
Abstract
Background
Implementation of screening modalities has led to a decreased incidence of colorectal malignancies. Unfortunately, overall incidence has remained unchanged as cases have increased in patients below the suggested screening age. Therefore, we evaluated characteristics and oncological outcomes of malignancies in patients ≤40 years of age.
Methods
Single-center retrospective analysis of prospectively collected data of malignancies in patients ≤40 years evaluated in our institution between 2010 and 2016. Basic descriptors for demographic, clinical, histologic, and genetic data were collected. Disease-free survival (DFS) and 5-year overall survival (OS) were compared for patients between 30-40 years and <30 years.
Results
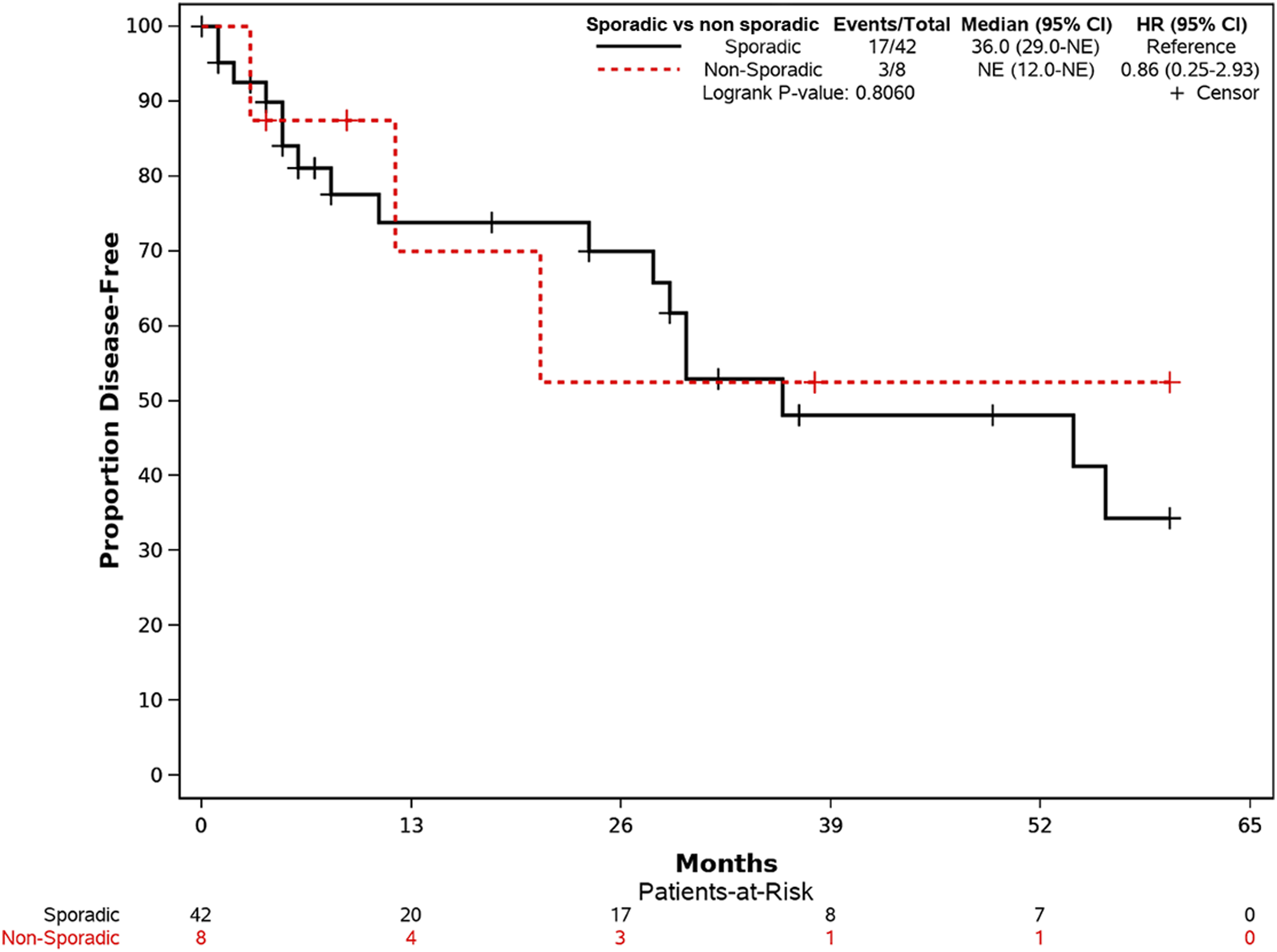
Fifty-six patients ≤40 years were identified, 44 of whom (96.5%) had adenocarcinomas. Most common malignancy location was the rectum (64.3%). Despite aggressive tumor characteristics such as moderate/poor differentiation (88.6%), lymphovascular invasion (26.8%), perineural invasion (21.4%), and advanced tumor stage T3/T4 (60.7%), OS rate was 94.6%. Both age groups had similar oncologic characteristics. There was a trend toward worse OS (2/11 and 1/45, P = .06) but not for DFS (7/11 and 15/43, P = .18) in patients <30 years of age compared to 30-40 years. There were no differences in OS (3/44 vs 0/88, P = .44) or DFS (17/42 vs 3/8, P = .80) between sporadic vs non-sporadic malignancies, respectively.
Conclusions
Patients ≤40 years of age with malignancy have advanced tumor stages and aggressive tumor characteristics at diagnosis. Although there is higher OS risk for patients <30 compared to those aged 30-40 years, no differences were found for DFS between these two groups.
Key Takeaways
Although the incidence of CRC in the young population ≤40 years of age is increasing compared to those >50 years of age, the relative incidence is still low. However, given this increasing incidence, CRC should be considered in this patient population. This study adds to the body of evidence that, despite the aggressive nature of CRC in patients ≤40 years of age, patients have good 5-year survival at approximately 94.6% at 5 years. It also highlights the fact that consideration for genetic counseling and testing may be indicated as a mutation may be found in >25% of patients and this has clinical implications for first degree relatives of affected individuals.
Introduction
The overall incidence of colorectal malignancy in patients >50 years has decreased in the United States during the past few decades likely because of the implementation of multiple malignancy screening methods to detect early cancers or premalignant lesions.1,2 Conversely, the incidence of malignancy in young patients has increased from 1.0% to 2.4% annually since the mid-1980s in adults aged 20 to 39 years and by .5% to 1.3% since the mid-1990s in adults aged 40 to 45 years. 3 Colorectal malignancies can be broadly divided into sporadic malignancy or hereditary colorectal malignancy syndromes which occur in about 3%-5% of patients. 4 Sporadic malignancies are more common and arise from multiple mutations in tumor suppressor genes and oncogenes that occur over time. Patients with sporadic malignancies are usually diagnosed around 70 years of age. 5 Conversely, HCCS are characterized by developing in younger patients and having multiple different genetic abnormalities. 4 Hereditary colorectal malignancies can be divided into non-polyposis syndromes and polyposis syndromes. Non-polyposis syndromes include hereditary non-polyposis colorectal cancer syndrome (HNPCC), or Lynch syndrome which is the most common HCCS that develops from germline mutations in the DNA mismatch repair gene mechanisms. 6 Polyposis syndromes can be divided into adenomatous, which include familial adenomatous polyposis syndrome (FAP) and MUTYH-associated polyposis syndrome (MAP) and into hamartomatous, which are rare and include Peutz-Jeghers syndrome, Juvenile polyposis syndrome, PTEN hamartoma tumor syndrome, and mixed hyperplastic polyposis syndrome. 4
The primary aim of this study was to assess clinicopathological factors and oncological outcomes of patients diagnosed with colorectal malignancies ≤40 years of age. The secondary aim was to assess the association between genetic profile and clinical demographics and the association between sporadic vs non-sporadic malignancies and clinicopathological characteristics of colorectal malignancies.
Methods
This is a single-center retrospective analysis of prospectively collected data in 56 patients ≤40 years of age diagnosed with colorectal malignancies between 2010 and 2016. Patients were divided into two groups: <30 years of age and 30-40 years of age. Clinical and demographic information for each patient including age, gender and race, tumor location, and surgery type was obtained. Pathological characteristics such as tumor site, histological subtype, tumor grade, lymph node involvement, American Joint Committee on Cancer (AJCC) staging, 7 recurrence, and survival were evaluated. Subjects were excluded from the study if they were >40 years of age or were lost to follow-up.
Tumor location was described as right-sided if the tumor was located in the cecum, ascending colon, hepatic flexure, or transverse colon; left-sided if the tumor was in the descending or sigmoid colon; and rectum. Overall survival (OS) time was calculated from the time of surgery to death. Disease-free survival (DFS) was defined as the length of time from the date of surgery to disease recurrence or last follow-up appointment documented in the electronic medical record. Patients were followed up by their respective colorectal surgeon, gastroenterologist, and/or primary care physician. Local recurrence (at the anastomosis and/or in adjacent lymph nodes) and distant recurrences were documented by clinical, radiological, and/or pathological diagnosis.
During genetic counseling, if patients had a clear clinical phenotype for a hereditary malignancy syndrome, they underwent syndrome-specific genetic testing on the basis of phenotype. Genetic testing for other patients was recommended after genetic risk assessment on the basis of personal and family histories of colorectal malignancy, as well as results of germline mutation testing and immunohistochemistry (IHC) tumor analyses. According to the results of the genetic testing, patients with genetic mutations were grouped in the non-sporadic malignancy group. HCCS were determined by abnormalities in IHC, germline mutation testing, KRAS and BRAF testing. FAP was determined on a clinical basis. Patients without a hereditary syndrome were classified as the sporadic malignancy group.
Statistical Analysis
Study data were collected and managed using RedCap electronic data capture tools hosted at our institution. 8 Data are presented as mean ± standard deviation, or frequency (percent). Univariate analyses were performed to assess differences between the subjects with age less than 30 years and the subjects with age of 30 to 40 years, as well as between the subjects with sporadic malignancy and the subjects without sporadic malignancy. Wilcoxon’s rank-sum test or t test was used to compare continuous variables, while chi-square test or Fisher’s exact test when appropriate was utilized to compare categorical variables. In addition, survival analysis was conducted to evaluate overall survival and disease-free survival truncated at 5 years for follow-up for all patients. Kaplan-Meier plots were generated, and log-rank tests were used to compare estimates between groups. All analyses were performed using SAS version 9.4 (SAS Institute Inc. Cary, NC, USA) and a P value of less than .05 was considered statistically significant.
This study was approved by our institution’s Institutional Review Board (IRB).
Results
Baseline Data
A total of 1469 patients were diagnosed with colorectal malignancies between 2010 and 2016 at our institution; 56 were ≤40 years of age and met the inclusion criteria for our study (Figure 1). Patients were predominantly male (53.6%) and were a mean age of 33.9 (±5.1) years. The most common type of malignancy was adenocarcinoma (including mucinous and signet cell subtypes) in 54 patients (96.5%). Overall, 30 (53.6%) patients were male and 37 (66.1%) had rectal cancer. Stage I was identified in 7 patients (12.5%), stage II in 5 patients (9.1%), stage III in 20 patients (35.7%), and stage IV in 24 patients (42.9%). A total of 3 (6.8%) died during an average follow-up of 35 (range, 1-204) months. Colorectal malignancy case selection flow gram.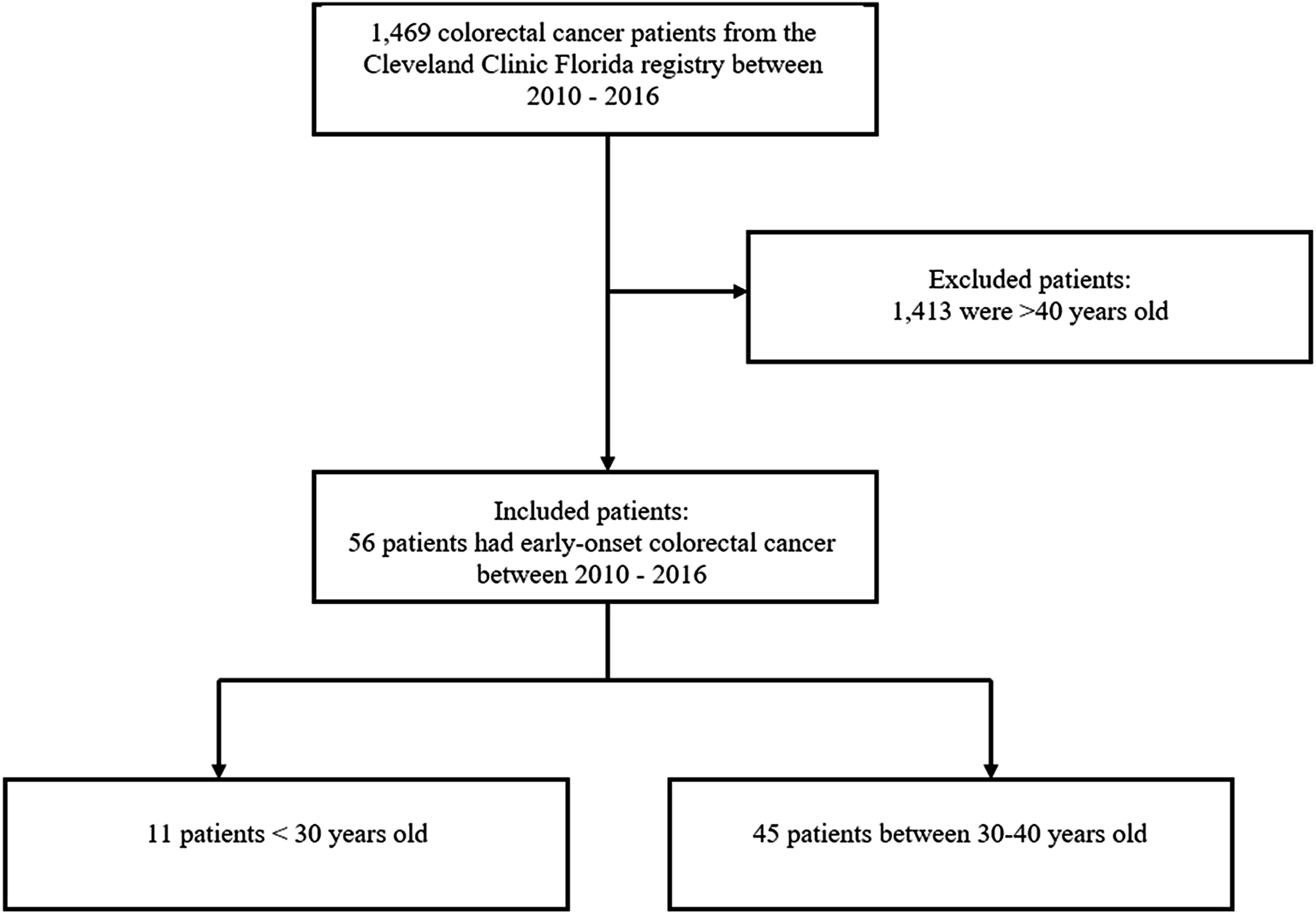
Characteristics by Age Group
Overall and Age-Group Baseline Demographic and Clinical Characteristics of Patients <40 Years Diagnosed with Colorectal Malignancies.
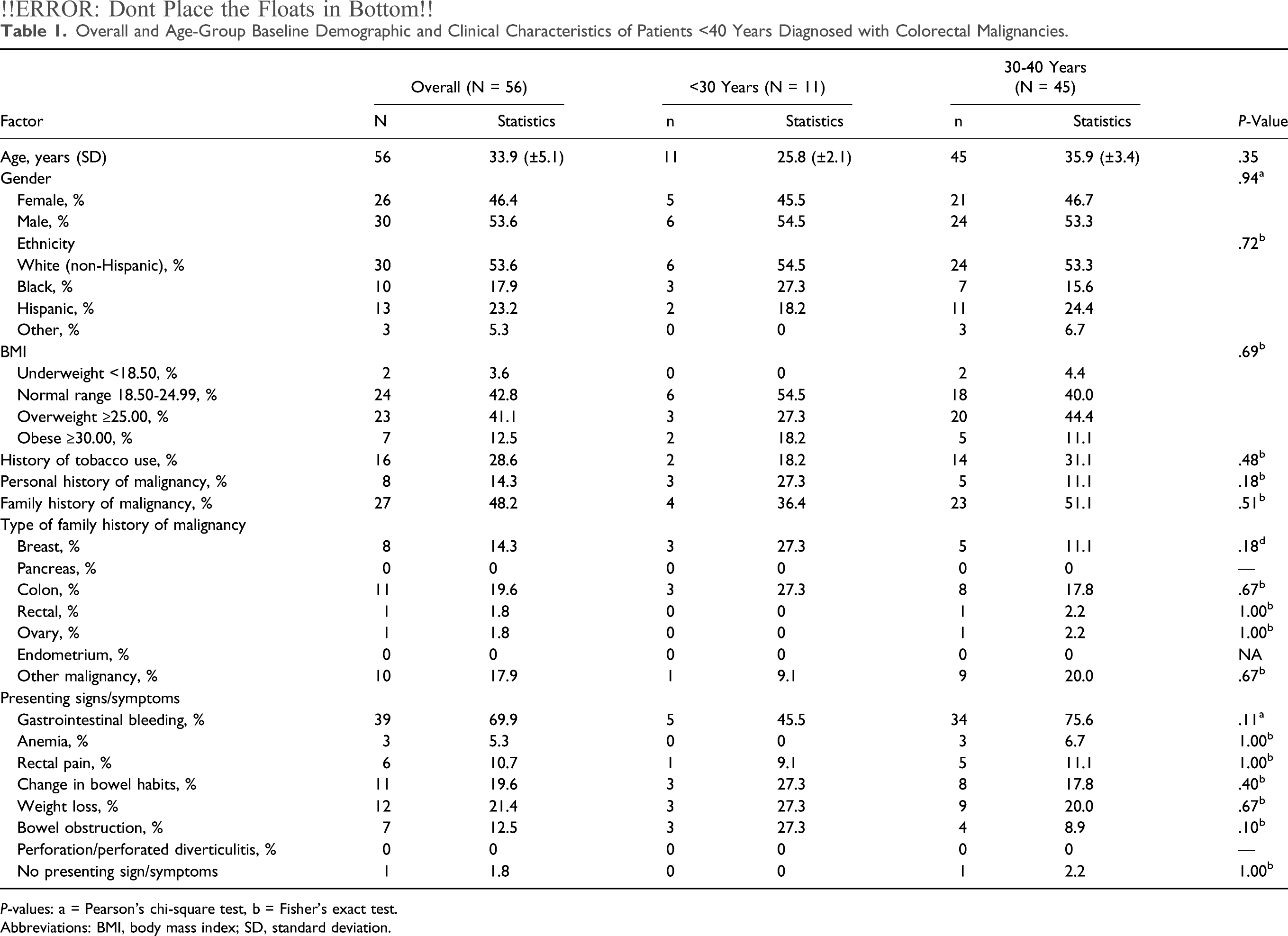
P-values: a = Pearson’s chi-square test, b = Fisher’s exact test.
Abbreviations: BMI, body mass index; SD, standard deviation.
Overall and Age-Group Clinicopathological Characteristics of The Patients with Early-Onset Colorectal Malignancy.
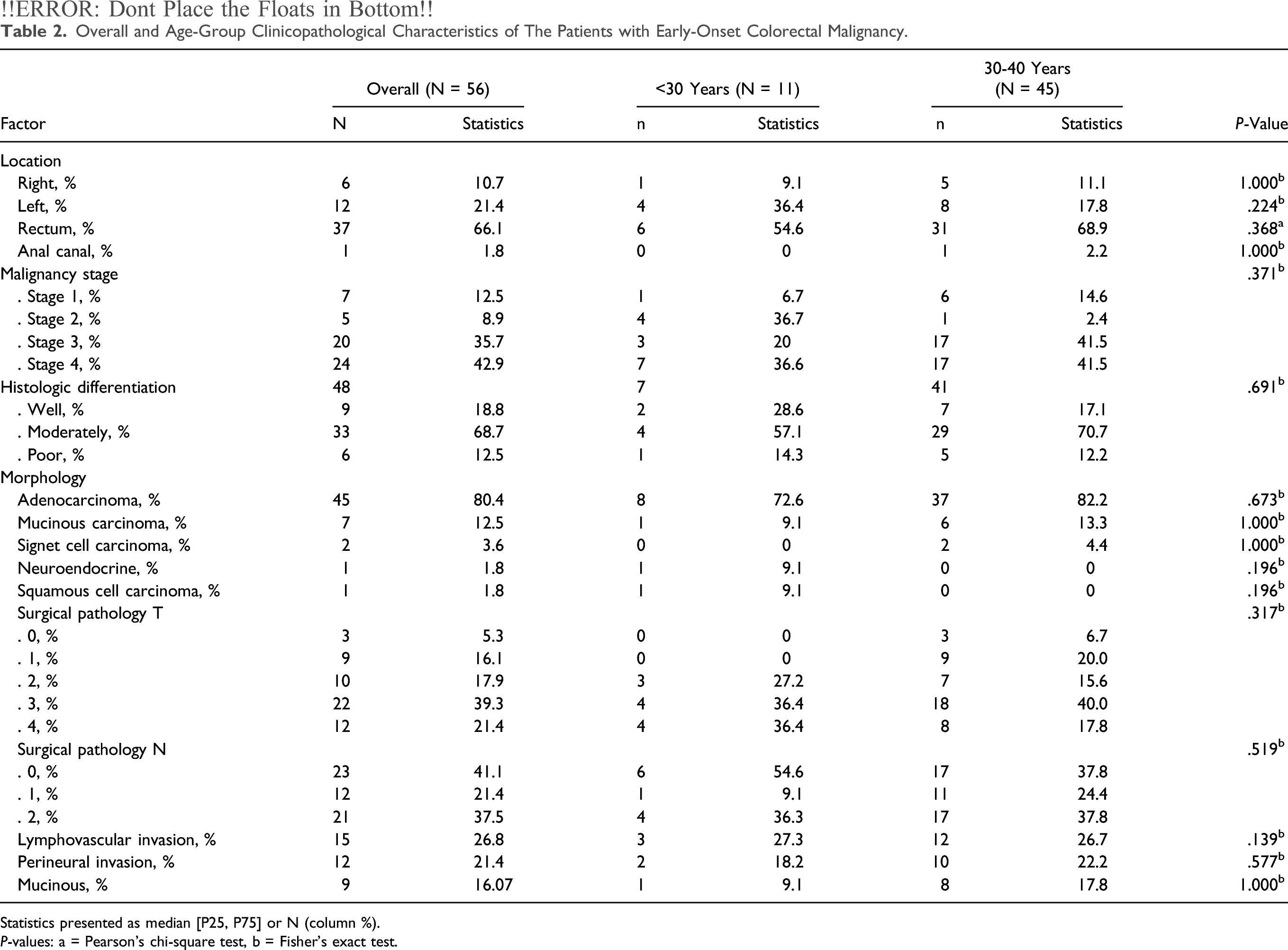
Statistics presented as median [P25, P75] or N (column %).
P-values: a = Pearson’s chi-square test, b = Fisher’s exact test.
Genetics
Genetic Testing Patterns in Patients with Early-Onset Colorectal Malignancy and Outcomes.
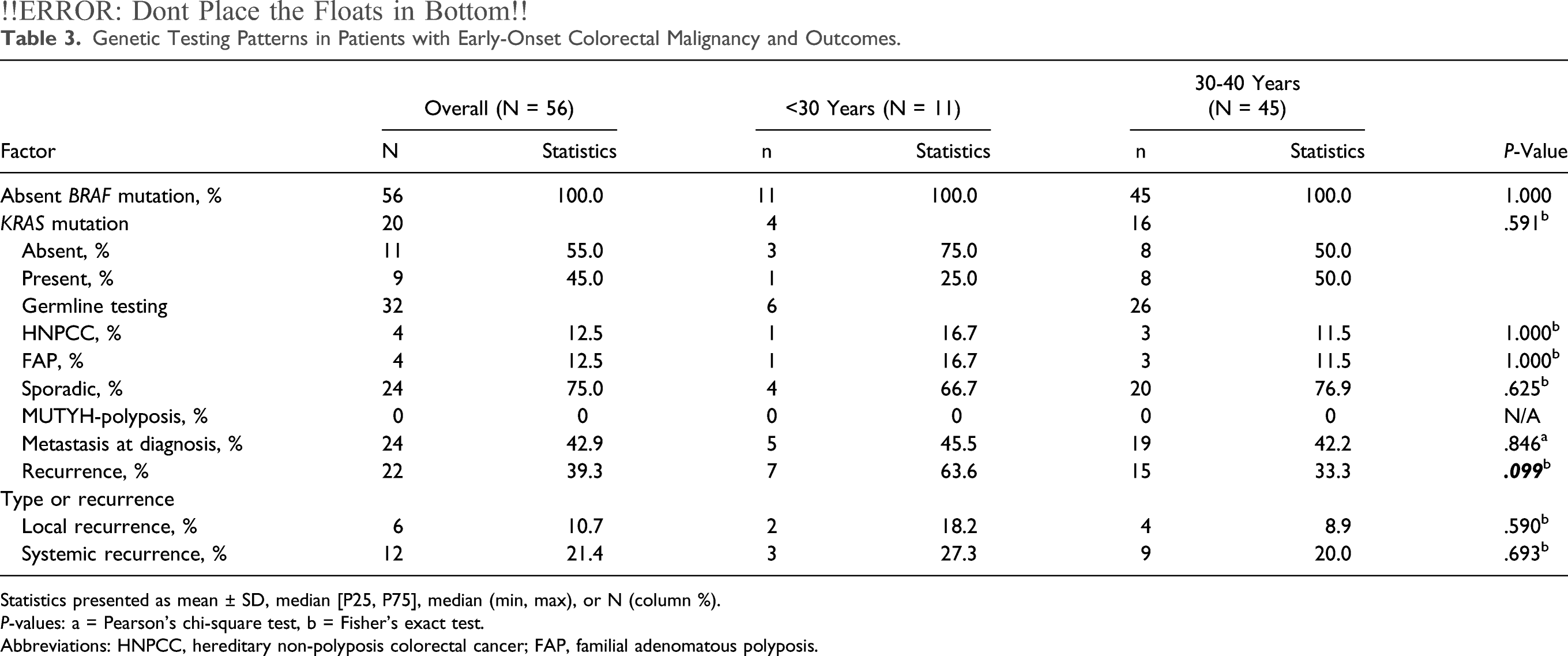
Statistics presented as mean ± SD, median [P25, P75], median (min, max), or N (column %).
P-values: a = Pearson’s chi-square test, b = Fisher’s exact test.
Abbreviations: HNPCC, hereditary non-polyposis colorectal cancer; FAP, familial adenomatous polyposis.
Analysis of Factors Associated to Positive KRAS Mutation.
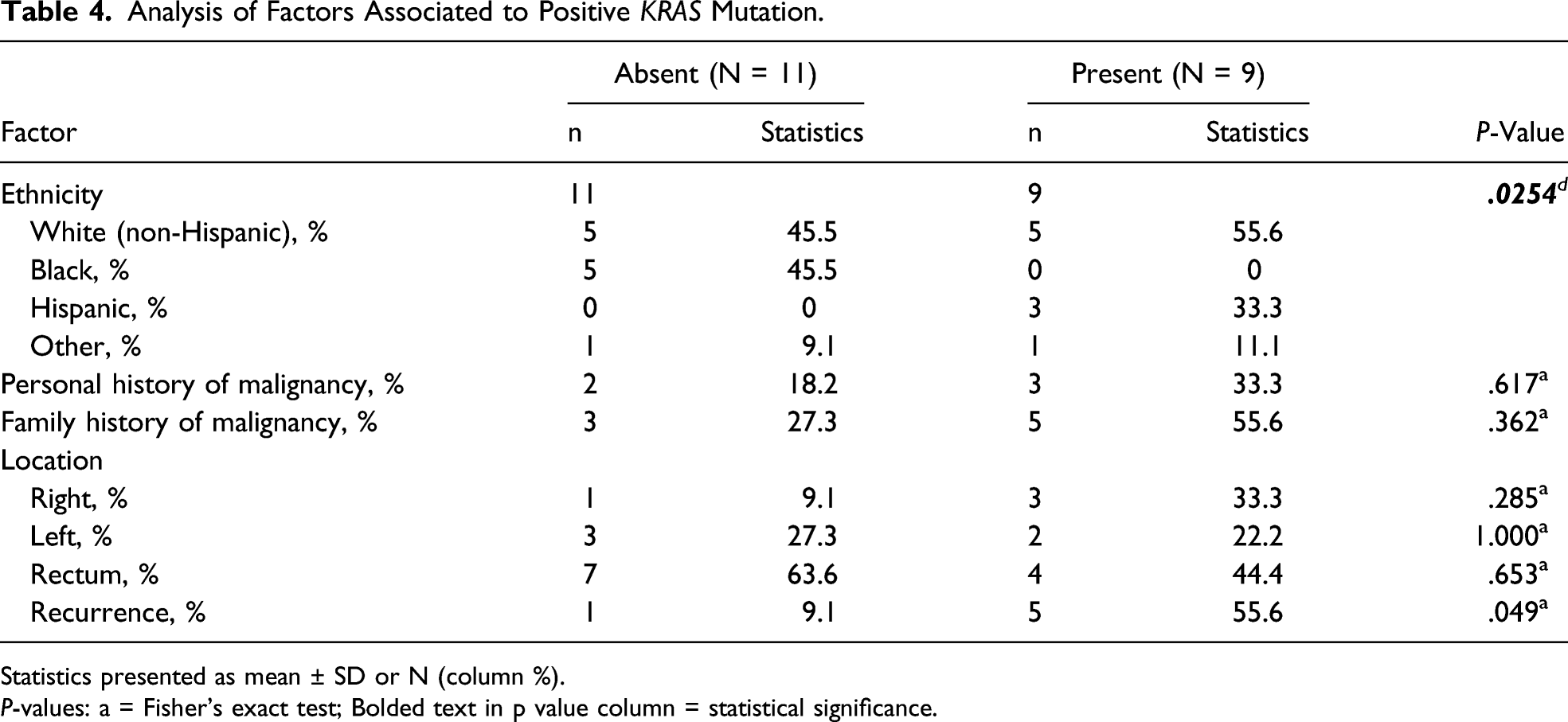
Statistics presented as mean ± SD or N (column %).
P-values: a = Fisher’s exact test; Bolded text in p value column = statistical significance.
Demographic Factors in Sporadic vs Non-Sporadic Colorectal Malignancy.
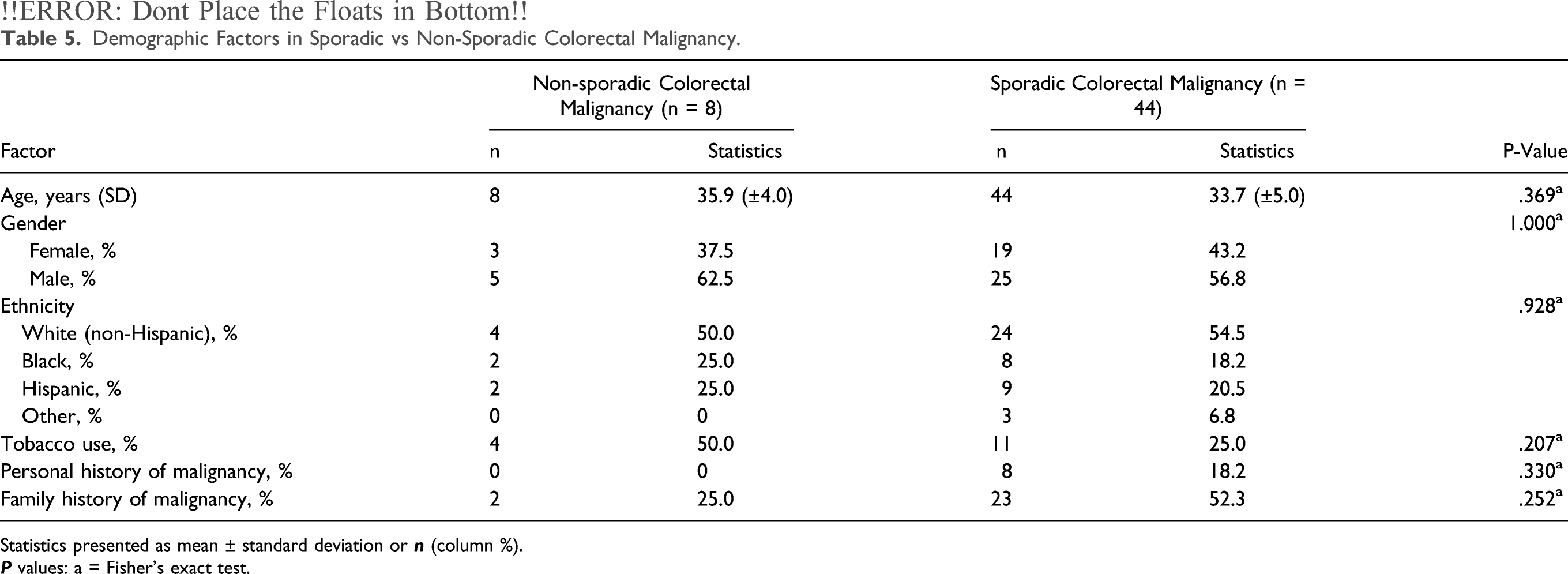
Statistics presented as mean ± standard deviation or
Clinicopathological Characteristics of the Patients with Non-Sporadic vs Sporadic Colorectal Malignancy.
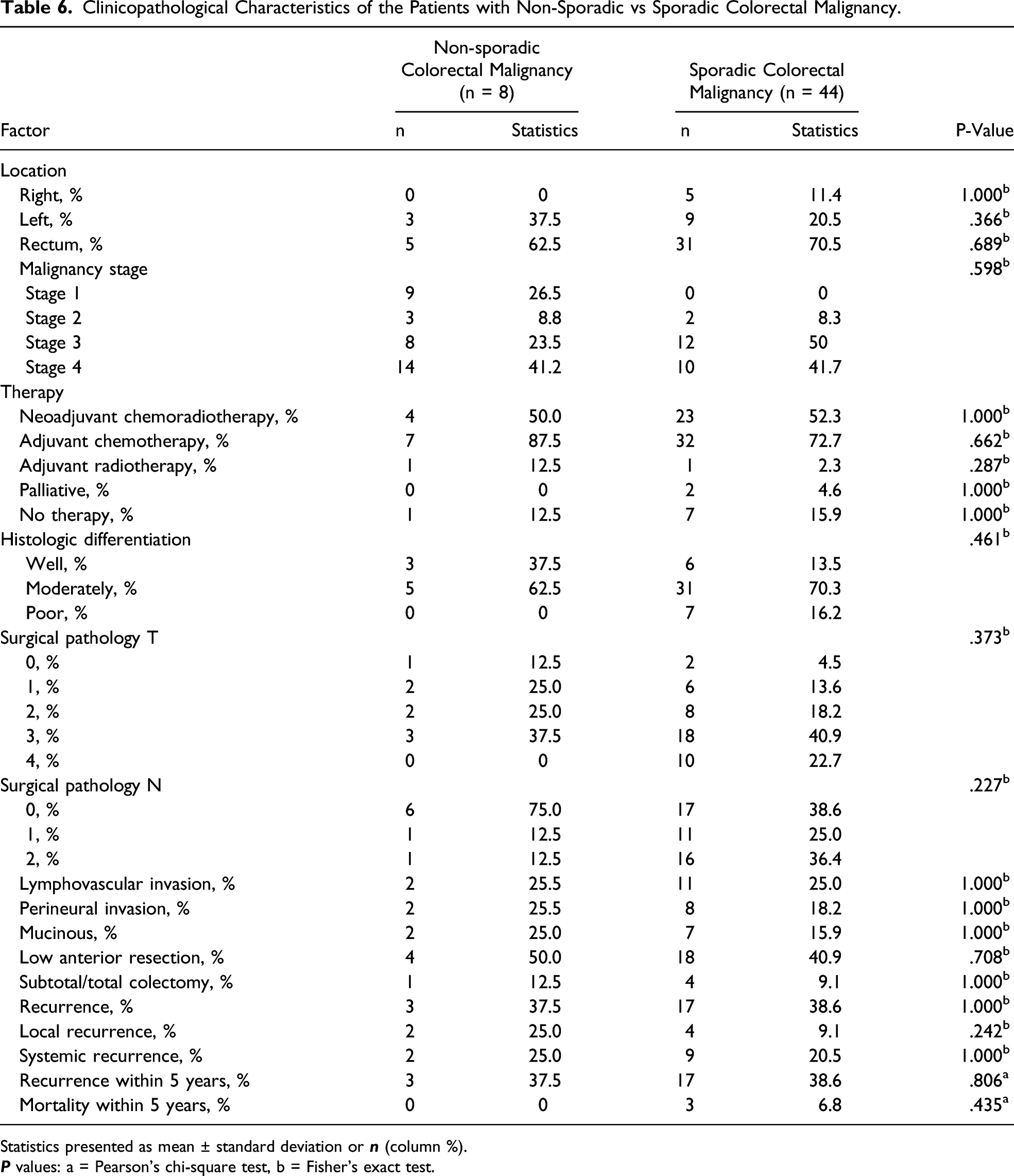
Statistics presented as mean ± standard deviation or
Survival and Disease-Free Interval
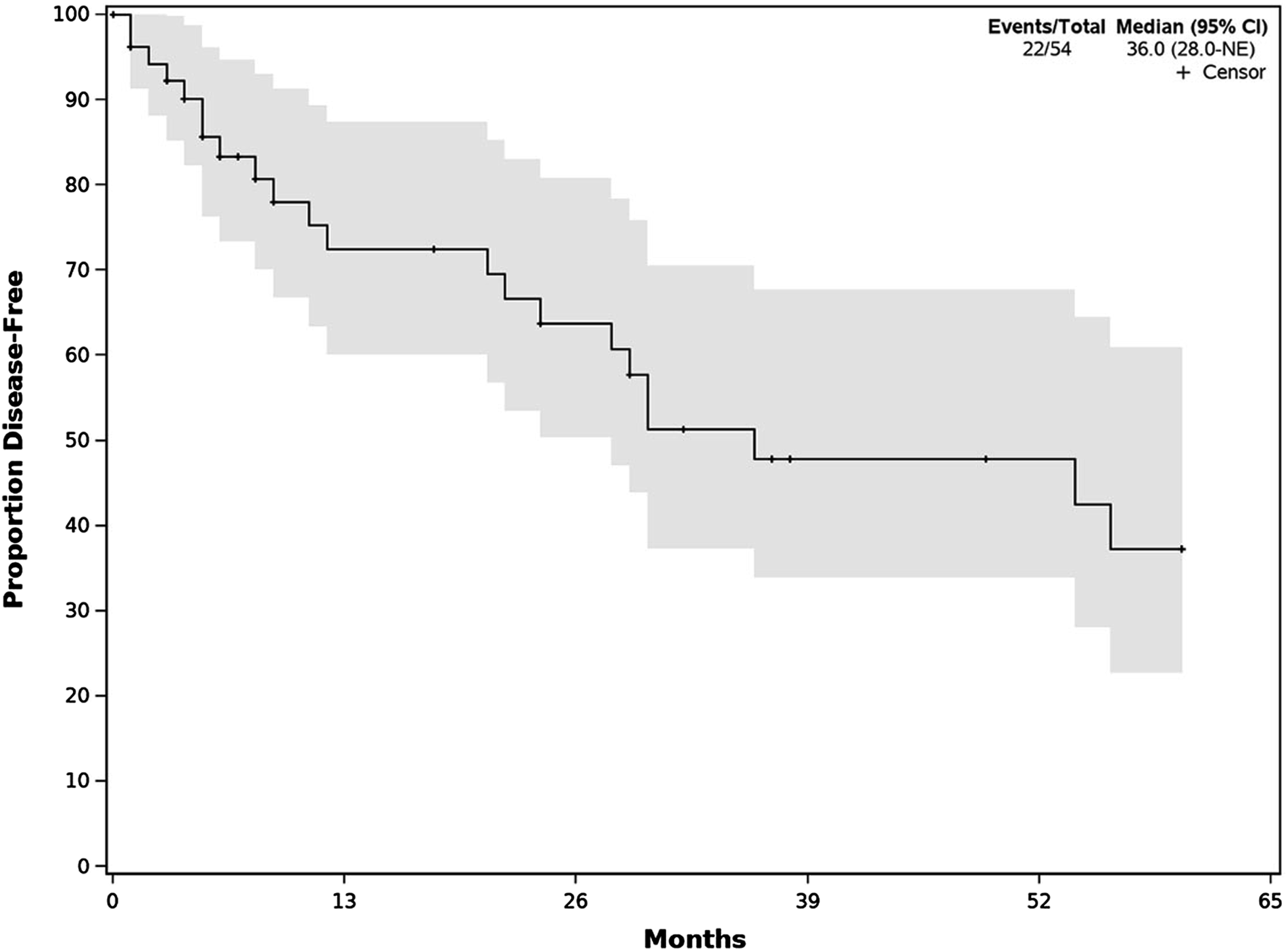
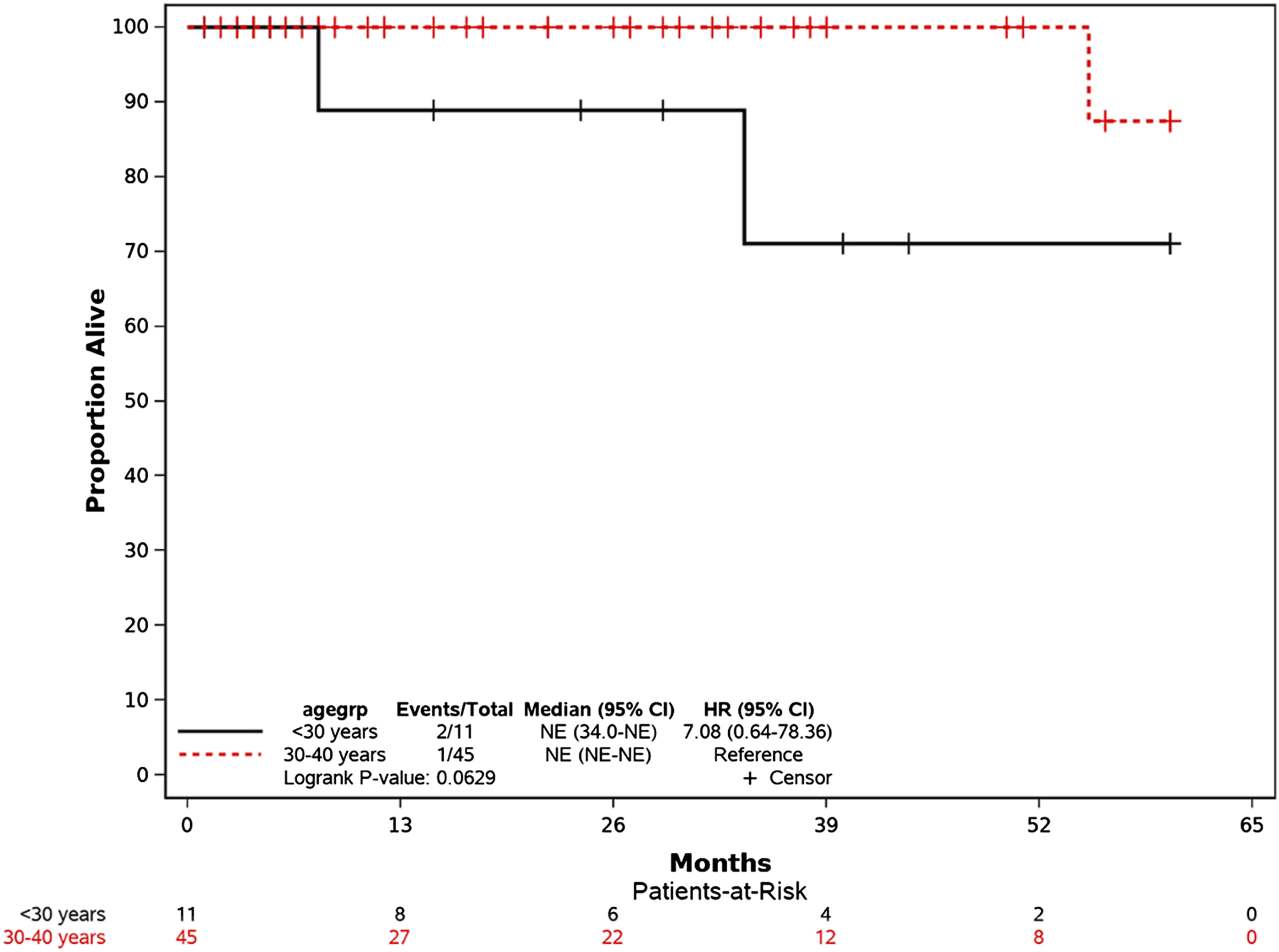
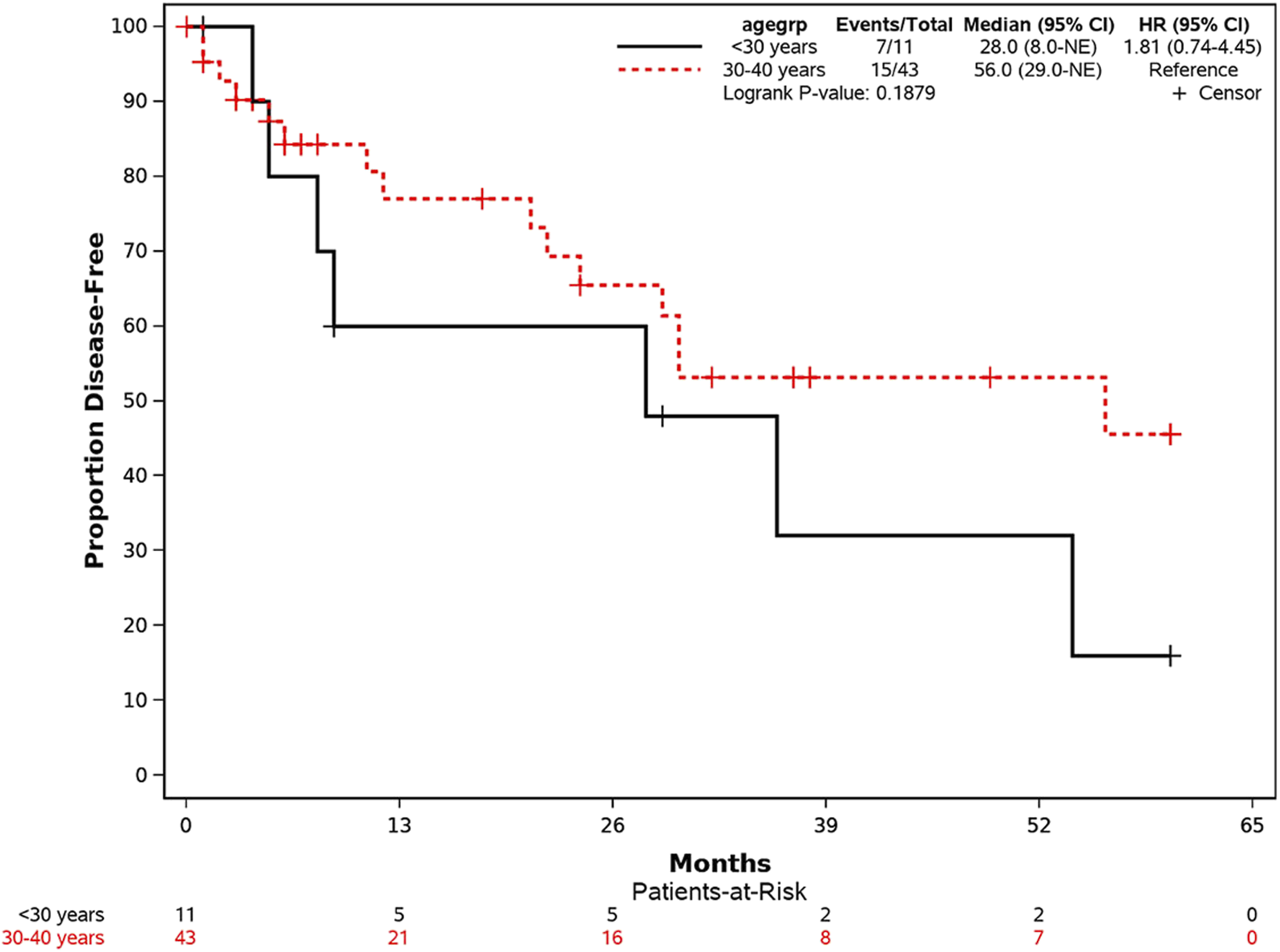
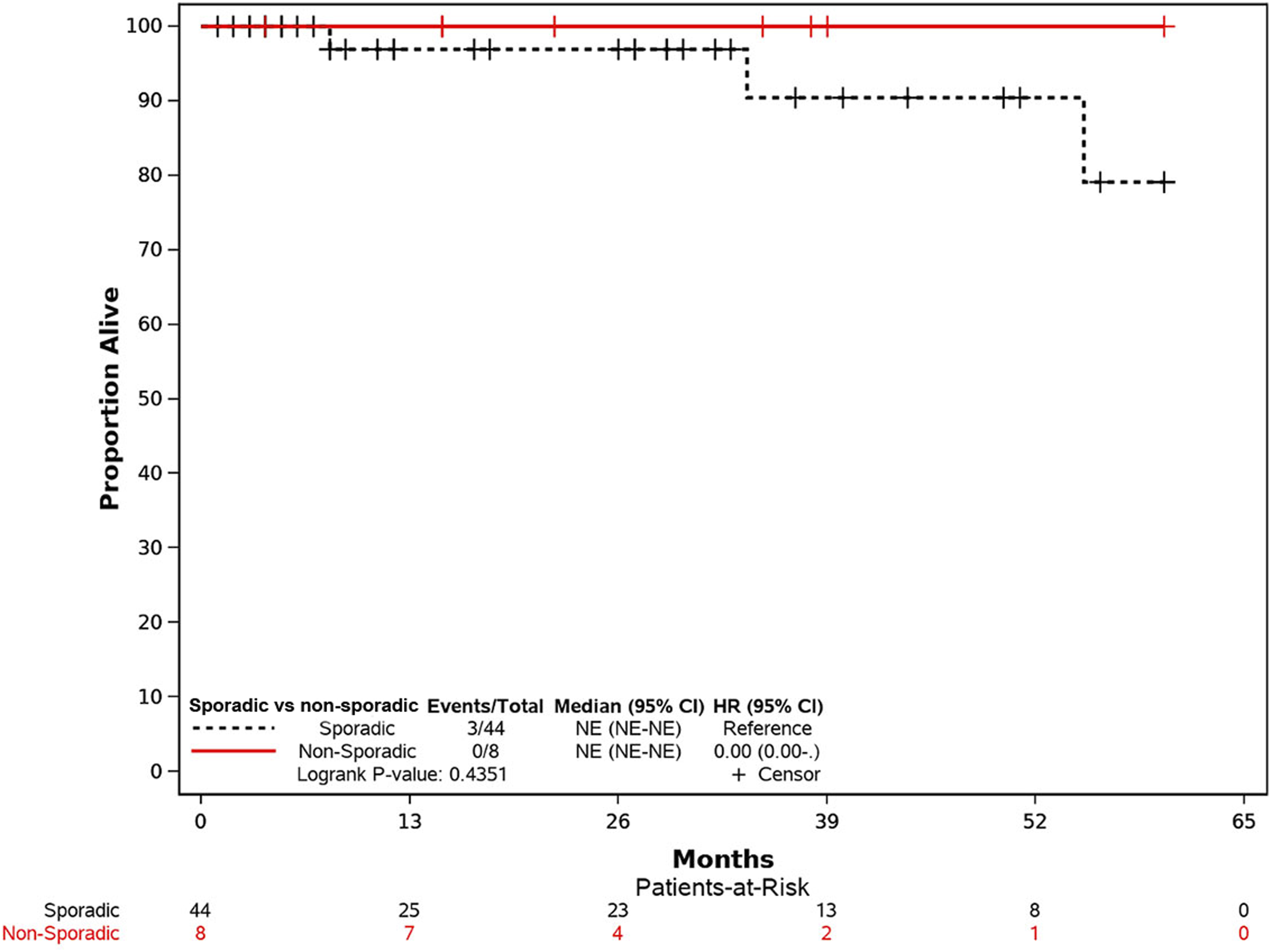
The 5-year OS and DFS rates for all patients were 94.6% and 39.3%, respectively, for patients with adenocarcinoma (Figures 2 and 3). There was a trend toward worse survival (HR 7.08, 95% CI .64-78.36; P = .062) in patients who were <30 years of age compared to patients between 30 and 40 years (Figure 4), but no difference in DFS rate was found (Figure 5). There was no difference in the OS or DFS rate between non-sporadic malignancy and sporadic malignancy (Figures 6 and 7). Overall 5-year survival Kaplan-Meier curve for patients diagnosed with adenocarcinoma. Overall 5-year disease-free survival Kaplan-Meier curve for patients diagnosed with adenocarcinoma. Overall 5-year survival Kaplan-Meier curve by age groups. Overall 5-year disease-free survival Kaplan-Meier curve l curves by age groups. 5-year survival Kaplan-Meier curves comparing sporadic and non-sporadic colorectal malignancies. 5-year disease-free Kaplan-Meier curves comparing sporadic and non-sporadic colorectal malignancies.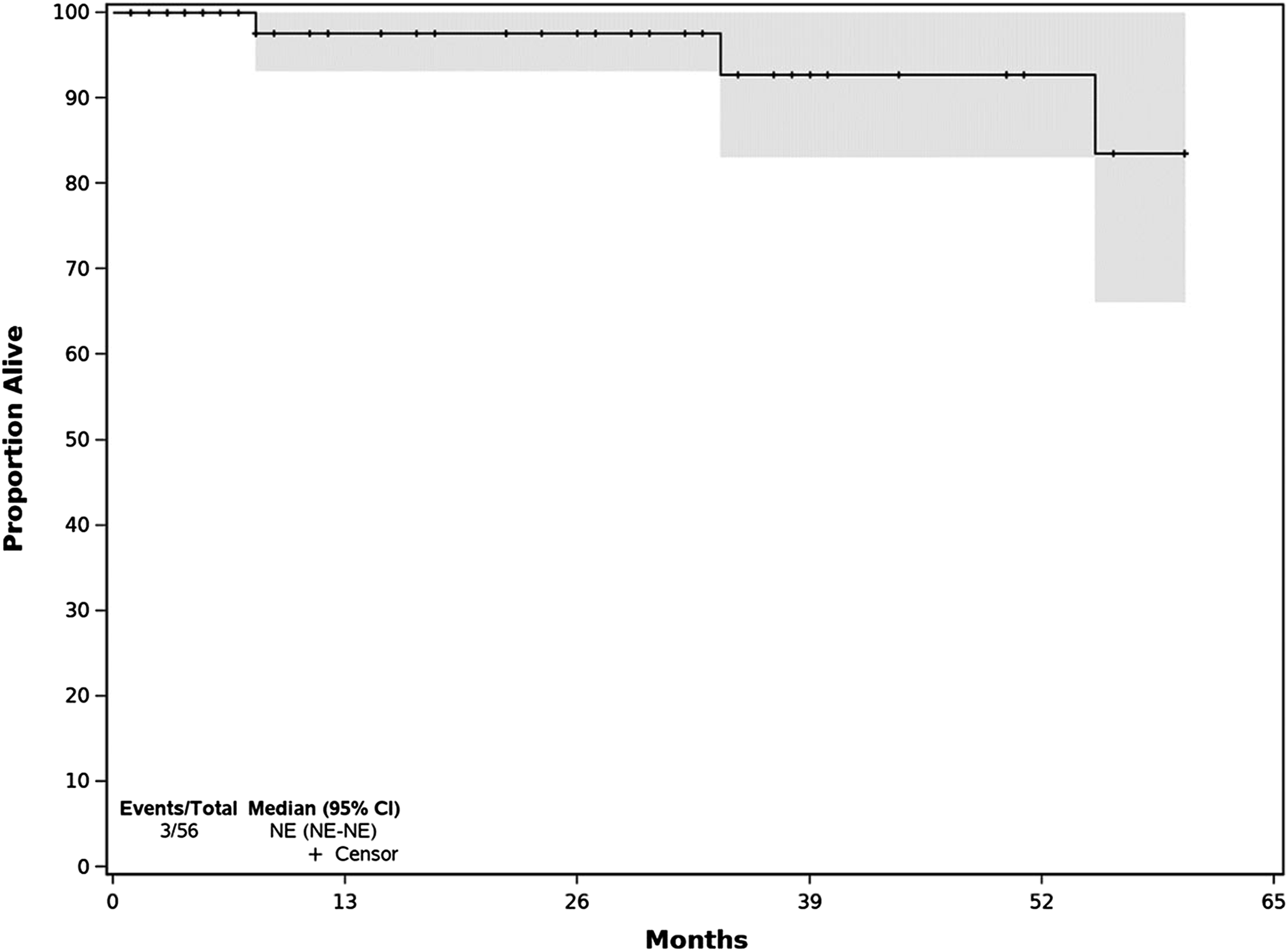
Discussion
Colorectal malignancy has been rising in the young population compared to those patients >50 years of age where there is strong evidence to support that colonoscopy decreases mortality.9,10 We aimed to evaluate the characteristics and outcomes of malignancy in patients ≤40 years of age. Approximately 4% of the total colorectal malignancy population that presented to our institution was ≤40 years of age. Adenocarcinoma was the most common colonic tumor, representing 96.5% of cases. The largest proportion of patients had Stage 4 colorectal cancer (42.9%), while earlier stages were less frequent (12.5% for stage 1 and 8.9% for stage 2). The 5-year OS rate was 94.6% despite having advanced tumor stages at diagnosis. The majority of patients had sporadic malignancy. Approximately 4% of patients were <40 years of age, which falls within the range of early-onset colorectal malignancy (.8-15%) as reported in the retrospective literature. 11
Although many studies have evaluated survival or colorectal malignancy in the young population, not many studies have undertaken a comprehensive analysis of the pathologic, oncologic, and genetic factors that may be contributing to malignancy in patients ≤40 years of age.
Multiple studies compound colon and rectal malignancies on their analysis; however, the more significant change over time in the malignancy location in the young population (<40 years of age) is the distal colon, particularly the rectum.1,12,13 Our study is consistent with these findings as 64.3% of our cohort was found to have rectal cancer, the majority (68.9%) of which were seen in patients between 30 and 40 years of age. The distal location of the malignancy is the reason why 69.9% of our patients presented with gastrointestinal bleeding. Although there are multiple possible benign causes of rectal bleeding in the young population such as hemorrhoids or fissures, physicians need to be aware of early signs of malignancies or advanced adenomas in this population.14,15 Delay in diagnosis is approximately 6 months and may affect disease stage and prognosis. 16
Younger patients <30 years of age were more likely to have recurrent disease and a trend toward worse survival as compared to those 30-40 years of age, likely because of higher percentages of poorly differentiated tumors, lymphovascular invasion, and perineural invasion, which are known high risk factors of recurrence and worse survival. 17 Despite the overall advanced tumor staging (T3-T4) (60.7%) and other aggressive characteristics such as lymphovascular invasion (26.8%), perineural invasion (21.4%), and mucinous type (16.1%) in our young cohort population, the 5-year OS was 94.6%, which is better than previous studies in the 1980s and 1990s in which the 5-year OS ranges from as low as 3% to 60%.18-21 A recent study in colorectal cancer patients <40 years of age showed similar findings with high 5-year mortality despite advanced stages. 22 Young age has been shown to be an independent predictor of better survival likely due to a lack of significant competing comorbidities, less surgical complications, and better tolerability of more aggressive chemotherapy.23-25 Other potential reasons for increased survival over the years include improvement in surgical techniques and chemotherapeutic regimens.26,27
Our study demonstrates that the majority of colorectal malignancies in patients ≤40 years is sporadic (84.6%) and that other genetic predispositions such as Lynch syndrome or FAP are less common. Although patients <30 years of age were more likely to have a hereditary malignancy, this difference was not significant. This finding is consistent with other studies in which sporadic malignancies were the most common in this young population.28,29 Patients with sporadic malignancy had more advanced stages of disease compared to those with non-sporadic malignancy. It is possible that this difference is due to the fact that patients with non-sporadic malignancies had early colonoscopies as there are well established screening guidelines for people with affected family members with hereditary colon malignancy. 30
Adjuvant chemotherapy was more frequently used in patients with sporadic malignancy as compared to non-sporadic malignancy likely because they were at more advanced stages of disease. The survival between the two groups was similar despite some studies stating that adjuvant chemotherapy after radiation and surgery for rectal cancer does not improve survival. 31
There are multiple limitations to our study given the retrospective nature of our data review. Many patients were referrals to our institution and information regarding genetic testing may not have been available at the time of data collection. In addition, survival rates could have been affected as many patients continue oncologic evaluation at outside institutions and had loss of long-term follow-up at our institution. Furthermore, the sample included in our study is relatively small, which why none of the African American patients had KRAS mutation. However, we believe our results are consistent with more recent survival rates in young patients with colorectal malignancies. Finally, it is important to mention that, in young patients, the standard 5-year follow-up may not be long enough to determine the long-term recurrence or mortality rates in young patients. Further studies with longer follow-up are warranted to explore this area.
Conclusions
Although the incidence of colorectal malignancies in the young population ≤40 years of age is increasing compared to those >50 years of age, the relative incidence is still low. However, given this increasing incidence, malignancies should be considered in this patient population. This study adds to the body of evidence that despite the aggressive nature of colorectal malignancies in patients ≤40 years of age, patients have good 5-year survival at approximately 94.6% at 5 years. It also highlights the fact that consideration for genetic counseling and testing may be indicated as a mutation may be found in >25% of patients and this has clinical implications for first degree relatives of affected individuals.
Footnotes
Acknowledgments
Hong Liang, PhD for all statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.