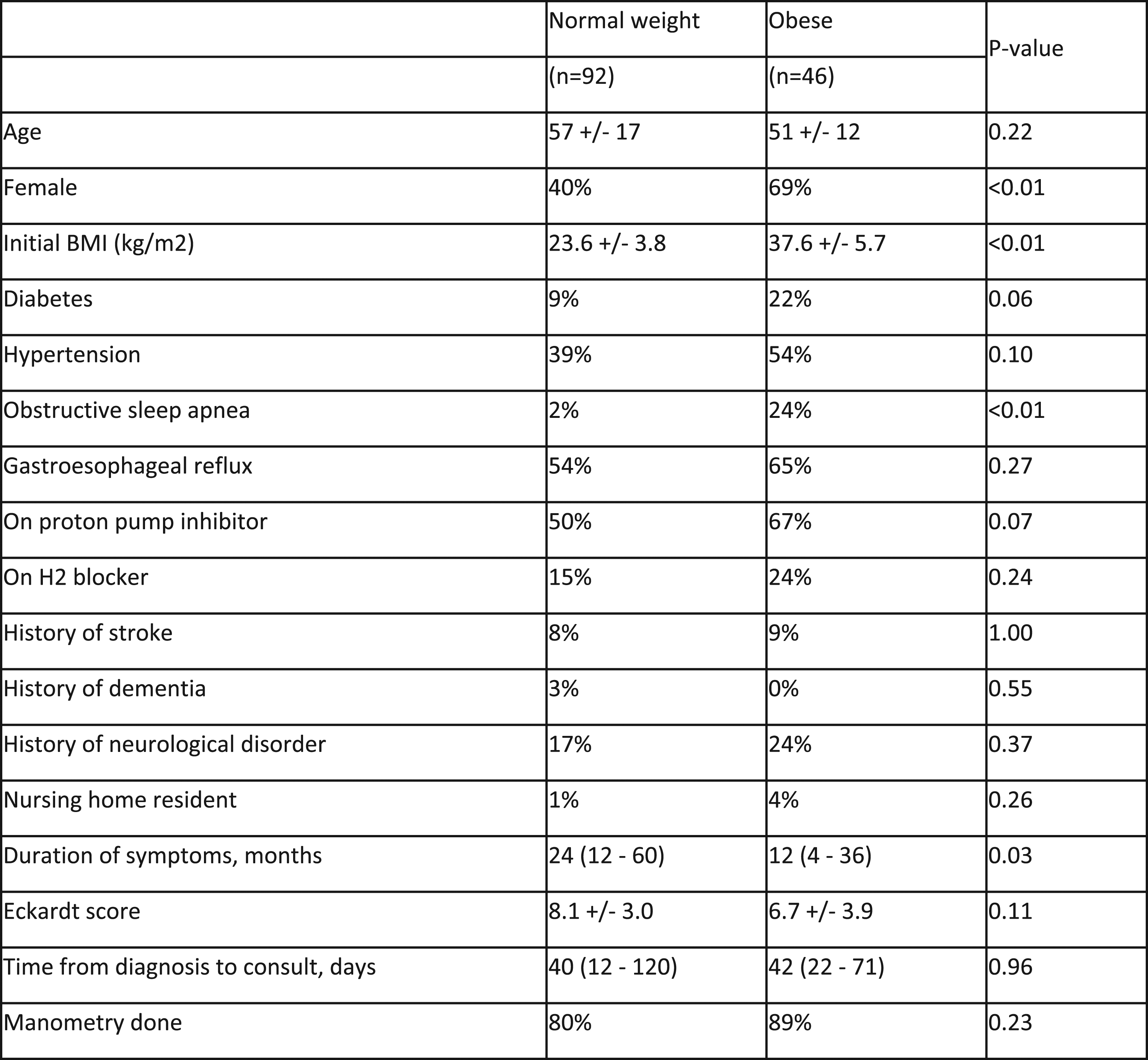
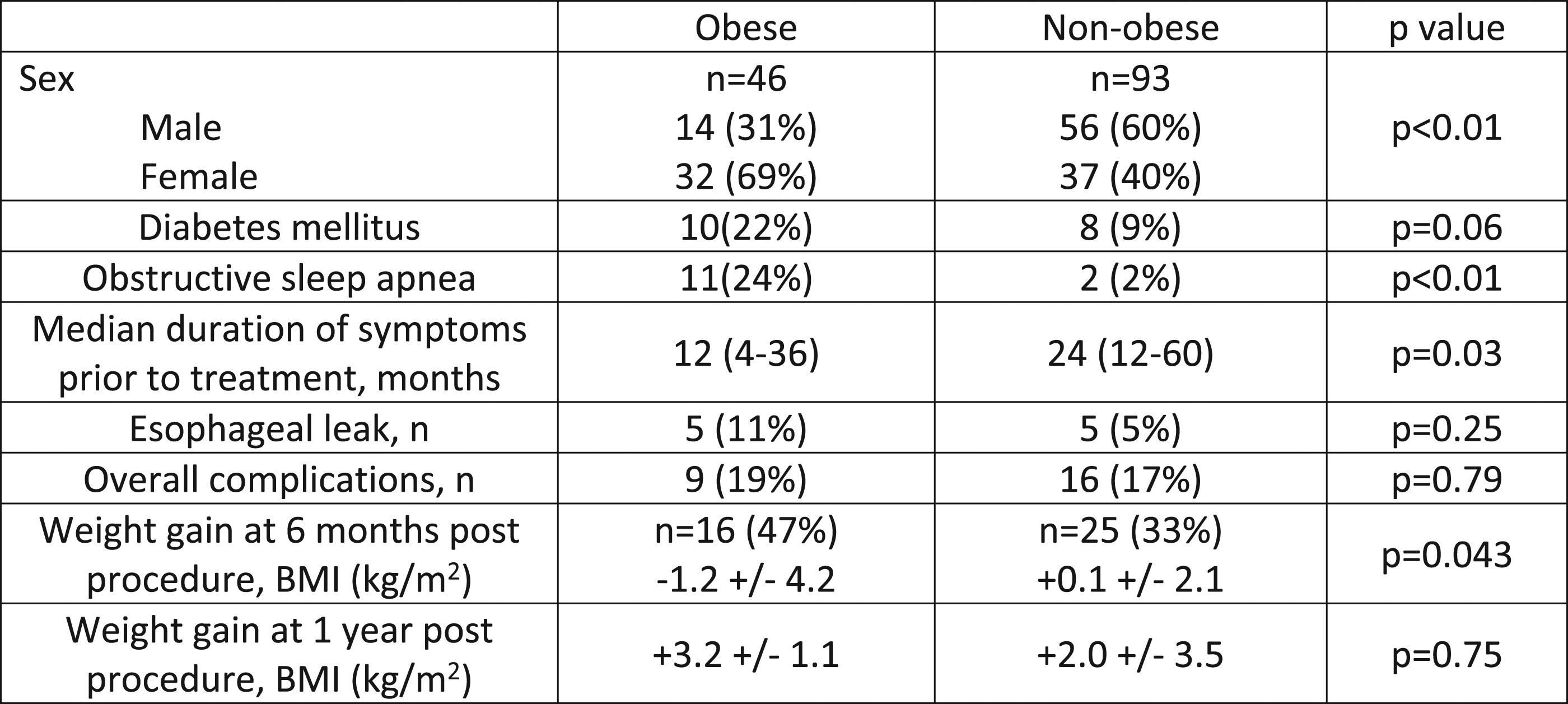
In follow-up 98 (78%) patients had BMI data. There was a statistically significant difference in mean BMI change −1.2 +/− 4.2 kg/m2 in obese patients and +.1 +/− 2.1 kg/m2 in normal weight patients (P = .043) at 6 months. This corresponds to an average weight change of −2.2 +/− 10.1 kg in obese patients compared to −.9 +/− 4.1 kg in non-obese patients (P = .48). One year follow-up was available in 16 (47%) obese and 25 (33%) non-obese patients and showed a non-significant (P = .22) trend toward greater weight gain in the non-obese group (+8.3 +/− 13.1 kg) compared to obese (+1.0 +/− 20.1 kg).
Discussion
A disease defined by weight loss and food aversion is unsurprisingly underreported and poorly understood in our increasingly overweight populace. 2 To reinforce the notion, much of our current data, particularly around POEM comes from Asian populations where obesity is far less common. 5 We hypothesized that obesity is a common diagnosis in those with achalasia, but time to diagnosis and treatment is longer compared to normal weight counterparts due to implicit bias and current training paradigms. We also hypothesized that complications would be higher and post-intervention weight gain greater in obese patients.
The first assumption was partly true in our patient cohort. Nearly two-thirds of patients identified were overweight or obese and only one was clinically underweight. This lies in stark contrast to traditional teaching on the disease. There is a growing acknowledgment of this trend. Recent investigations have demonstrated obesity as an independent risk factor for esophageal motility disorders. Nevertheless, reports of detailed evaluation of esophageal function in morbidly obese patients are rare. 6 Motility disorders associated with obesity include hypertensive lower esophageal sphincter (LES), nutcracker esophagus, diffuse esophageal spasm, ineffective esophageal motility, and nonspecific motility disorders. 7 New to our study was the finding that patients categorized as obese were identified and treated earlier in their symptomatic experience than normal weight counterparts.
Our second assumption also revealed interesting counterpoints. Though underpowered, our 6- and 12-month follow-up found patients categorized as obese more likely to lose weight after treatment and those starting at normal weight more likely to gain in the postoperative period. This was confirmed in our data by using BMI rather than overall weight to standardize the change in body composition. Further study of larger groups would be needed to confirm the finding and parse the underlying pathophysiology that might explain this outcome. There was a trend toward higher leak rate in obese patients. This likely is owed to POEM being offered more commonly to high-risk patients and this series incorporates our early learning curve with the procedure. However, obesity as a risk factor for surgical complications would certainly be justified by the literature. 8
With overlapping symptomology in respect to achalasia and comorbidities associated with obesity such as GERD, we found our institution was able to diagnose and intervene in our obese demographic without obvious bias. Limitations of this study include the retrospective nature of our data set, which assumes some selection bias and missing data points. We also limited our data set to include patients associated with our thoracic surgery department to minimize variability in diagnoses and work up.
The obese patient with achalasia should be recognized as a patient group with unique physiologic needs that present commonly and with similar symptoms to normal weight counterparts. Duration of symptoms may be shorter in the obese patient with esophageal dysphagia prior to physician evaluation. In our center we noted trends toward greater weight gain following interventions in non-obese patients with equivalent complication rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.