
Abstract

Literature on the role of cardiopulmonary resuscitation (CPR) and epinephrine in both adult and pediatric traumatic cardiac arrest (TCA) has been conflicting.1-4 Studies have reported that despite CPR, provided in the pre-hospital or emergency department setting, survival rates of TCA patients remain poor.1,2 Additional reports have suggested that while epinephrine may increase return of spontaneous circulation (ROSC) in TCA, it may negatively impact outcomes including long-term survival and favorable neurological outcome. 4 Thus, the impact of epinephrine and CPR in pediatric TCA is unclear and warrants further investigation.
The objectives of this study were to describe the use of CPR and epinephrine in children with TCA and to compare the clinical characteristics between survivors and non-survivors.
We performed a retrospective cohort study of children ≤18 years of age with TCA who were treated between January 1st, 2010, and December 31st, 2019 at the emergency department of one of the following three urban tertiary care hospitals: Site A: a pediatric center with 1200 annual injury related visits and Sites B and C: two regional adult trauma centers that collectively see approximately 2500 trauma visits per year, of which 17% are pediatric. Children with TCA who were evaluated at the two adult facilities, and subsequently transferred to the pediatric center, were only included once as part of their respective institutional cohort. Children with cardiac arrest due to medical causes and drowning were excluded. Patients were identified from a pre-existing trauma registry that is updated and maintained by trauma teams of all three hospitals. This database was queried for children evaluated for TCA during the study period. We defined TCA as cardiac arrest occurring secondary to an injury (blunt or penetrating). All data were extracted from the electronic medical record and transferred to an excel spreadsheet by a trained research assistant. Data extraction was reviewed for accuracy and context by the principal investigator. Information was collected on demographics, date of injury, type of injury (blunt vs penetrating), Injury Severity Score (ISS), CPR duration, pre-hospital management, epinephrine doses and frequency, interventions performed, and patient outcomes. Complete neurologic recovery was defined as recovery without any neurological deficits at the time of discharge. The study was approved by the Institutional Review Board. Descriptive statistics were reported using general measures of frequency and central tendency. A series of chi-square, fisher’s exact, and Mann-Whitney U tests were conducted to provide an unadjusted comparison of patient and clinical characteristics associated with survival after a traumatic cardiac arrest. Data were screened for pattern and completeness; no missing data were found. Statistical inferences were made based on a two-tailed alpha of .05 and/or a 95% confidence interval. Analyses and data manipulations were performed using the stats package in R version 3.6.0.
Demographics and Characteristics of Traumatic Cardiac Arrest Patients (N = 62)
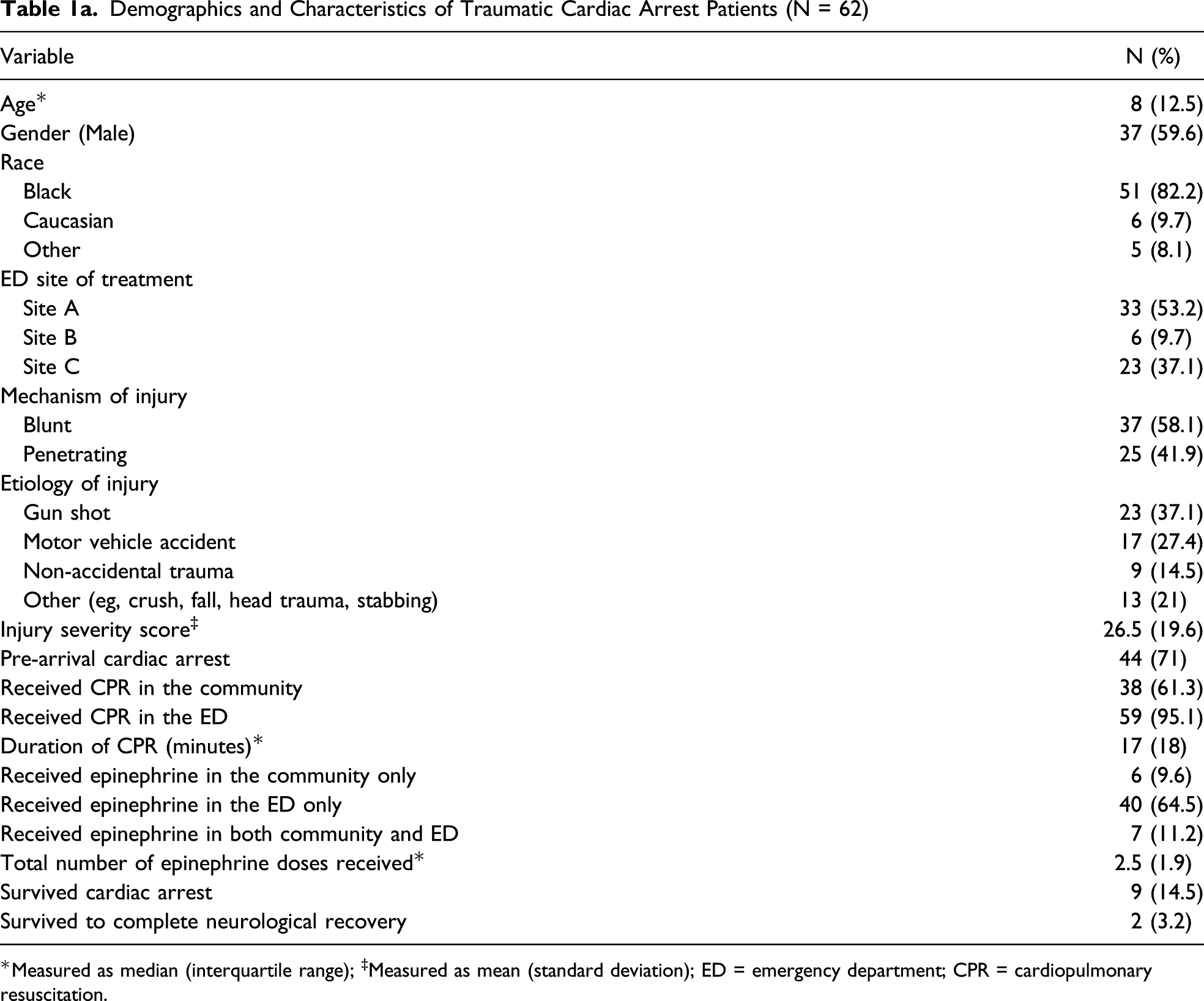
*Measured as median (interquartile range); ‡Measured as mean (standard deviation); ED = emergency department; CPR = cardiopulmonary resuscitation.
A CPR dose of epinephrine was administered in 53/62 patients (85.4%) either pre arrival (n = 6), in the ED (n = 40) or both in the ED and community (n = 7). Among those who received epinephrine, 56.6% (n = 30) received via intraosseous route while 43.4% (n = 23) received via intravenous route. No patients received a dose of epinephrine through the endotracheal tube. The median number of epinephrine doses was 2.5 (IQR 1.9) (Table 1a). One child with blunt trauma secondary to a crush injury received a total of 23 doses of epinephrine.
Comparison of Prognostic Factors Between Survival Status.
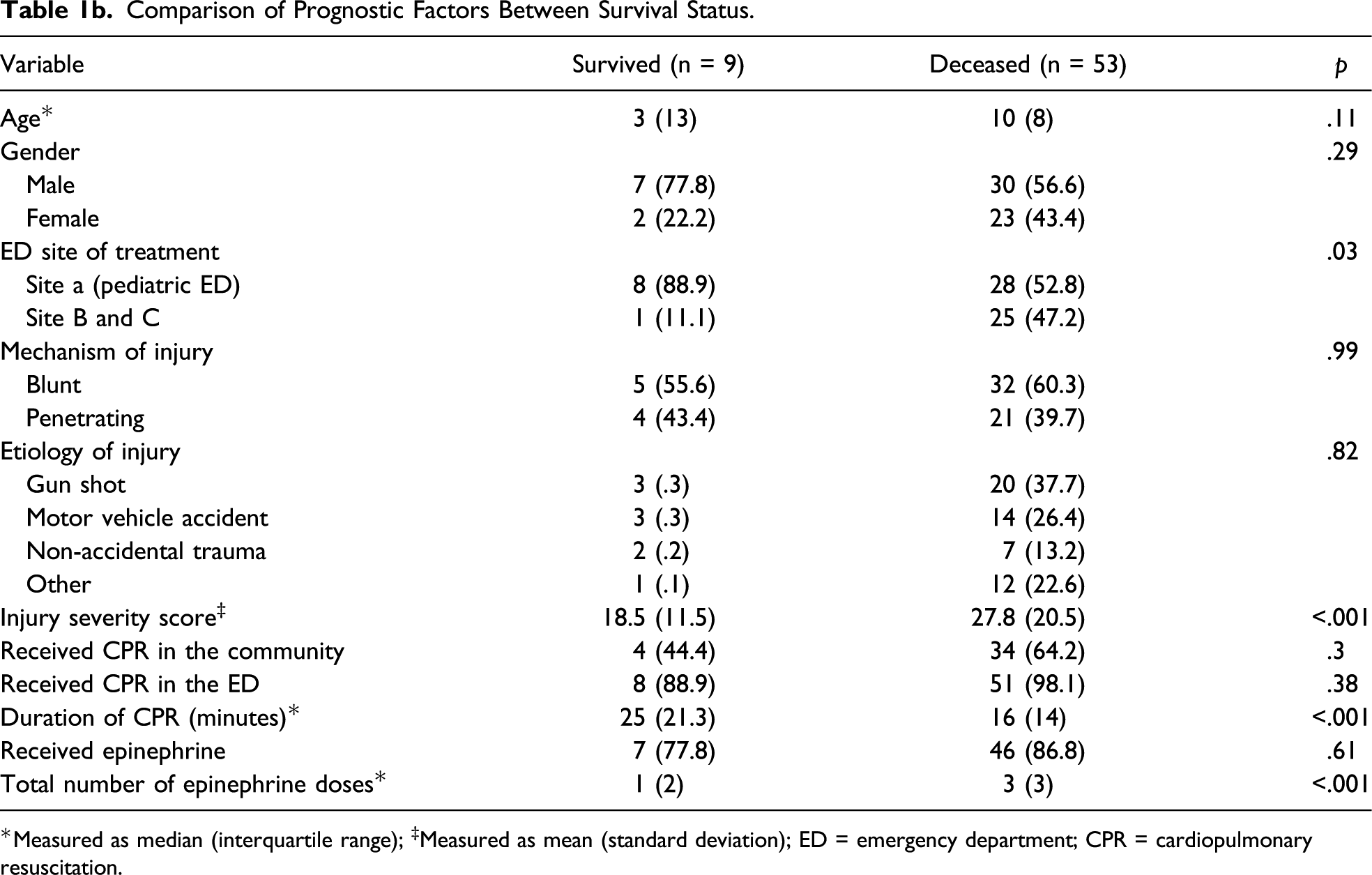
*Measured as median (interquartile range); ‡Measured as mean (standard deviation); ED = emergency department; CPR = cardiopulmonary resuscitation.
Our study describes the use of CPR and epinephrine in a cohort of pediatric TCA patients evaluated in three trauma centers. We found that compared to non survivors, those children who survived received a longer duration of CPR and lesser numbers of doses of epinephrine.
Previous studies have reported on the poor efficacy of CPR among TCA in adult patients.1,2 In contrast to these studies, we found survivors in our cohort had a longer duration of CPR compared to the non-survivors. This suggests that there may be a role for CPR in children following TCA, although this should not distract from addressing crucial reversible causes of TCA, such as tension pneumothorax or hemorrhagic shock. Reports on the efficacy of epinephrine have conflicting results in both adult and pediatric populations and mostly suggest ROSC or short term survival.3,4
Lin et al examined pediatric TCA patients and found that early administration of epinephrine temporarily increased heart rate and blood pressure in the initial post-resuscitative period but did not significantly increase the rates of survival or favorable neurologic outcomes. 4 Similarly, in our study although the survival rate was 14.5%, only 2 children were neurologically intact at discharge. This suggests that aggressive resuscitation with multiple doses of epinephrine may not translate into favorable neurological outcomes in pediatric TCA and warrants further large scale investigation.
Our study had limitations. First, our sample size was small and restricted to three EDs and hence may not be applicable to other centers. However, this study is representative of 10 years of data collection, reiterating the low incidence of pediatric TCA. Additionally, in our study there was a difference in ISS among survivors and non-survivors, indicating that injuries may have been less severe in those who survived, which may have impacted our results. However, regardless of this difference in ISS all patients in our cohort sustained cardiac arrest following their injury. Lastly, the retrospective nature of study limits retrieval of data to what is available in the electronic medical record.
In this study of pediatric TCA, we found that survival to complete neurological recovery remains poor. The duration of CPR was longer among children who survived a TCA. Although the use of epinephrine in children with TCA was high, survivors received less doses compared to non-survivors. Larger studies are needed to confirm these findings and determine the efficacy of epinephrine and CPR in pediatric TCA.
Footnotes
Author Contributions
Authors US, CK, and LD designed the study. Authors KL, RA, US, and LD performed data interpretation, writing and critical revisions of the manuscript and tables for important intellectual content; Author FM conducted data analyses and critically reviewed the manuscript for important intellectual content; Authors US, AA, CK, and DC were involved in data acquisition, statistical analysis and manuscript writing and revisions. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.