
Abstract
Background
Traumatic breast injuries that require surgical intervention are rare and incompletely studied. The study objective was to define the incidence, mechanism/burden of injury, interventions, and outcomes after breast injuries requiring surgery nationally.
Methods
All patients with breast trauma necessitating surgery were identified from the National Trauma Data Bank (NTDB) (2006-2017) using ICD-9 and -10 codes, without exclusions. Demographics, injury mechanism/severity, procedures, and outcomes (mortality, hospital length of stay [LOS, days], ICU LOS, and AIS >1 in >1 body regions, defining multisystem trauma) were compared with ANOVA or Chi-squared tests, as appropriate.
Results
In total, 899 patients (.01% of NTDB) met study criteria. Median age was 41 years and most patients were female (n = 802, 89%). Penetrating trauma was the most common injury mechanism (n = 395, 44%), followed by blunt trauma (n = 369, 41%) and burns (n = 135, 15%). Median ISS was higher after blunt trauma than penetrating trauma or burns (10 vs 5 vs 4, P < .001). Laceration repair/mastotomy was the most common procedure among penetrating (n = 354, 90%) and blunt (n = 265, 72%) trauma patients, while mastectomy was the most common after burns (n = 126, 93%). Breast procedures varied significantly by mechanism (P < .001).
Conclusion
Breast injuries requiring surgery are uncommon. Most occur following penetrating trauma, although injury severity is highest after blunt trauma and mortality is highest after burns. Procedure type, injury severity, and outcomes varied significantly by mechanism of injury, implying that breast trauma should be considered within the context of injury mechanism. These findings may assist with prognostication after breast trauma necessitating surgical intervention.
Key Takeaways
Breast trauma necessitating surgical intervention is uncommon across the United States and varies in frequency, trauma severity, and outcomes by mechanism of injury. This may help inform discussion with patients and their families following trauma. The type of surgical intervention pursued after breast trauma varied significantly by mechanism of injury, suggesting that surgical planning after breast injury must be considered with the context of the traumatic mechanism.
Introduction
Traumatic injuries to the female breast that require surgical intervention are rare and incompletely studied. In the United States, trauma accounts for over 150,000 deaths per year and is the fourth leading cause of death for all ages. 1 The incidence of trauma to the female breast is unknown and currently, there is no standardized algorithm for the evaluation and treatment of these injuries. Furthermore, little is known about the correlation between different types of breast injuries and clinical outcomes. The majority of prior research is comprised of single-institution case studies and investigations of only one mechanism of trauma or injury type.2-8 The purpose of this study was to define the incidence, mechanism/burden of injury, interventions, and outcomes after breast injuries requiring surgery on a national level. We hypothesized that patient demographics, surgical procedure incidences, and outcomes would differ significantly based on mechanism of injury.
Methods
This is a retrospective observational study using the National Trauma Data Bank (NTDB), which aggregates de-identified patient data from medical centers across the United States into the largest trauma registry in existence. 9 The NTDB was queried for all patients who underwent breast surgery following traumatic injury between 2007 and 2016. Breast surgeries were identified using procedure codes for laceration repair/mastotomy (85.0, 85.81, 85.94, and 85.96) and mastectomy (85.2, 85.3, and 85.4). Procedure codes were also used to identify patients who underwent skin flap creation (85.82 and 85.83) or complex reconstruction (85.70-85.79, 85.84, and 85.85). There were no exclusions. Our Institutional Review Board reviewed this project and deemed it exempt, with a waiver of informed consent on the basis of the study design.
Patient baseline characteristics including age, sex, comorbidities, Emergency Department (ED) arrival heart rate, ED arrival systolic blood pressure (SBP), and ED arrival Glasgow Coma Scale (GCS) were collected from the NTDB. Injury characteristics including Abbreviated Injury Scale (AIS), Injury Severity Score (ISS), and injury mechanism were also collected. Multisystem trauma was defined as more than one AIS body region with AIS score >1.
Patients were categorized by mechanism of injury: blunt, penetrating, and burn. Patient baseline characteristics across the three groups were compared using univariable analysis including analyses of variance for continuous variables and chi-square tests for categorical variables. Data were collected and analyzed using SPSS version 20.0 (IBM Corporation, Armonk, NY). Statistical significance was defined as P < .05.
Results
Patient Demographics, Clinical Data, and Injury Data
Demographics, Injury and Clinical data of Breast Trauma Patients.
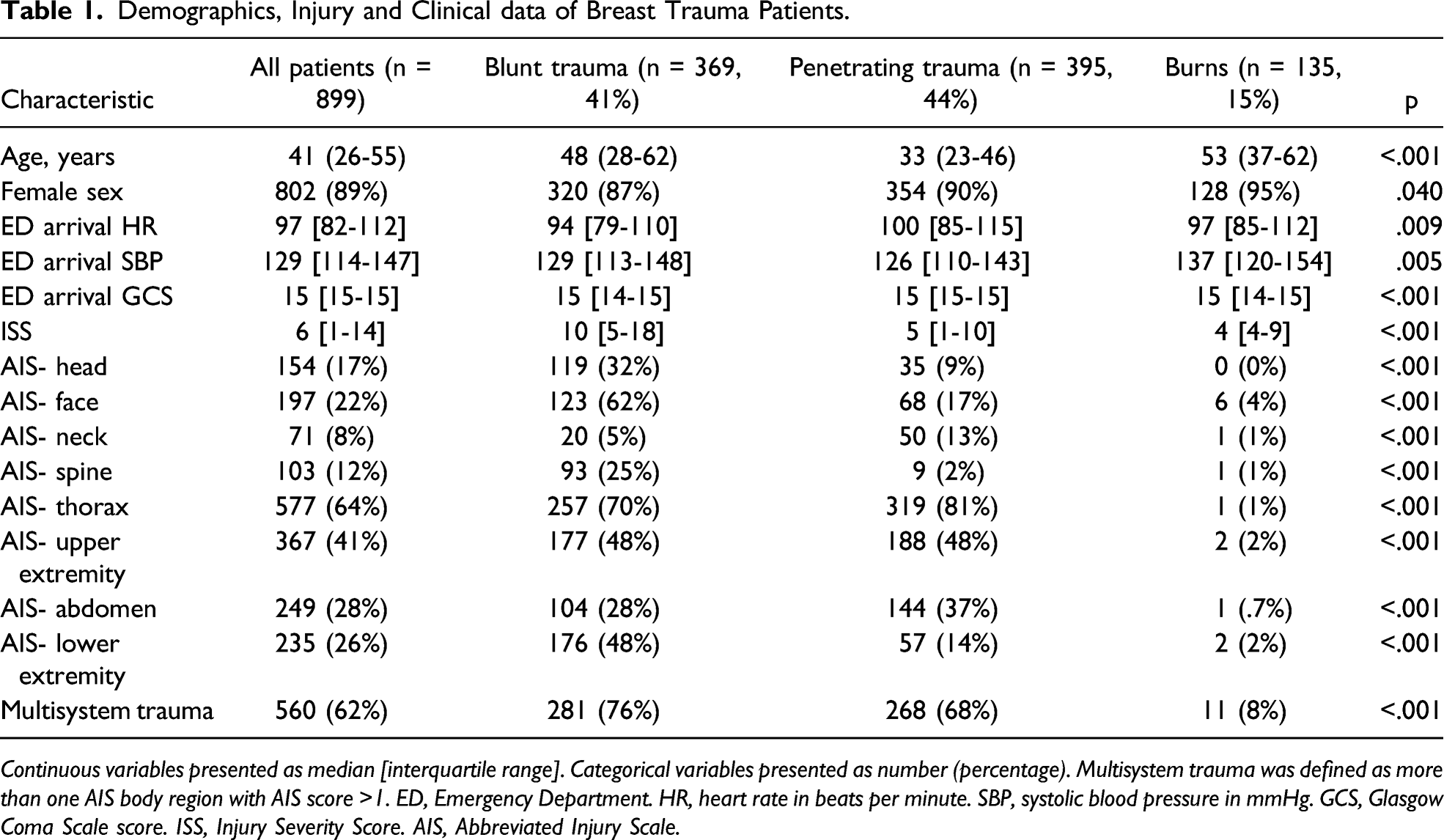
Continuous variables presented as median [interquartile range]. Categorical variables presented as number (percentage). Multisystem trauma was defined as more than one AIS body region with AIS score >1. ED, Emergency Department. HR, heart rate in beats per minute. SBP, systolic blood pressure in mmHg. GCS, Glasgow Coma Scale score. ISS, Injury Severity Score. AIS, Abbreviated Injury Scale.
Surgical Intervention for Breast Trauma
Type of Operative Intervention for Breast Trauma Patients.
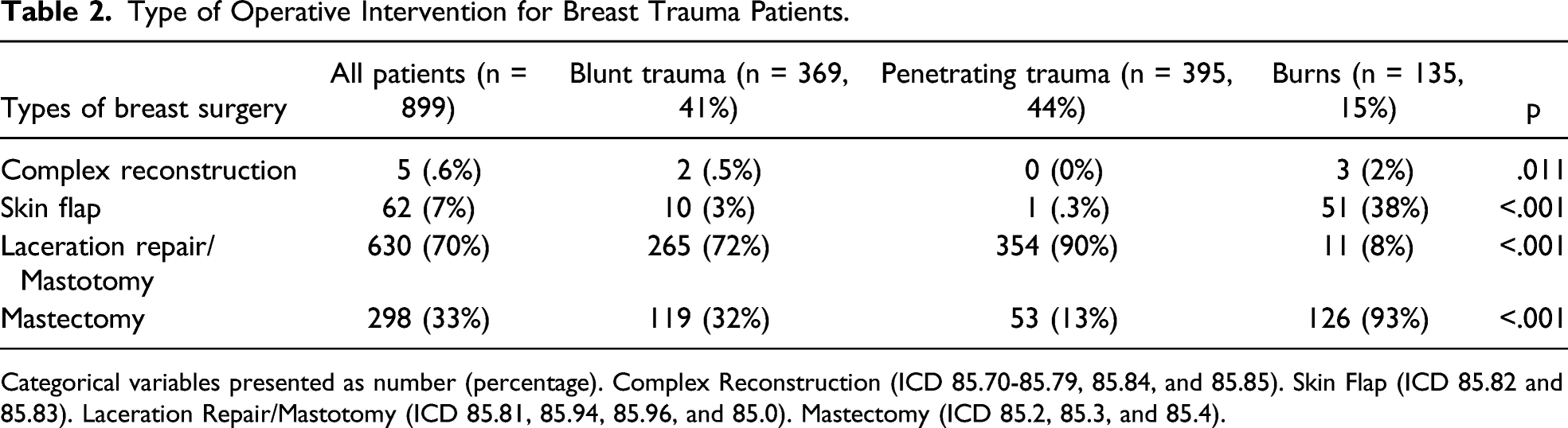
Categorical variables presented as number (percentage). Complex Reconstruction (ICD 85.70-85.79, 85.84, and 85.85). Skin Flap (ICD 85.82 and 85.83). Laceration Repair/Mastotomy (ICD 85.81, 85.94, 85.96, and 85.0). Mastectomy (ICD 85.2, 85.3, and 85.4).
Outcomes
Outcomes of Breast Trauma Patients.
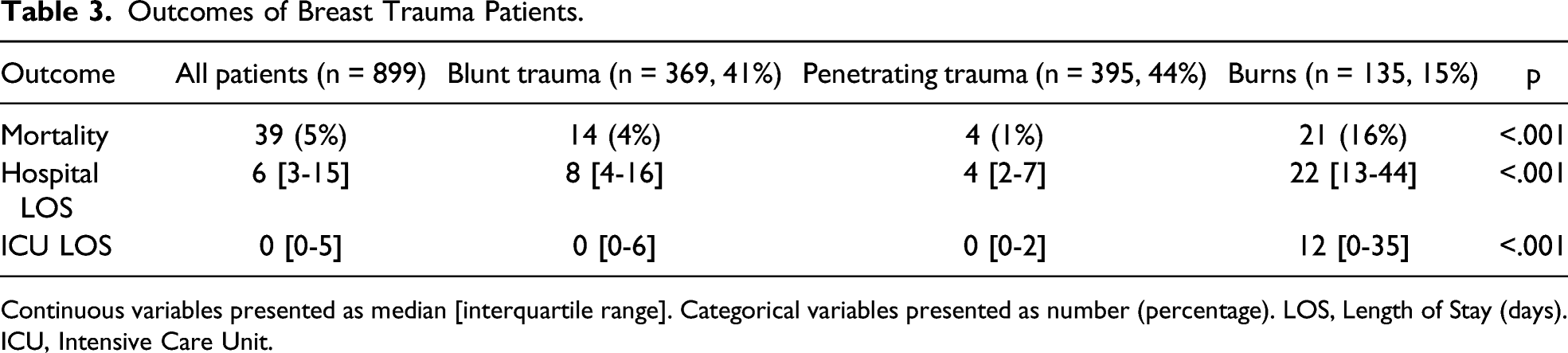
Continuous variables presented as median [interquartile range]. Categorical variables presented as number (percentage). LOS, Length of Stay (days). ICU, Intensive Care Unit.
Discussion
This nationwide study is the first to analyze the demographics and outcomes of breast trauma by mechanism of injury among patients necessitating operative interventions on the breast. The majority of prior research is comprised of case reports and/or only evaluates a single mechanism of breast injury.2-8 In this study of nearly 900 patients nationwide, we found that patient characteristics, type of surgical intervention, and outcomes varied significantly between blunt trauma, penetrating trauma, and burn patients. For example, mastectomy was the most common surgery after burn injuries, while laceration repair and mastotomy were more common following penetrating or blunt trauma. Burn patients had higher mortality rates, as well as longer hospital LOS and ICU LOS compared to blunt and penetrating trauma patients. Blunt and penetrating trauma patients, however, were more likely to sustain multisystem trauma.
The significance of breast trauma in the context of a trauma patient’s overall clinical status remains largely unknown. Trauma to the female breast can cause a spectrum of pathology that requires operative interventions, ranging from cosmetic deformities to life-threatening hemorrhage. Breast trauma may be associated with the presence of other more serious injuries, such as thoracoabdominal injuries seen with seatbelt signs, and therefore may indicate the need for further work-up.2-3 Sanders et al performed a single-institution retrospective chart review of 108 female patients treated for traumatic breast injuries secondary to blunt trauma at a level I trauma center. The overwhelming majority of patients (98%) were involved in motor vehicle accidents and all but 7 of the patients (94%) were treated nonoperatively for breast hematomas. Of the 7 patients who required intervention, 6 (86%) underwent angiography with selective angioembolization. The most commonly associated injuries were long bone extremity fractures (47%) and rib fractures (15%). 4
Additional research is needed to create a standardized injury classification and treatment system for female breast trauma. Majeski proposed one of the earliest classification systems of breast trauma secondary to seat-belt injuries. Injuries were divided into four classes based on clinical presentation with associated diagnostic and therapeutic recommendations. Contrast-enhanced computed tomography (CT) of the chest and surgical interventions were reserved for patients with the highest class of injury who sustained avulsion injuries with active bleeding. 5 Song et al later proposed a classification system for seat-belt injuries to the female breast based on the timing of presentation and clinical characteristics. Imaging and treatment recommendations were made based on each category. 6 Similarly, Sanders et al proposed a treatment algorithm which divided blunt breast trauma into simple versus complex injuries. 4 According to this algorithm, simple breast trauma in a hemodynamically stable patient can be managed conservatively, whereas complex breast trauma in a hemodynamically stable or unstable patient should undergo chest CT or exploration, respectively. Patients with blush seen on CT should be referred to Interventional Radiology for angiography and possible embolization. Notably, all of these classification systems are limited to a single mechanism of injury. Future classification systems and treatment algorithms should include multiple mechanisms of breast traumatic injuries in order to be applied more broadly. Additionally, each class of injury should ideally predict patient outcomes, such as hospital LOS and mortality, in order to aid with prognostication and formulating treatment plans.
We acknowledge the limitations of this study. First, this is a retrospective observational study, with the inherent biases and lack of granularity of this type of study design. Second, the specific impact of breast-related trauma on patient outcomes, rather than the effect of other injuries and trauma mechanism, is difficult to define. Many of the differences between patient characteristics and outcomes may reflect the inherent differences between the mechanisms of injury, rather than differences in the breast injuries themselves. A multi-center prospective study is warranted to better control for the effect of other injuries on outcomes, determine commonly associated injuries, and validate our study findings.
In summary, breast injuries necessitating surgical intervention are uncommon and incompletely understood. Most injuries occur following penetrating trauma, although injury severity is highest after blunt trauma and mortality is highest after burns. Surgical procedure type, injury severity, and outcomes varied significantly by mechanism of injury, implying that breast trauma should be considered within the context of the injury mechanism. The findings of this study may assist patients, clinicians, and families with prognostication following operative breast trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.