
Abstract
Objective
Closed-incision negative pressure therapy (CINPT) with the Prevena system has been used and clinically evaluated in high-risk groin incisions to reduce the risk of postoperative complications. We performed a cost-effectiveness analysis evaluating CINPT in femoral-popliteal bypass with prosthetic graft.
Methods
A literature review looking at prospective randomized trials determined the probabilities and outcomes for femoral-popliteal bypass with and without CINPT. Reported utility scores were used to estimate the quality adjusted life years (QALYs) associated with a successful procedure and postoperative complications. Medicare current procedure terminology and diagnosis-related group codes were used to assess the costs for a successful surgery and associated complications. A decision analysis tree was constructed with rollback analysis to highlight the more cost-effective strategy. An incremental cost-effectiveness ratio (ICER) analysis was performed with a willingness to pay at $50,000. Deterministic and probabilistic sensitivity analyses were performed to validate the robustness of the results, and to accommodate for the uncertainty in the literature.
Results
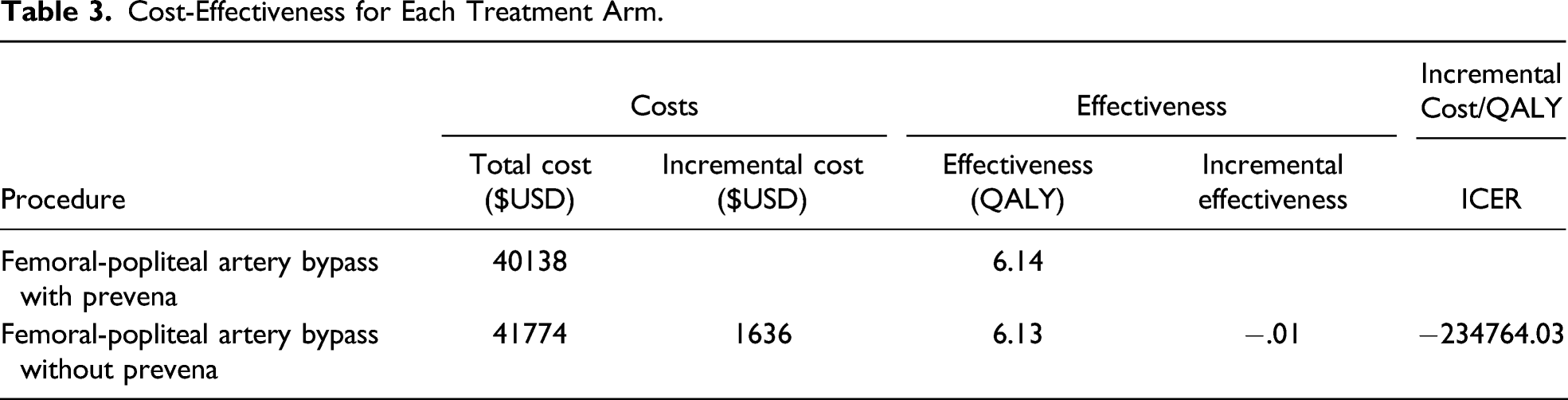
Femoral-popliteal bypass with CINPT is less costly ($40,138 vs $41,774) and more effective (6.14 vs 6.13) compared to without CINPT. This resulted in a negative ICER of −234,764.03, which favored CINPT, indicating a dominant strategy. In one-way sensitivity analysis, surgery without CINPT was more cost-effective if the probability of successful surgery falls below 84.9% or if the cost of CINPT exceeds $3139. Monte Carlo analysis showed a confidence of 99.07% that CINPT is more cost-effective.
Conclusions
Despite the added device cost of CINPT, it is cost-effective in vascular surgical operations using groin incisions.
Keywords
Introduction
While advances have been made in surgical infection control practices, a prevalence survey from the Centers for Disease Control and Prevention estimated 110,800 surgical site infections (SSIs) associated with inpatient surgeries in 2015. 1 Furthermore, SSI is currently the most costly healthcare-associated infection with an average increased cost of $20,842 per admission and extended length of stay of 9.7 days. 2 The incidence of SSIs following peripheral vascular surgery procedures at the groin varies from 2.8% to 44% in the literature.3-6
Previous studies have demonstrated that negative pressure wound therapy (NPWT) has reduced the incidence of SSI in various high-risk surgical wounds.7-11 Groin incisions, in particular, have a higher risk for postoperative complications, including wound infection, wound dehiscence, seroma, hematoma, skin necrosis, and lymph leaks. This increased risk in postoperative complications for groin incisions is secondary to anatomical proximity to the perineum and urogenital structures, relatively superficial graft position, and manipulation of lymphatics. 12 Increasing evidence for the benefits of CINPT in the field of vascular surgery, in particular, has emerged through recent meta-analyses and consensus recommendations.13-17
The PrevenaTM system (KCI Medical, San Antonio, TX) is a CINPT device which can be applied to closed incisions with continuous 125mmHg of negative pressure for up to seven days. This microdeformational system applies a highly porous material under suction to the wound surface, creating an environment for increased granulation tissue formation and decreased lateral tension. 18 Furthermore, the centripetal pulling of wound margins (termed “macrodeformation”) reduces edema by increasing the pressure gradient between the interstitial space to the surface porous material. 19 Kairinos et al further demonstrated that this negative pressure stimulates cell proliferation and angiogenesis via the HIF-1α/VEGF pathway. 20
The aim of our study was to perform a cost-effectiveness analysis evaluating closed-incision negative pressure therapy (CINPT) use in femoral-popliteal bypass with prosthetic graft. While previous studies have evaluated health-care costs associated with CINPT in vascular surgery, 21 scarce cost-effectiveness analyses have been conducted on CINPT in vascular surgery groin incisions. 22 We performed a cost-effectiveness analysis evaluating CINPT use in femoral-popliteal bypass with prosthetic graft.
Methods
Reference Case
In this cost-utility model, a hypothetical cohort of vascular patients with lower extremity claudication and tissue loss were included. The base case was defined as a 65-year-old male patient with lower extremity claudication and tissue loss. This age demographic was felt to be reasonable in this vascular surgery population. Furthermore, both claudication and tissue loss were chosen as not only does this appropriately reflect the vascular surgical patient population, but also tissue loss is a known risk factor for surgical site complications.
In this hypothetical scenario, the patient could undergo femoral-popliteal bypass with prosthetic graft with or without Prevena closed-incision negative pressure therapy. Life expectancy of patients in this cohort from time of surgery is estimated to be 8.7 years. 23
Decision Model and Probabilities
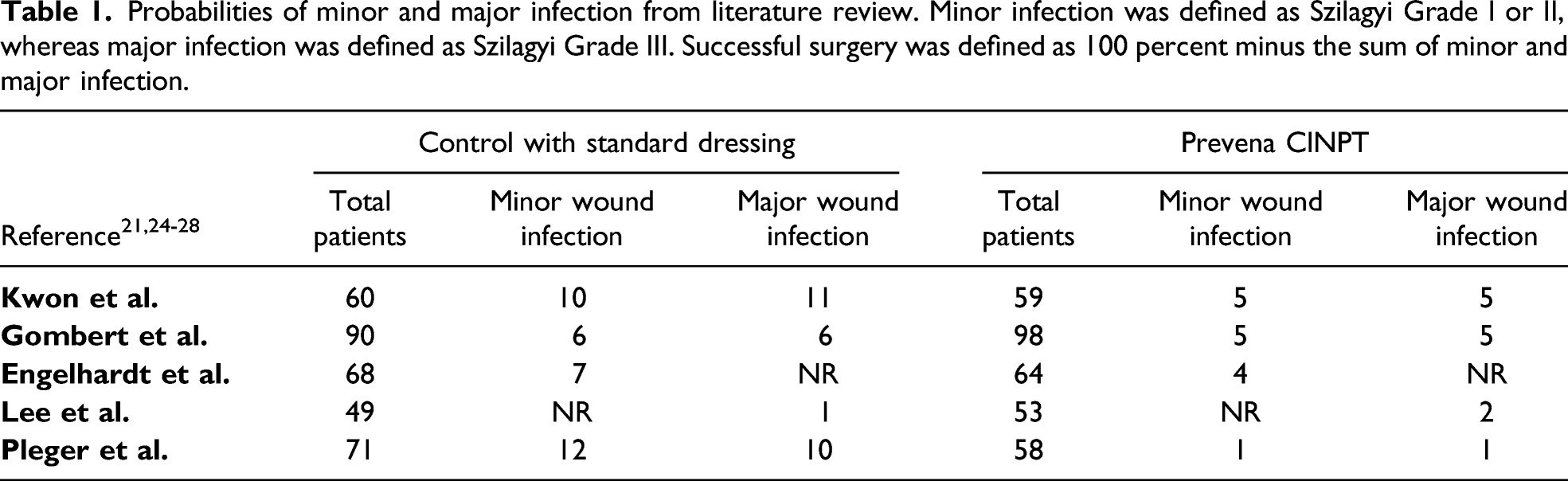
We used TreeAge Software Pro Version 2020 (Treeage Software, Inc., Williamstown, MA) to construct the decision model and compare both treatment modalities (Figure 1). In this model, under each arm of the decision tree, the probability of health states was incorporated as well as the associated costs and their utilities. In this model, both treatment modalities (femoral-popliteal artery bypass with prosthetic graft with vs without Prevena closed-incision negative pressure therapy) have the same types of postoperative complications: minor wound infection, major wound infection, successful sartorius flap reconstruction, excision of graft and axillary-femoral bypass, amputation, and death with different probabilities. These event pathways, complications, and probabilities were obtained by performing a comprehensive review of vascular surgery patients undergoing lower extremity bypass with and without Prevena closed-incision negative pressure therapy using “lower extremity bypass,” and “negative pressure therapy” as search terms.21,24-28 The literature review had two independent reviewers (JB, TT) and any disagreement in data collection metrics was resolved by the senior author’s (AC) arbitration. Probabilities of complications and outcomes from these studies were pooled and weighted to provide a complication rate for each. These data provided the probability of successful surgery, minor infection, and major infection (Table 1).21,24-28 The end states of sartorius flap reconstruction, excision of graft and axillary-femoral bypass, amputation, and death were obtained from our groups’ previously published work.
29
Decision tree. The bottom green line represents the cost-effective strategy. Probabilities of minor and major infection from literature review. Minor infection was defined as Szilagyi Grade I or II, whereas major infection was defined as Szilagyi Grade III. Successful surgery was defined as 100 percent minus the sum of minor and major infection.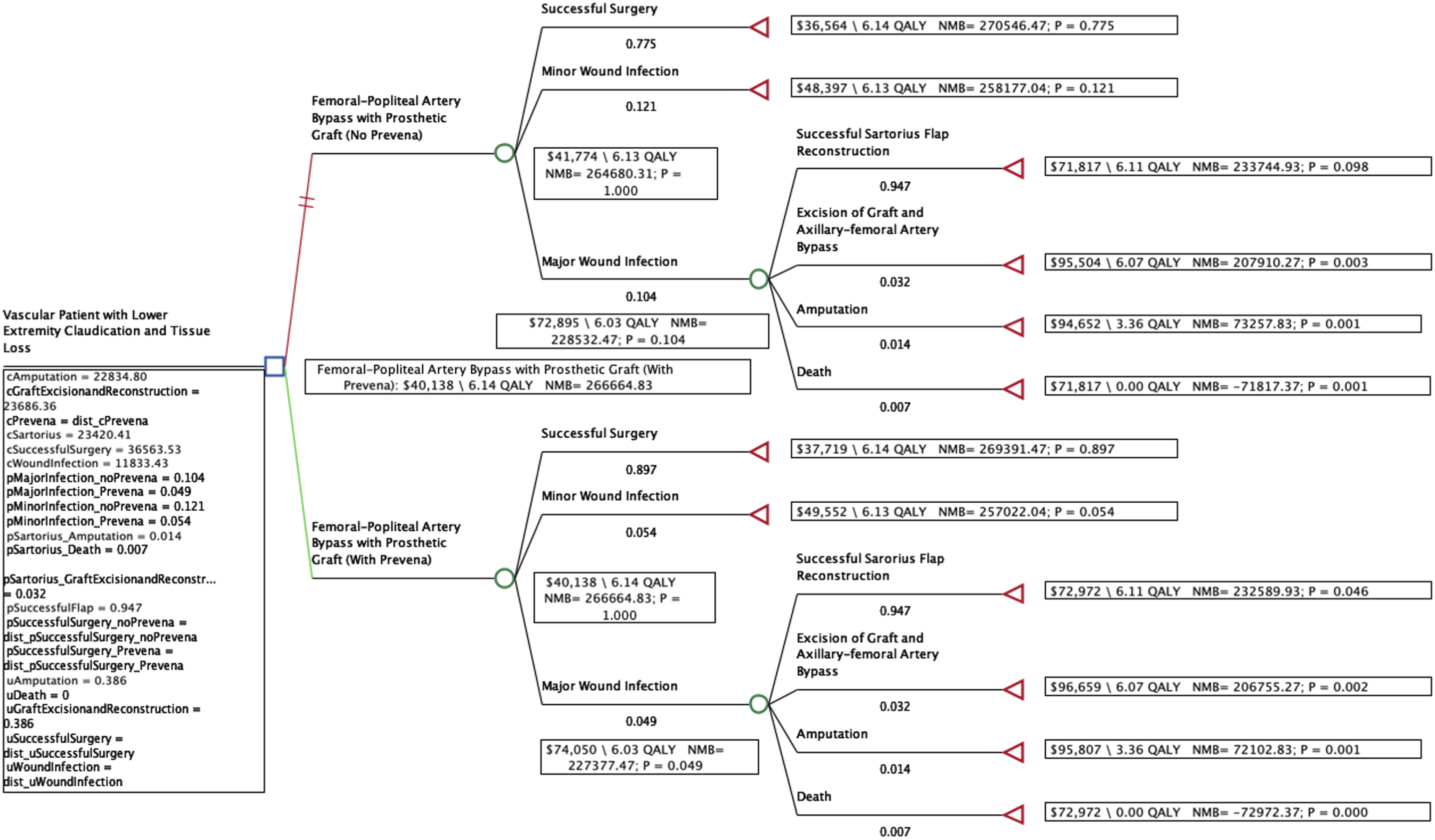
Costs and Perspective
Utilities, Costs, and Quality-Adjusted Life-Years (QALY).
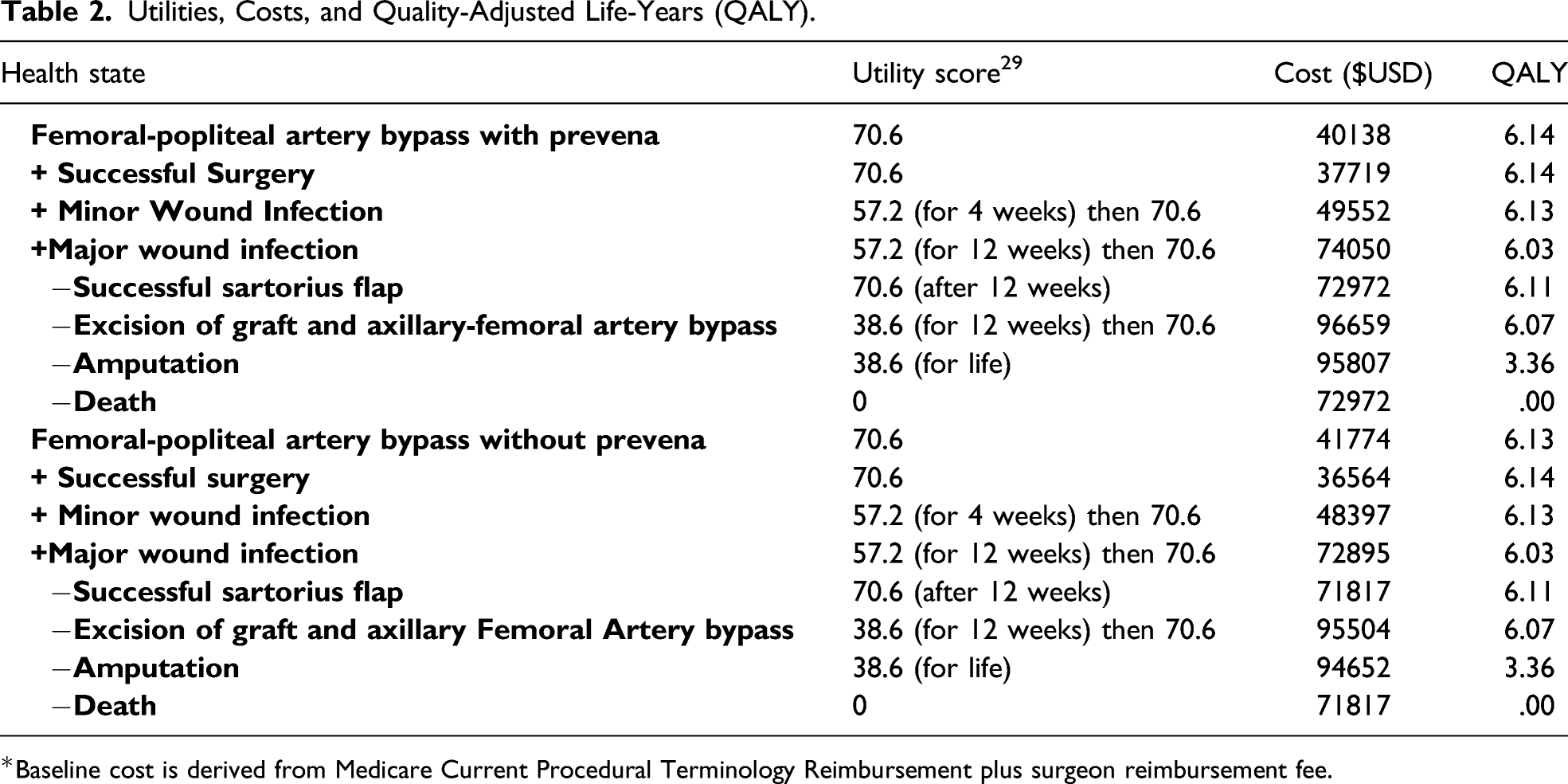
*Baseline cost is derived from Medicare Current Procedural Terminology Reimbursement plus surgeon reimbursement fee.
Of note, this model did not include any indirect costs such as those for loss of productivity, waiting time, transportation, and absence from work. The perspective of the third-party payer was adopted in order to provide well-balanced cost burden to each treatment modality, which is a well-accepted and established perspective in the literature.30,31
Utilities
Utility scores of all health states of femoral-popliteal artery bypass with prosthetic graft with and without Prevena closed-incision negative pressure therapy were obtained from previously published utility scores that represented health states ranging from 0 (death) to 1 (healthy). 29 These utility scores (Table 2) were converted to quality-adjusted life years (QALYs) to measure the effectiveness of our model. Patients with minor wound infections were estimated to recover within 4 weeks and return to baseline, while patients with major wound infections were estimated to recover within 12 weeks and return to baseline, with the exception of amputation and death, which were permanent end-health states. Past cost-effectiveness studies have used 4 weeks as a reasonable recovery period for minor infections.29,32 The example below illustrates how QALY was obtained for a 65-year old male patient that was expected to live up to age 73.7 years. This example was published in our previous works.
Life expectancy for an operative candidate for revascularization is 73.7 years (per Whitehall study). 21 For a 65-year-old patient, life expectancy is 8.7 years. A patient with a minor wound infection with Prevena is expected to have a utility of .572 and recover within 4 weeks. The utility of a successful surgery without complication is .706.
Number of Health Years Remaining = Average Life Expectancy – Average Age of Patient
73.7 years – 65 years = 8.7 years
Duration of Health State:
4 weeks/52 weeks = .08 years
QALYs:
(utility of health state) x (duration of health state) + (utility of successful procedure) x (remaining life years)
(.572) (.08) + (.706) (8.7 – .08) = 6.13 $/QALYs
Incremental Cost Utility Ratio
Using the QALYs and costs in the decision tree, incremental cost effectiveness ratio (ICER) was then calculated using the formula below:
An ICER of less than $50,000 was used to deem a surgical approach cost-effective. This ICER quotient assesses the value of a new device versus standard treatment and weighs the potential clinical benefit of the new device over the potential added cost that it may incur when used.
Deterministic Sensitivity Analysis
Fundamentally, sensitivity analyses (both deterministic or probabilistic) have been developed to determine whether the uncertainties in the literature with regards to varying outcomes and probabilities when assessing newer technologies against the standard of care effect the overall conclusion on whether or not a new device is cost-effective. To further evaluate the robustness and reliability of our model, we conducted sensitivity analyses (SA). One-way (deterministic) sensitivity analysis was conducted for each variable which was varied from the lowest to the highest values (as described in the literature) to determine the impact on our result. Tornado analysis (another form of deterministic sensitivity analysis) was performed to identify the greatest variable(s) of uncertainty with a range of variables from both industry funded and unfunded studies.
Subgroup Analysis
To reduce industry bias, we specifically analyzed ranges for probability of minor and major wound infections with and without Prevena that were obtained from studies with no financial conflict of interest and included these studies in the Tornado diagram. This was performed to evaluate if results differed when only studies without industry conflicts of interest were included.
Probabilistic Sensitivity Analysis
The second form of SA was the probabilistic sensitivity analysis using Monte Carlo simulation. In this form of SA, the effect of simultaneously changing the values of variables is based on the SD obtained from the literature. Variables included in this probabilistic sensitivity analysis were: cost of Prevena (gamma distribution), utility of successful surgery (beta distribution), utility of wound infection (beta distribution), probability of successful surgery without Prevena (beta distribution), and probability of successful surgery with Prevena (beta distribution). In general, a conclusion that deems a new technology more cost-effective is seen as reliable and robust if the Monte Carlo probabilistic sensitivity analysis favors the new technology as the more cost-effective option greater than 80% of the time when the simulations are performed.
Decision-Analysis Quality Assessment
The cost-utility and decision analysis design followed value analysis consensus guideline recommendations described by the CHEERS criteria. 33
This study was done in accordance with the principles outlined in the Declaration of Helsinki.
Results
Cost-Effectiveness for Each Treatment Arm.
Deterministic Sensitivity Analysis
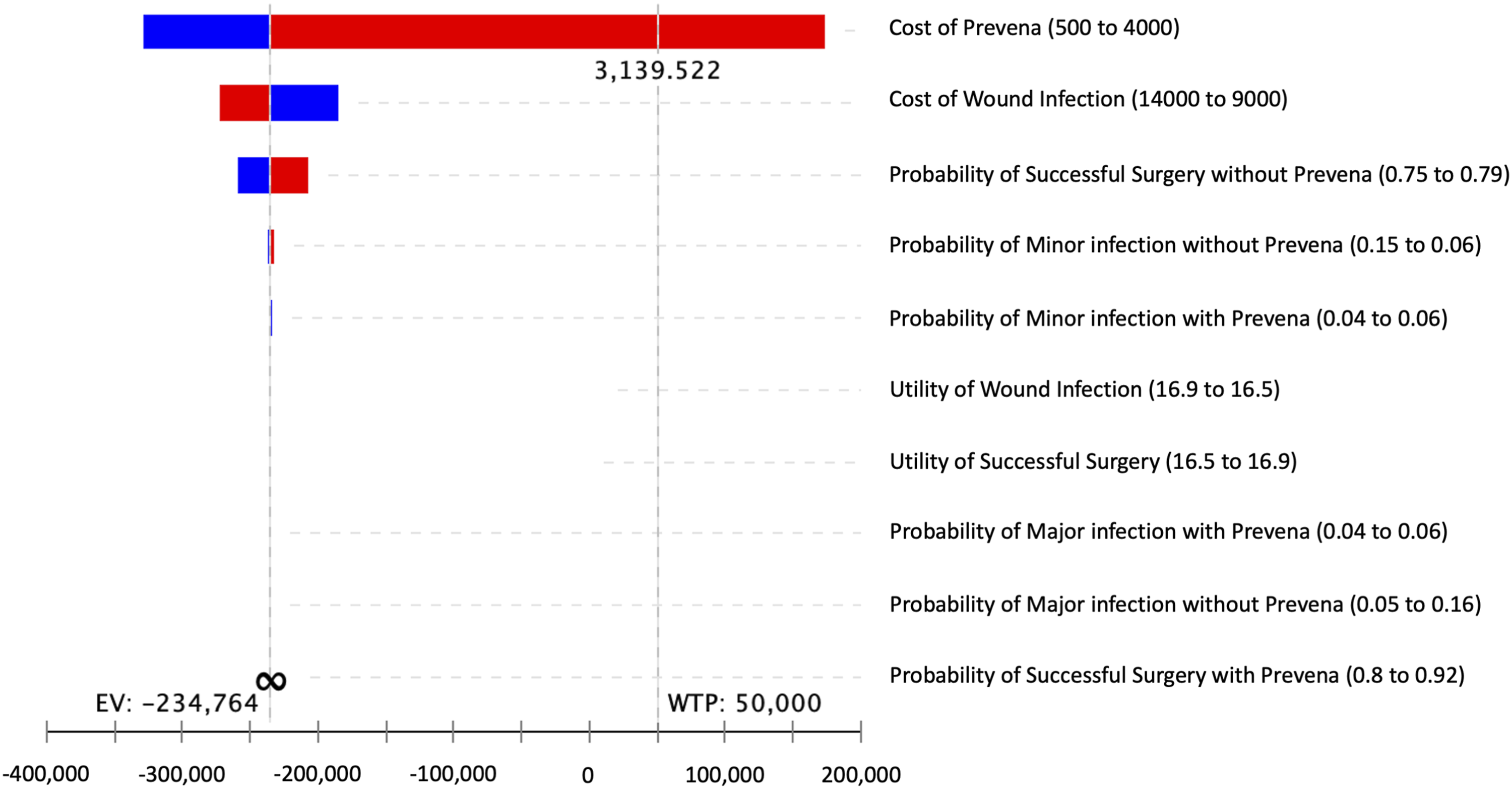
In one-way, deterministic sensitivity analysis, femoral-popliteal bypass without Prevena reached a threshold point and was the more cost-effective strategy if the probability of successful surgery in the Prevena arm was less than 84.9% (Figure 2A). As such, it would not be cost-effective to use the Prevena in a surgeon’s practice if the rate of successful surgery when using a Prevena was less than 84.9%. Similarly, femoral-popliteal bypass without Prevena reached a threshold point and became the more cost-effective strategy when the cost of Prevena exceeds $3139 (Figure 2B). A Tornado diagram analysis (Figure 3), with uncertainty around the mean value for each of the variables studied derived from the literature, identified the cost of Prevena as the greatest variable of uncertainty. (A)One-way Sensitivity Analysis. At WTP of 50,000, surgery without Prevena becomes the more cost-effective strategy if the probability of successful surgery falls below 84.9%. (B) One-way Sensitivity Analysis. At WTP of 50,000, surgery without Prevena becomes the more cost-effective strategy if the cost of Prevena exceeds $3139. Tornado Diagram (ICER) identifying the greatest variable of uncertainty as the cost of Prevena.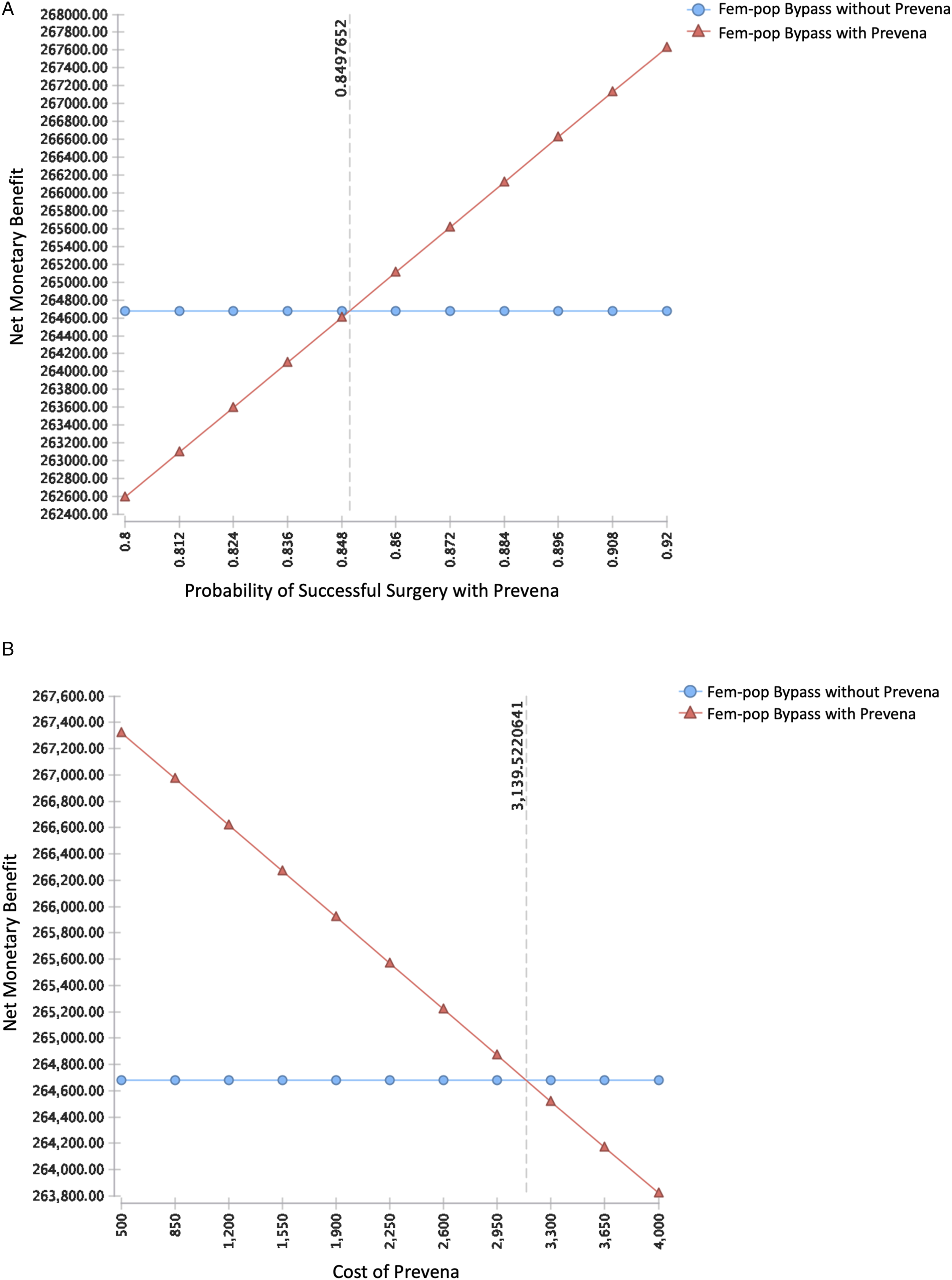
Subgroup Analysis
Using the highest impact variables from the Tornado diagram, we performed a subgroup analysis of non-industry sponsored studies. This Tornado diagram took into account the range of probabilities for minor and major wound infections with and without Prevena derived from unfunded studies. None of the probability variables demonstrated a threshold point that would contradict our conclusion. Thus, even when looking at solely unfunded studies, results favored Prevena as a cost-effective option in this patient population.
Probabilistic Sensitivity Analysis
With probabilistic sensitivity analysis, we used Monte Carlo simulation to manipulate several variables at the same time while running 10,000 simulations, and demonstrated a confidence of 99.07% in favor of femoral-popliteal bypass with Prevena (Figure 4). Probabilistic Sensitivity Analysis Monte Carlo Acceptability at WTP $50,000. A confidence of 99.07% that our conclusion, Prevena use with Femoral-popliteal bypass is the cost-effective strategy.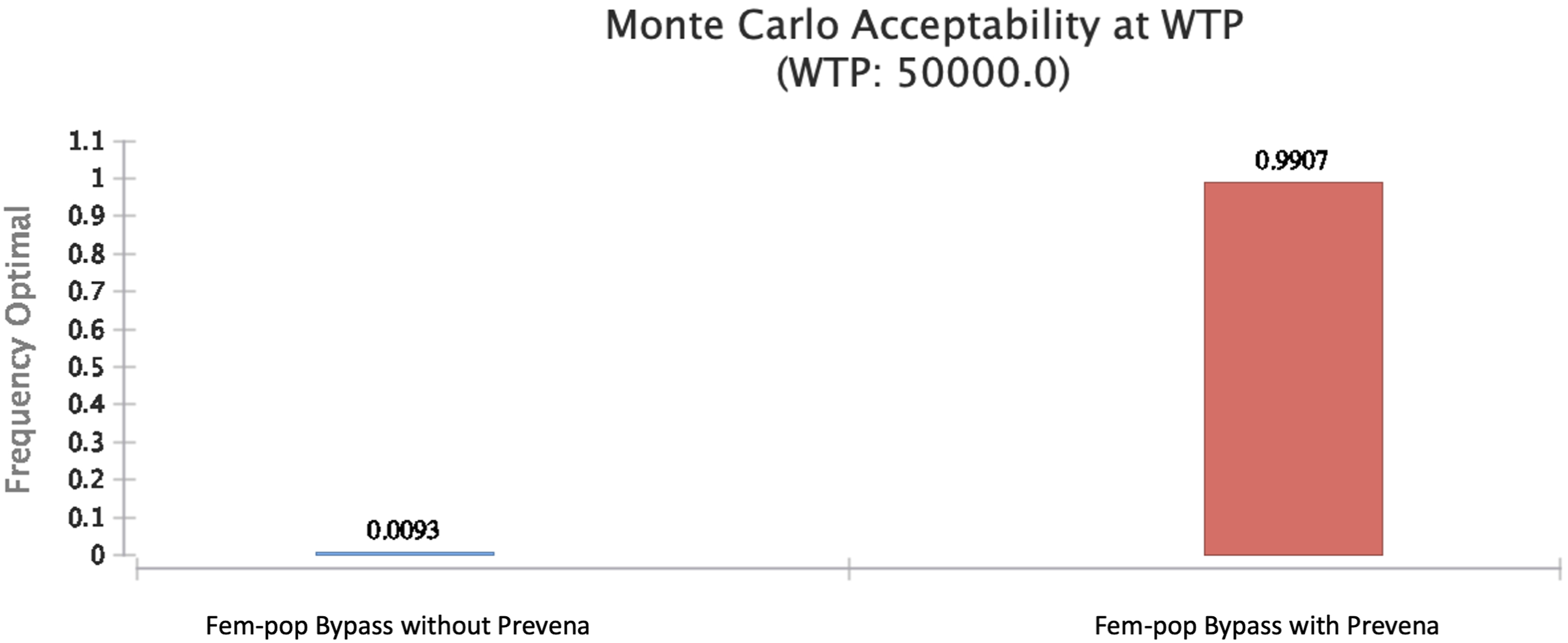
Discussion
Lower extremity bypass procedures with closed surgical incisions present with a high risk of post-operative complications, only second to hip and knee arthroplasty. 34 This is thought to be secondary to the risk of lymphatic disruption and a robust bacterial burden in the groin. 35 In addition to this, peripheral vascular disease confers an even higher risk of post-operative complications. 34 These postoperative complications include wound dehiscence and SSI, among others. To mitigate these risks, technologies such as the Prevena closed-incision negative pressure therapy (P-CINPT) have been developed and put into practice. This innovative device is applied intraoperatively and left in place for up to 7 days. The application of closed incision-negative pressure to the surgical site improves healing by maintaining a sterile environment and offloading midline tension by decreasing lateral forces.18,34 In addition, P-CINPT also maintains the beneficial effects of negative pressure therapy including the removal of excessive fluid and inflammatory mediators, promotion of a moist wound environment, decreasing bacterial colony counts, as well as increasing granulation, angiogenesis, and blood flow through microcirculatory effects to the wound edges.34,36
Previous meta-analyses have demonstrated a clear reduction in groin incision SSIs following vascular surgery bypass procedures when utilizing incisional negative pressure wound therapy (including Prevena) compared to standard dressings.37,38 Despite this apparent benefit, there are no current evidence-based guidelines on closed-incisional negative pressure therapy to reduce the risk of SSIs in groin incisions in vascular surgery. 37 To further elucidate the utility of closed-incisional negative pressure therapy in vascular surgery groin incisions, a cost-effectiveness analysis was undertaken using a femoral-popliteal bypass using prosthetic graft as a model. It is important, however, to first mention that the risk of SSI is not solely related to the use of incisional negative pressure wound therapy, but instead highly dependent on patient comorbidities, including body mass index, smoking, diabetes mellitus, preoperative nutritional status, reoperations, and intraoperative conditions (hypothermia, volume replacement, and prolonged ischemic time).
Our results demonstrate a clear cost-effectiveness benefit favoring the use of Prevena for groin incisions in femoral-popliteal bypass. While a .01 QALY is small, it actually represents a meaningful clinical benefit when calculating the ICER (incremental cost effectiveness ratio), which is the ratio of clinical effectiveness (QALY) and cost.29,39 In this study, the strongly negative ICER indicates that CINPT is the dominant strategy. This is due primarily to the higher probability of successful surgery and fewer major wound infectious complications within the Prevena arm. The cost of Prevena is offset by these favorable clinical outcomes.21,24-28 Overall, these data support the adoption of Prevena ciNPT for groin incisions in femoral-popliteal bypass. It is more cost-effective to use this innovative technology in vascular groin incisions to decrease infectious wound complications and promote the probability of a successful operation.
While novel, this study is not without its limitations. First, the method of cost-utility analysis relies on utility scores, which are obtained from a thorough literature review. These scores are subject to variation and bias as these utility scores are derived from validated surveys given to surgeons, and overlook the patient perspective, which may result in an over- or under-estimate of clinical effectiveness. Nevertheless, our Monte Carlo simulation favored CINPT, even with taking into account this potential variation in utility scores. There are additional shortcomings using this pooled data from a literature review both with respect to utility scores and probability of surgical outcomes. The studies in our literature review included those that were independently funded as well as industry sponsored. To account for this and to attempt to remove potential industry bias, we performed a sub-group sensitivity analysis to include a range of successful surgery and infectious wound complication probabilities from studies without reported industry sponsorship in order to demonstrate if results differed when including data from studies with industry sponsorship versus those without. This sensitivity analysis did not see a threshold point that flipped our conclusion favoring the use of Prevena in any of the studied variables indicating that there was not substantial bias from industry sponsorship influencing our results. It is imperative to acknowledge that even though the use of Prevena decreases complication rates, there is still inherent bias associated with the study of medical devices. Nonetheless, this study is important as vascular graft infections are associated with not only significant morbidity and mortality to the patient but also a significant healthcare cost burden $640 million annually in the United States. 40
Lastly, a limitation of this study is the use of the third-party payer perspective to calculate costs. Our analysis did not account for costs from a societal perspective, which would have included total costs to the patient, including costs accounting for loss of productivity, waiting time, transportation, and absence from work, or from a hospital perspective. Therefore, the use of the third-party payer perspective does not reflect the total targeted hospital charges other providers and patients may experience, nor does it reflect the overall healthcare cost burden with a major infection. Despite this, the third-party payer perspective is well defined and accepted within the realm of cost-utility literature, most notably the CHEERS criteria checklist.33,39,41-47
Conclusions
Despite the added device cost of the Prevena closed incision negative pressure therapy, its use is cost-effective in vascular surgery operations using groin incisions with femoral-popliteal bypass as a model.
Footnotes
Authors’ Note
Meeting Presentation: Presented virtually at SCVS March 13-17th in Miami, FL.
Author Contributions
All authors who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take responsibility for the content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Chatterjee has a consulting relationship with KCI.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.