
Abstract
Introduction
This study aims to improve public health outreach in a high-risk population.
Methods
This is a single center study of Trauma Registry data, inclusive years January 1, 2016 to March 30, 2021. The study population was stratified into two groups: ETOH ≥ 80 mg/dL and ETOH <80 mg/dL. A total of 1141 were included.
Results
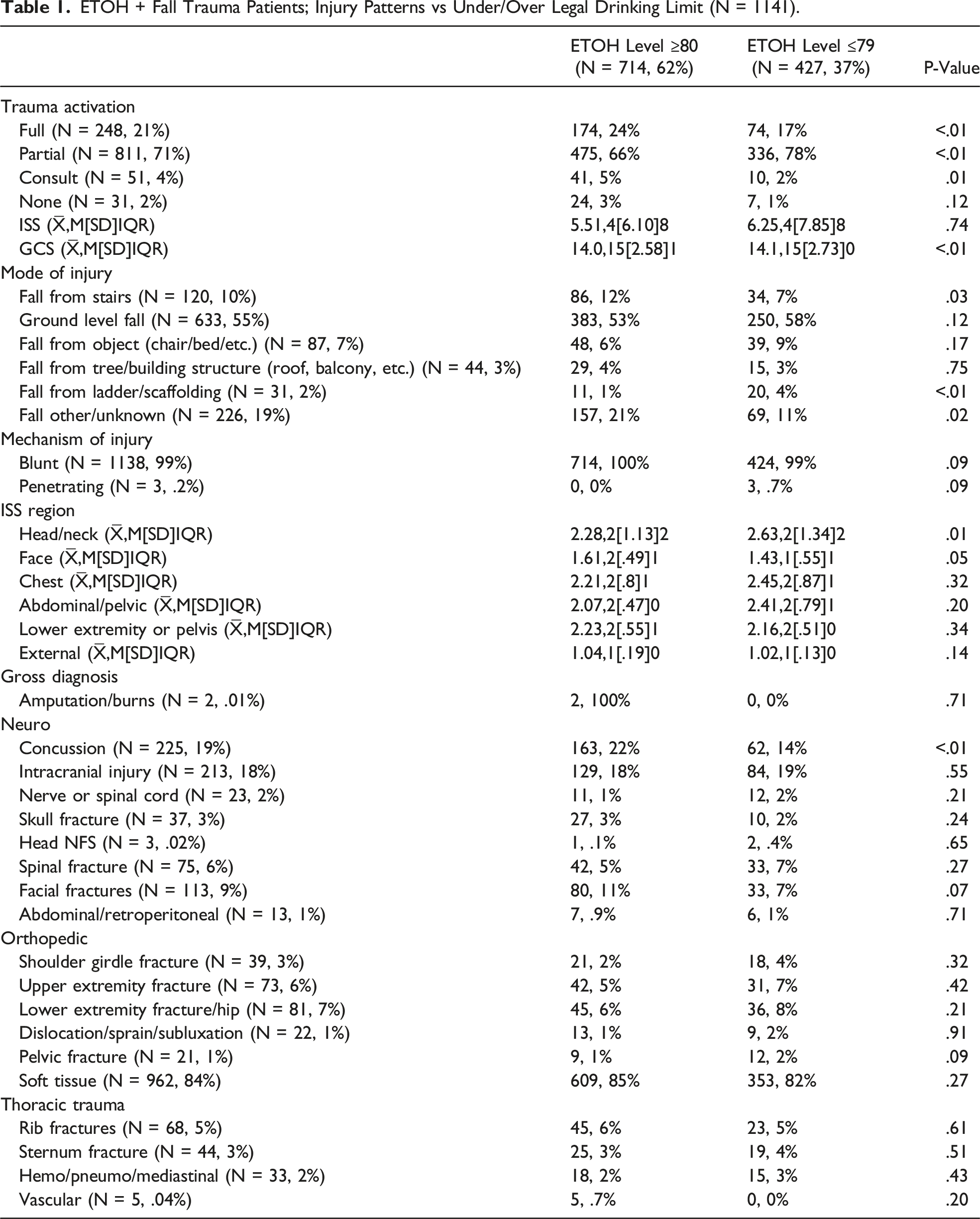
Those above the legal drinking limit had a significantly higher mean ETOH (231 mg/dL; P <.01) and were typically younger men that arrived by ground ambulance. The significant injury patterns of those above the legal limit included full activation and consults who fell from stairs and fell from other or unknown. A higher proportion of intoxicated fall trauma patients above the legal limit were diagnosed with a concussion.
Conclusions
Excess alcohol consumption, particularly during a pandemic year, may lead to a higher incidence of fall from stairs trauma in men who are more likely to be diagnosed with a concussion.
Keywords
Traumatic falls, even though preventable, are a major problem surrounding traumatic injuries. Adults are at a higher risk of experiencing traumatic injuries due to falls. Adult traumatic falls commonly include unintentional (90.2%), workplace accidents (8.1%), and attempted suicide (1.7%). 1 Grouping patients into distinct categories due to the type of fall is relevant in trauma centers. Two distinct categories for fall causation can include comparing intoxicated vs sober patients. Sober and intoxicated patients experience different types of injuries based on their states. For example, sober patients are more likely to sustain lower extremity injuries, 2 while intoxicated patients sustain more head and spinal injuries. 2 Intoxication not only implies being under the influence of alcohol but also prescription medication and illegal drugs. Intoxicated patients with fall-related injuries due to drugs commonly have a history of, or currently use, opioid prescriptions. 2 Prescriptions such as hydromorphone, oxycodone, morphine, and fentanyl are commonly tied with fall patients, leading to various outcomes, such as injury or even, in some cases, death. 2 The sober or intoxicated mindset may vary, leading to the causation of unique fall patterns. For example, sober patients are more aware and alert, leading to the ability to consider the chances of falling when put in certain situations, contributing to falling injuries. 3 The higher the level of intoxication also leads to the higher chances of falls. 4 Intoxicated patients who binge drink alcoholic beverages are associated with an increased risk of traumatic fall injuries than patients who do not binge. 4 A common fall seen with middle-aged intoxicated patients is unintentional falls off of balconies, leading to injuries and, in certain cases, death. 4 Patients who have sustained injuries due to traumatic falls, whether while sober or intoxicated, have a significantly higher chance of a repeated fall. 3 Further investigation of sober vs intoxicated fall injury patterns is critical for improved public health outreach, education, and prevention.
A retrospective cohort study on trauma registry data of fall patients (>/ = 18 years) admitted to an ACS verified level one trauma center in South Carolina, inclusive of January 1, 2016 to March 30, 2021. The study population was stratified into two groups, over the legal drinking limit (EtOH ≥ 80 mg/dL) and under the legal drinking limit (EtOH < 80 mg/dL). Based on patient demographics, injury patterns, morbidity, and mortality, comparisons were made. Continuous variables were compared using the Wilcoxon test, whereas categorical variables were compared using Pearson’s chi-square test of proportions, as appropriate in R software.
ETOH + Fall Trauma Patients; Injury Patterns vs Under/Over Legal Drinking Limit (N = 1141).
Consuming alcohol in the preceding six hours, when compared with no alcohol, has almost an eight-fold increase in the risk of injury, with a higher risk associated with four or more drinks compared with one to three drinks, which suggests a dose-response effect. For the elderly population, it is also essential to take into account the potential confounding effects of central nervous system-altering medications along with alcohol intoxication. Exposure to these medications is associated with a significantly increased risk of falling and related injuries at four years. This is likely due to increased sedation.
Injury patterns seen under the influence of alcohol differ from those unrelated to alcohol. Those intoxicated have more tendency to fall from stairs or ladders, suffer blunt injuries to the head, neck, or face, or pelvic fractures. In addition, more injuries to the back of the head occur under the influence of alcohol. The findings of this study show an 18% association between falls with alcohol over the legal limit and intracranial injuries. Although not a statistically significant association, it is an essential complication of alcohol-related falls as intracranial injuries present very high morbidity and mortality for the patient and long-term sequelae of the injury. A greater incidence of alcohol-related traumatic falls are observed in the summer than in other seasons; although this distinction was not statistically significant, however, it is expected due to the heavy traffic seen in a beach destination within South Carolina during the summer. In this trauma center, there were fewer traumatic falls seen during the years associated with the COVID-19 pandemic compared to other years. However, most of these had a blood-alcohol level above the legal limit. These findings can be explained by the travel bans and the higher incidence of alcohol use during the pandemic. We present limited data for 2021, and these trends may very well change as more tourists return in the next coming years.
The present study estimates that 62% of fall trauma patients that presented to an ACS verified trauma center were over the legal drinking limit and were typically younger men brought in by ambulance. These patients with alcohol levels above the drinking limit had a higher probability of being full trauma activations or consult with lower GCS and diagnosed with a concussion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There are no conflicts of interest to declare. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.