
Abstract
Introduction
Stop the Bleed (STB) is a national training program aiming to decrease the mortality associated with life-threatening bleeding due to injury. The purpose of this study was to evaluate the efficacy and confidence level of security personnel placing a tourniquet (TQ) compared to civilians.
Methods
Pre and post questionnaires were shared with security personnel (Group 1) and civilians (Group 2). Both groups were assessed to determine comfort level with TQ placement. Time and success rate for placement was recorded pre- and post-STB training. A generalized linear mixed model or generalized estimating equations was used to compare pre and post measurements.
Results
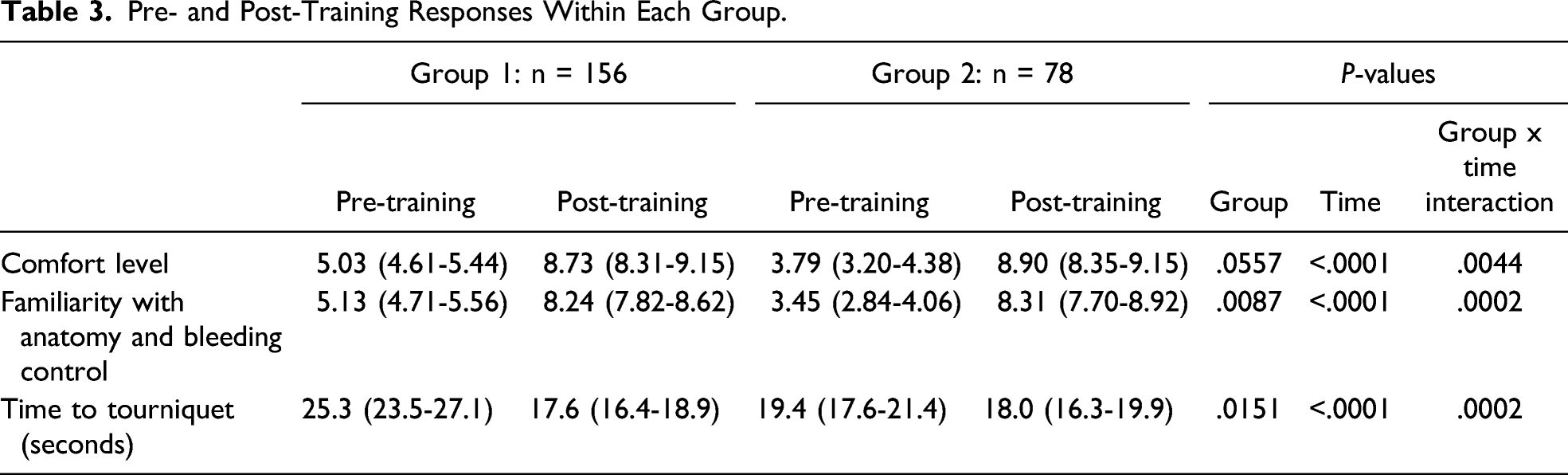
There were 234 subjects enrolled. There was a statistically significant improvement between the pre- and post-training responses in both groups with respect to comfort level in placing a TQ. Participants also demonstrated increased familiarity with the anatomy and bleeding control after STB training. A higher successful TQ placement was obtained in both groups after STB training (Pre-training: Group 1 [17.4%], Group 2 [12.8%]; Post-training: Group 1 [94.8%], Group 2 [92.3%]). Both groups demonstrated improved time to TA placement with a longer mean time improvement achieved in Group 1. Although the time to TQ placement pre-and post-training was statistically significant, we found that the post-training times between Groups 1 and 2 were similar (P = .983).
Conclusions
Participants improved their confidence level with the use of hemorrhage control techniques and dramatically increased the rate and time to successful placement of a TQ. While civilians had the greatest increase in comfort level, the security personnel group saw the most significant reduction in the time to successful TQ placement. These findings highlight the critical role of STB in educating and empowering both civilians and security personnel in bleeding control techniques.
Introduction
The number of mass shootings has averaged about 20 per year since the 1970s in the USA. 1 The Sandy Hook Elementary School shooting in Newton, Connecticut in 2012 was the catalyst for the Hartford Consensus and the Stop the Bleed (STB) program that teaches bystanders to be an active participant in victim survival. In April of 2013, a group of officials met to develop methods to “increase strategies to increase survivability in mass casualty shootings.” 2 The STB program was launched by the American College of Surgeons with White House and Federal agencies collaboration, merging the lessons of our military experience and tenets of the Hartford Consensus.
In a previous study, 3 our group reported on the performance of law enforcement officers and private security personnel (combined hereafter referred to as “Security Group”) with STB training. Private security personnel are often retired or active law enforcement officers and have an expectation of some knowledge of tourniquets (TQs). We wanted to understand if similar benefits would be seen in the civilian population and how this compared to our prior study group. Therefore, the purpose of this new study was to evaluate the efficacy and confidence level of the Security Group as compared to civilians (Civilian Group) in placing a TQ. We hypothesized that STB training would improve performance in successfully placing TQs in both groups and with superior performance of the Security Group.
Methods
Study Design and Participants
We obtained approval from the Institutional Review Board at NYU Langone Hospital—Long Island. Volunteers who attended our Stop the Bleed courses were invited to participate in the study. All agreed, signed informed consent, and were admitted to the study. We provided a pre- and post-evaluation questionnaire of our STB educational program that included civilian population working for secondary schools and commercial businesses from surrounding communities on Long Island, New York. Participants in STB trainings were educated per the American College of Surgeons (ACS) guidelines, using appropriately certified and registered instructors.
Each class consisted of two parts: (1) a lecture component using the ACS-developed STB presentation, and (2) simulation stations offering trainees the opportunity to practice holding pressure and packing wounds using inanimate models and applying combat application tourniquets (CAT) to their partner’s arms. Participants were evaluated by direct observation of performance and self-assessment of the learning experience. In order to compare both groups, the questionnaire and the study modality were the same used in our previous study. 3
Observation of Performance
To evaluate the correctness of TQ application and time required for placement, a member of the research team observed the participant apply the TQ just before the start of the course and again immediately after the lecture and the simulation. Participants were observed for correctness of placement (yes/no) and for time to correct placement in minutes. The observers use “not on joint” and “loss of a pulse” as the determinants of correct TQ placement. Study subjects were directed to use their arm and/or their partner’s arm to place a TQ. Having previously been trained in TQ placement, all research associates were comfortable with the correct placement of the TQ. The research team was able to assess correct placement using visualization and the loss of a strong palpable pulse. They also confirmed that TQ location was appropriate and not overlying a joint.
Self-Assessment
Participants completed anonymous pre- and post-training questionnaires that used Likert scales to assess their knowledge and comfort level with use of TQs. The questionnaire contains ten questions, four at the pre-training and six at the post-training phases (Appendix). Questions such as how comfortable they were using TQs for hemorrhage control and how familiar they were with the anatomy as it applied to the basics of bleeding control were asked and answered. The Likert scales ranged from 1- not comfortable/familiar at all, to 10-very comfortable/familiar, no questions or concerns. The post-training questionnaire contained two extra questions that used similar Likert scales: “How much did an explanation of the anatomy by a surgeon or other qualified physician help your understanding and comfort level with applying the tourniquet?” and “Would ongoing interaction, teaching, and availability by qualified surgeons make you feel more secure and safe in your job?” All study subjects completed all questionnaires.
After completion of the prospective evaluation of the TQ application in the civilian population cohort, a comparison of the Security Group (Group 1) versus the Civilian Group (Group 2) was performed.
Statistical Analysis
Separate Generalized Linear Mixed Models (GLMM) were used for the analysis of “Time to tourniquet application,” “How comfortable are you with the tourniquet (scale of 1-10),” and “How familiar are you with anatomy and bleeding control (scale of 1-10)” comparing the two groups pre- and post-training. The standard assumptions of Gaussian residuals and quality of variance were tested using the Shapiro-Wilk test. Since the standard assumptions were not met for Time to TQ application, a natural logarithm transformation was performed. The results were brought back to the original units and reported as geometric means with their corresponding lower and upper confidence limits. Generalized Estimating Equation (GEE) was used as a method of parameter estimation for the correlated binary data for the question “Was the tourniquet applied correctly” (Yes/No). Group (Security Group vs Civilian Group), time (pre vs post), and the group x time interaction were included in all models described above. A result was considered statistically significant at the P < .05 level of significance. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Pre-Training Responses in Both Groups.

Post-Training Responses in Both Rroups.

Pre- and Post-Training Responses Within Each Group.
Discussion
Mass casualty incidents have necessitated education of the public on survival techniques. The main goal of the STB course is the prevention of death due to controllable hemorrhage. 4 Three key concepts are at the foundation of achieving this goal: First, a new category of responder—the “immediate responder” was put forth. This is a citizen trained to render aid as soon as it was safe to do so. The second concept, victims needed to be evacuated to definitive care as soon as possible via cooperation between emergency medical system (EMS) personnel and law enforcement. Third, ensure police and other law enforcement and first responders are trained in the use of wound packing and TQs. 4
Ünlü and associates 5 evaluated combat TQ application times and application success rates in 102 participants during three different stages: basic, after-training, and blindfold phases. This study focused on the effect of training and repeated self-CAT applications on effectiveness rates. Brief training increased TQ success rates from 84% to 92% in the upper limb and 55.8% to 73.8% in the lower limb. Recognition of and interventions for bleeding injuries are enormously difficult in the low-light combat environment and under light discipline. In this study, training only involved a daylight environment but in the blindfolded phase, the upper and lower extremity success rates increased to 96% and 87% for upper and lower extremities, respectively. Moreover, the introduction of the ability to decrease blood flow is an important concept that may be unknown to the average citizen so that there would be an expected impact even in the absence of light.
In a study performed by Clasper et al 6 on UK Armed Forces members who sustained severe life-threatening limb injuries in Iraq and Afghanistan, they compared the presence or absence of pre-hospital TQ application. The authors reported a significant difference in the incidence of major complications, mainly due to deep tissue infection. They suggested that although the use of pre-hospital TQ was a factor, the method of fixation, implant, and timing of wound closure also played a role.
Teixeira et al 7 reported that civilian prehospital TQ application was independently associated with a 6-fold mortality reduction in patients with traumatic peripheral vascular injury. Multiple studies have confirmed the benefits of TQs in extremity wounds in the civilian setting. They highlight the importance of educating the public on the correct application of TQs and other hemorrhage control measures.8-11 In 2013, after the Boston Marathon bombing, it was reported that while TQs were applied in 83.9% of exsanguinating extremity injuries, many were not properly applied or were poorly improvised. 12 Although the willingness of first responders and spectators alike to administer first aid, several makeshift field TQs such as belts and other articles of clothing were not properly applied and as such did not control bleeding. 13
In a study performed by Schroll et al, 14 which included the training of 1974 lay rescuers to identify and control life-threatening bleeding, they were able to demonstrate a significantly increased knowledge of bleeding control techniques and confidence in their skills after completing a 1-h STB course and able to demonstrate proficiency in performing bleeding control skills.
We sought to empower the civilian population as we did with law enforcement officers and private security personnel previously 3 and to demonstrate the utility and validity of the STB course. In our study, while there was not a significant difference in the rate of “Apply Correctly” between the both groups across time (P < .9517), there was a statistically significant increase in both groups, respectively. In the Group 1 (P < .0001) and the Group 2 (P < .0001) rates of “Apply Correctly” did increase from the pre-to the post-assessment. Therefore, by obtaining correct placement of the TQ with statistically significant improvement after the STB course session, we have demonstrated the importance of the STB course in both groups. It is clear from our study that courses such as STB not only teach important skills but also increase comfort level with application of this life-saving skill.
Although there are reports 15 emphasizing the costs involved in this type of hands-on course and prioritization of the target audience, programs such as STB seeking to bring basic knowledge to civilians with minimal training are becoming mainstream. Basic easily-deployable knowledge to civilians has been successfully demonstrated by both the widespread deployment of AEDs and use of CPR. 16 The Federal Emergency Management Agency (FEMA) has recently launched the Until Help Arrives campaign in an effort to encourage bystanders to immediately help injured individuals in the field. 17
STB training publications are common in the literature but mainly examining civilians. Our study contributes to the existing literature differently as it actually compares the outcomes between groups comprised of law enforcement and private security personnel versus the civilian population. Training of both groups carry a benefit as an incident of mass shooting can happen anywhere at any time. We believe that this type of training should incorporate as many and as varied trainees as possible.
Our study has several limitations. The study groups were small and we did not assess for familiarity with TQ placement at the start. However, allowing study participants to use the TQ before and assessing the placement addressed this limitation. Some participants were allowed to practice for two to three attempts after the didactic and hands-on training session and prior to taking the post-test. While this could have introduced a feature of variability, the idea was to create a non-threatening and calm learning environment. Study design did not involve the effect of pain perception in the participants. While this could be a limiting factor, the focus was on the absence of a palpable pulse as an endpoint. As other articles published on the same topic, we were unable to provide data regarding cost of training. Lastly, we had hoped to increase the number of participants in the study, but the onset of the COVID pandemic in 2020 was prohibitive.
Conclusions
After Stop the Bleed training, participants improved their confidence level in the use of hemorrhage control techniques and dramatically increased the rate and time to successful placement of a tourniquet. While civilians had the greatest increase in comfort level, security personnel saw the most significant reduction in the time to successful placement. These findings highlight the critical role of Stop the Bleed in educating and empowering both civilians and security personnel in bleeding control techniques and should encourage both groups to obtain this potentially life-saving training. Future initiatives should include distribution of bleeding control kits, and evaluating the possibility of participants’ recertification and continued retention of knowledge and skills over time.
Supplemental Material
Supplemental Material - Stop the Bleed: A Prospective Evaluation and Comparison of Tourniquet Application in Security Personnel Versus Civilian Population
Supplemental Material for Stop the Bleed: A Prospective Evaluation and Comparison of Tourniquet Application in Security Personnel Versus Civilian Population by Patrizio Petrone, Gerard Baltazar, Ricardo A. Jacquez, Meredith Akerman, Collin E. M. Brathwaite, and D’Andrea K. Joseph in The American Surgeon
Footnotes
Acknowledgment
Ellen Berghorn, RN; Maureen Casey, RN; Sofía Espinoza, MD. NYU Langone Hospital—Long Island, Mineola, New York.
Author’s Note
Podium presentation at the 2021 Clinical Congress of the American College of Surgeons.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.