
Abstract
Background
Multiple socioeconomic and clinical factors have been implicated in the health disparities that exist amongst vulnerable populations with colorectal cancer. Efforts have been directed toward addressing these factors to improve outcomes. We evaluate the impact of primary care physicians (PCP) on the surgical presentation and outcomes of colorectal cancer at a safety-net hospital.
Methods
A retrospective chart review of 331 patients diagnosed with colorectal adenocarcinoma between 2014 and 2020 at a single-institution urban county medical center.
Results
The cohort was predominantly male (59%) and Hispanic (52.1%). Thirty-two percent of patients had a PCP at time of diagnosis. Patients with PCPs compared to those without PCPs had significantly lower rates of acute presentation (perforation or obstruction) (17.0 vs 38.1%, P < .001), higher rates of surgical resection (83.0 vs 70.7%, P = .016), and were less likely to have metastatic disease at presentation (20.4 vs 33.5%, P = .02). Overall, having a PCP also improved probability of survival (HR 1.36, P < .04).
Conclusion
Having a PCP at the time of colorectal cancer diagnosis is associated with improved outcomes in a safety-net population, with significant differences in surgical presentation and resection.
Key Takeaways
• Patients with primary care physicians (PCPs) compared to those without PCPs had significantly lower rates of emergency presentation and higher rates of resection of primary tumor for colorectal cancer • Patients with PCPs had improved probability of overall survival compared to those without PCPs
Introduction
Colorectal cancer remains one of the leading causes of cancer-related mortality in the United States, accounting for 8.7% of all cancer deaths in 2021. 1 Poorer outcomes for colorectal cancer disproportionately affect vulnerable populations, who face multiple barriers along the entire continuum of care, from diagnosis through treatment. Well known identified barriers include lack of insurance or access to health care, inadequate access to bowel preparation, and decreased health literacy, among others.2,3 Patients who are treated at safety-net hospitals often present with advanced stages of colorectal cancer which limit or eliminate surgical treatment options, leading to higher rates of mortality.4,5 The implementation of the Affordable Care Act (ACA) was designed to eliminate cost sharing for screening and to facilitate insurance coverage for these patients and has indeed had some success in improving outcomes. 6 However, the effect on colorectal cancer screening and survival has been modest at best, and gaps still exist that need to be identified. 7
One of these gaps may be the establishment of a primary care physician (PCP) for these patients. Despite increased insurance coverage, many patients continue to seek care only as needed or from the emergency department. However, PCPs are ideally situated to address many barriers to care, including facilitating screening and ensuring follow up to results. The objective of this study was to determine if the presence of a PCP at the time of colorectal cancer diagnosis was associated with improved outcomes in a safety-net hospital patient population and to examine the impact on surgical presentation of disease.
Methods
Study Design
Following exemption from the Institutional Review Board at Harbor-UCLA Medical Center, patients diagnosed with colorectal adenocarcinoma between 2014 and 2020 were identified by International Classification of Diseases (ICD)-10 codes (C18-C20). Adult patients with an isolated diagnosis of colorectal adenocarcinoma were included. Patients were excluded if an incorrect malignancy instead of colorectal adenocarcinoma was coded into the electronic medical record erroneously, if there was insufficient follow up, or if the diagnosis could not be confirmed by chart review.
Data were collected on patient demographics (sex, age, ethnicity), presence of a primary care physician at time of diagnosis, pathology reports (histopathologic findings, tumor biology), clinical stage at diagnosis and pathologic stage at time of surgery, as well as vital status.
Outcomes
The primary outcome was overall survival. Secondary outcomes included rates of emergency presentation, stage at diagnosis, and time to planned surgical and systemic therapies. Emergency presentation was defined as patients who first presented to the hospital with intestinal obstruction or perforation secondary to colorectal cancer requiring surgical intervention. In the statistical analysis of time to planned surgery, patients who presented needing emergency surgery were omitted. Cancer staging was based on the American Joint Committee on Cancer (AJCC) eighth edition classification system. Stage I and II malignancies were defined as local, Stage III as locally advanced, and Stage IV as metastatic.
Statistical Analysis
Continuous variables are shown as means with standard deviations and were analyzed using independent student’s t tests. Categorical variables are shown as percentages and were analyzed using Chi-squared tests. Bivariate analysis using Kaplan–Meier survival curve was used to assess long-term survival. Statistical significance was defined as P-value <.05. All statistical analysis was performed using SAS 9.4.
Results
Demographics Of Patients Diagnosed With Colorectal Cancer.
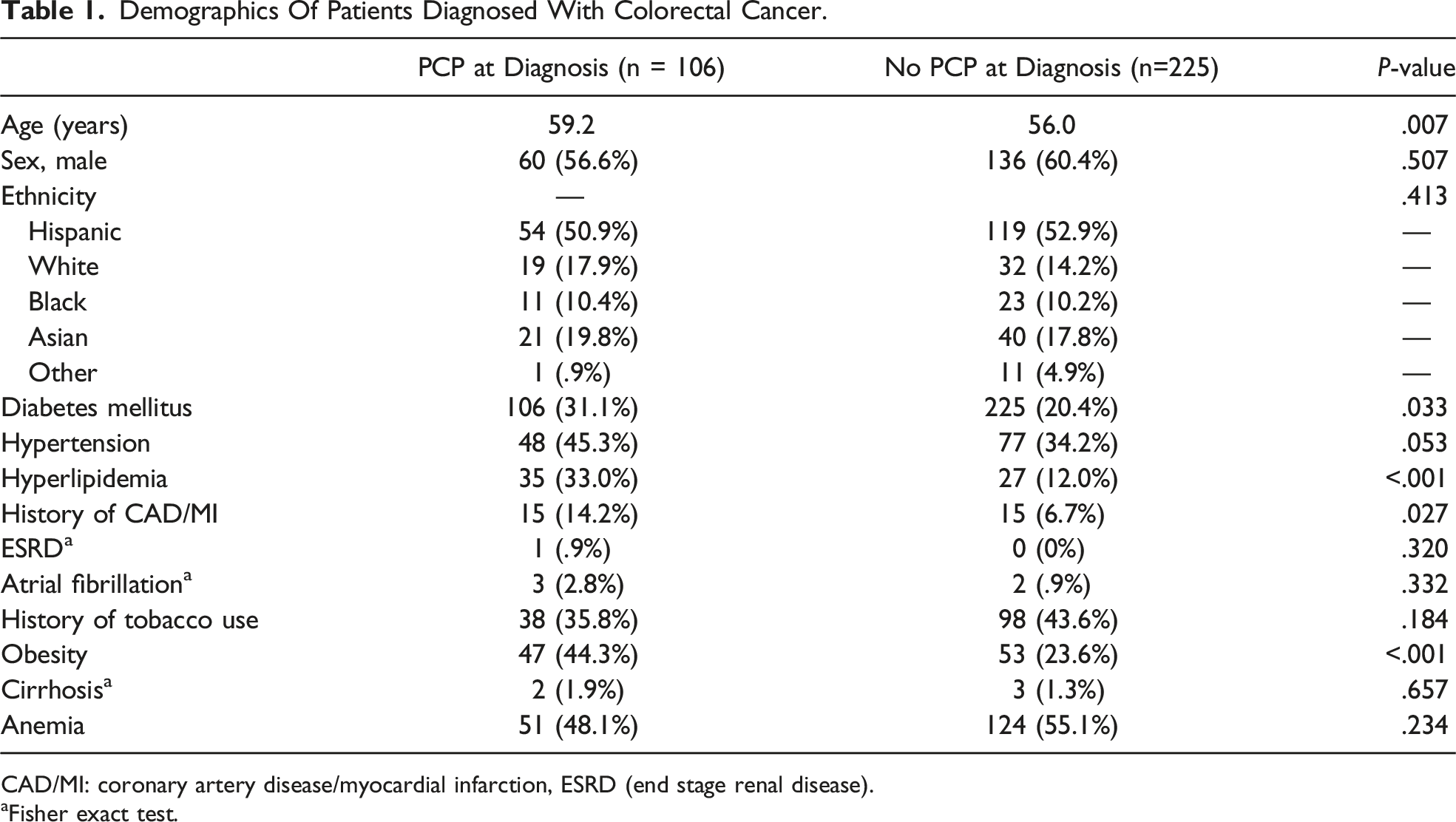
CAD/MI: coronary artery disease/myocardial infarction, ESRD (end stage renal disease).
aFisher exact test.
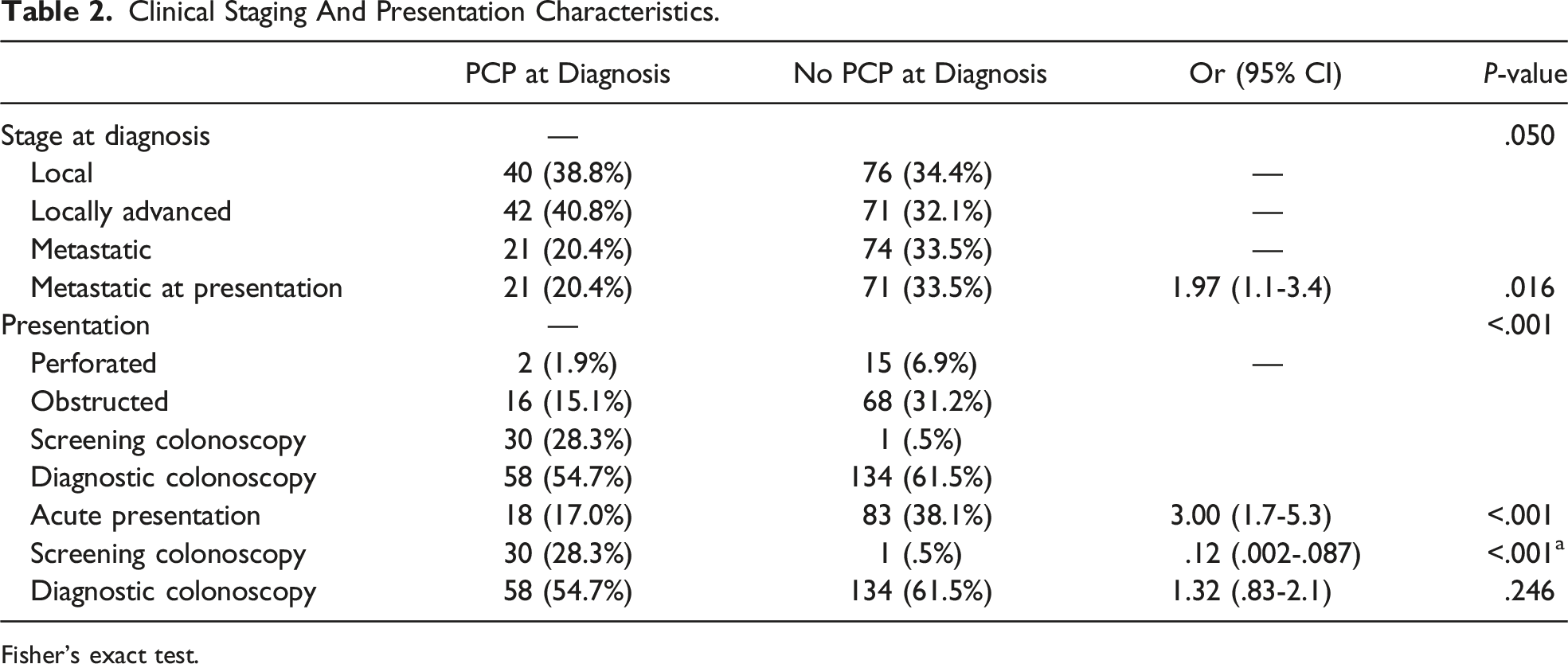
Patients with a PCP at the time of cancer diagnosis had an improved probability of overall survival with a hazard ratio of 1.36, P = .04 on bivariate analysis (Figure 1). Overall, patients with a PCP had lower rates of emergency presentation, 17.0% vs 38.1% (OR 3.00, 95% CI: 1.7-5.3, P < .001). Intestinal obstruction was the more common cause of emergency presentation in both groups 15.1% vs 31.2%. Patients with a PCP also had higher rates of surgical resection (83.0 vs 70.7%, P = .016) and lower rates of metastatic disease at presentation, 20.4 vs 33.5% (OR 1.97, 95% CI: 1.1-3.4, P = .016) (Table 2). Patients with PCPs were more likely to have undergone screening colonoscopy (28.3% vs .5%, P < .001) as a method of diagnosis. The rates of diagnostic colonoscopy for either a positive fecal immunochemical test or symptoms were the same between groups. Overall survival for patients with a PCP at time of cancer diagnosis (red) vs patients without a PCP at time of cancer diagnosis (blue). Clinical Staging And Presentation Characteristics. Fisher’s exact test.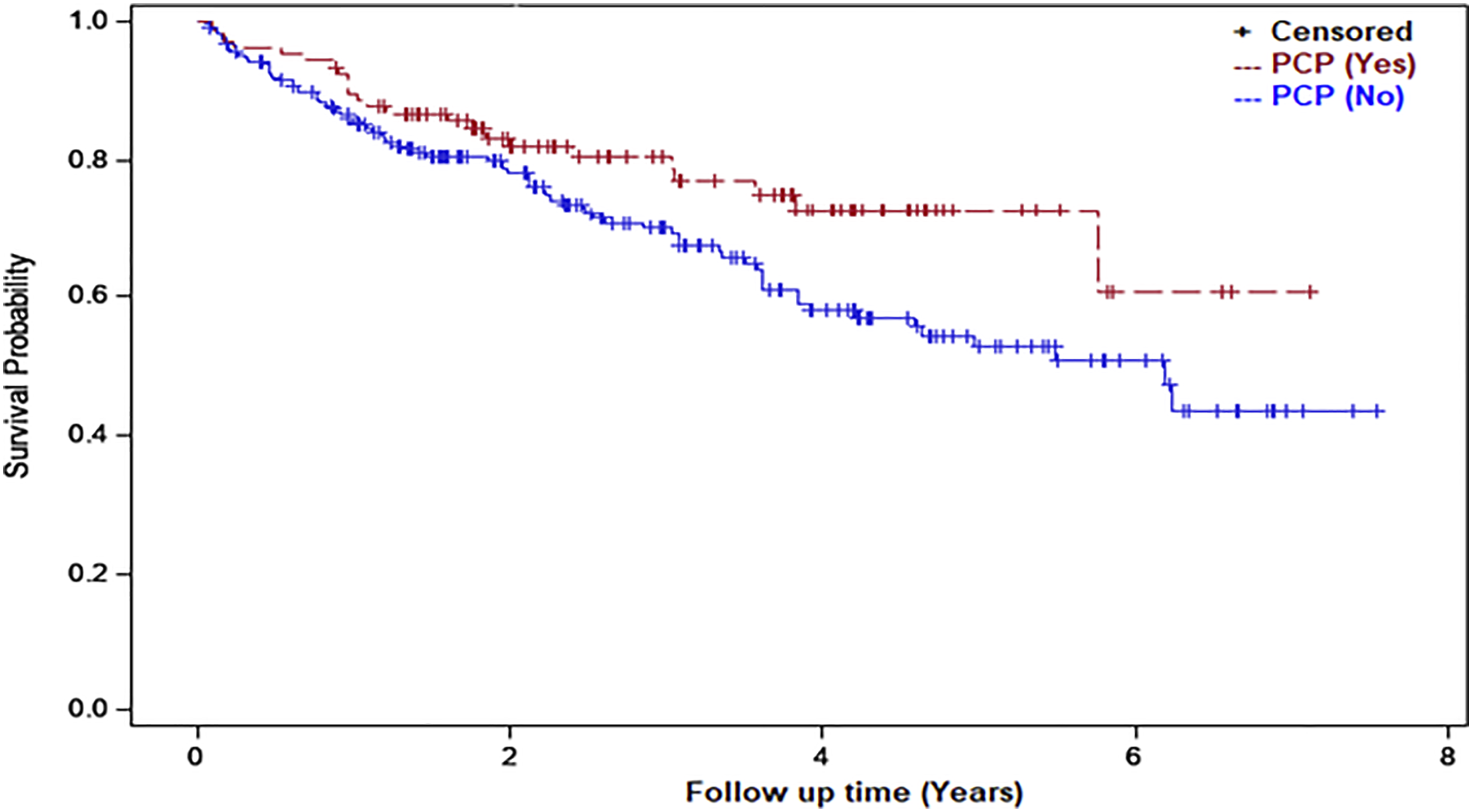
At the time of cancer diagnosis, patients with a PCP had higher rates of diabetes mellitus, hyperlipidemia, and coronary artery disease when compared to patients without a PCP, 31.1 vs 20.4% (P = .033), 33.0 vs 12.0% (P < .001), and 14.2% vs 6.7% (P = .027), respectively. History of tobacco use was more common in patients without a PCP and obesity was more common in patients with a PCP. Rates of chronic obstructive pulmonary disease, end stage renal disease, atrial fibrillation, and cirrhosis were low and not significantly different between the two groups.
Patients in both groups presented with similar tumor biology with no significant differences seen in microsatellite instability (MSI), KRAS positivity, NRAS positivity, or BRAF positivity. There was also no difference between groups with regards to lymphovascular or perineural invasion on final pathological evaluation.
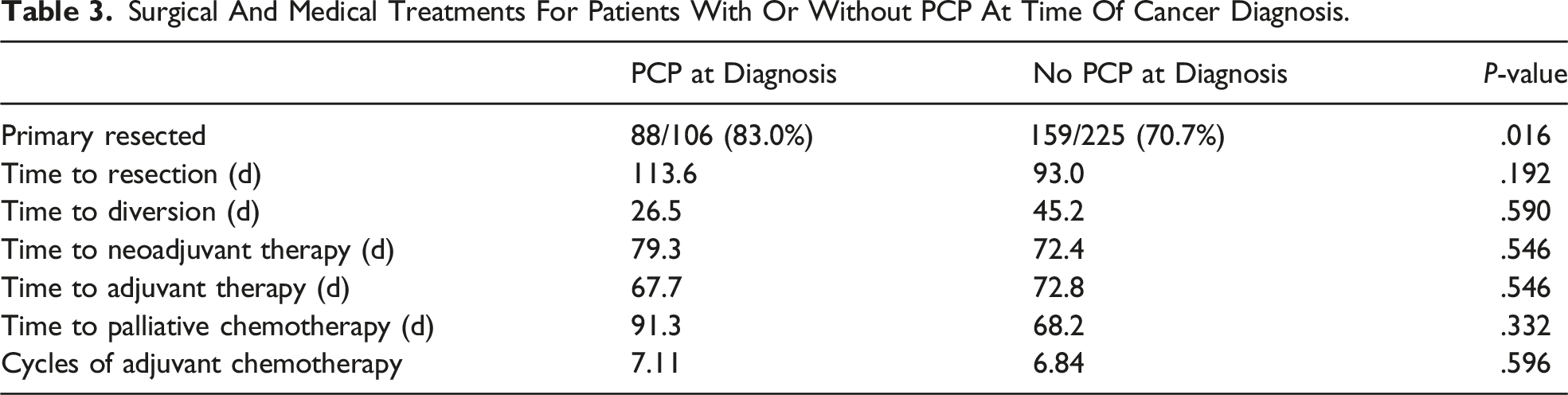
Surgical And Medical Treatments For Patients With Or Without PCP At Time Of Cancer Diagnosis.
Discussion
While other studies have postulated on the benefits of PCPs and cancer outcomes, 8 the reasons for improved outcomes remain incompletely described. Possible contributing factors include improved screening, control of chronic medical conditions, and better coordination of multidisciplinary care.9,10 In our present study, we find that the presence of a PCP leads to improved overall survival in patients with colorectal cancer, and that there are significant differences in the surgical presentation of disease.
The most striking contrast in the two study groups that may partially explain the difference in overall survival was the presentation of colorectal cancer. Patients with PCP were more than half as likely to present with a need for an emergent operation compared to those patients without a PCP. It is well established that emergent presentations are associated with poorer outcomes including higher rate of positive margin, poorer disease-free survival, and poorer overall survival in colorectal cancer patients.11,12 It may be that PCPs obviate acute presentations by initiating or expediting earlier work up for patient symptoms. In our study, patients with PCPs are also more likely to undergo screening colonoscopy, which also likely impacts presentation. 13
Surgical resection of the colorectal cancer primary was achieved more often in patients with a PCP, likely due to the earlier stage of presentation without presence of diffuse metastatic disease or a locally aggressive tumor. However, we did not find a difference in time to treatment, either surgery or chemotherapy between the groups, suggesting that the lower mortality with having a PCP was not necessarily related to improved coordination of care and more expeditious cancer treatment. It is true that our particular health care system, historically having a predominantly uninsured population, has developed pathways to expedite and facilitate care in patients who receive a pathologic diagnosis of colorectal cancer. While the impact of having a PCP on time to cancer treatment is an understudied area, at least several studies have shown a modest decrease in time interval to diagnostics or treatment for patients with PCP.14,15
Ironically, although patients with a PCP at diagnosis were found to have improved overall survival, they also had higher rates of concomitant comorbidities, including diabetes mellitus, hyperlipidemia, and coronary artery disease. We suspect that patients without PCPs were underdiagnosed with these conditions. Furthermore, the management of chronic diseases is also clearly an important aspect that may influence mortality. Uncontrolled diabetes and hypertension are well known to be associated with increased mortality and cardiovascular disease.16,17 Obesity and history of tobacco use were significantly more prevalent in the patients without PCP, likely related to the absence of preventive care.
In our study, we were unable to evaluate insurance status at the time of presentation, which is a significant limitation. Higher quality insurance has been shown to have a positive correlation with access to PCPs and poorer quality insurance or lack of insurance has been associated with poorer colorectal cancer outcomes regardless of race.18,19 It is interesting to note that even in patients who had PCPs at diagnosis, a fair number still presented with advanced disease, with 20% presenting with metastatic disease and 15% with obstruction. Screening colonoscopies, although higher in patients with PCPs, were still overall very low. As such, while we demonstrate that having a PCP is beneficial in many ways, the adherence to and continuity of care likely remain areas for improvement.
Conclusion
The presence of a PCP at the time of colorectal cancer diagnosis was associated with improved overall survival, decreased proportions of patients with emergency presentations and metastatic disease and higher proportions of patients undergoing surgical resection and screening colonoscopy.
Footnotes
Author Contributions
Naveen Balan: study design, data collection, data analysis, article writing and editing
Caitlyn Braschi: data collection, data analysis, article editing
Patrick Kirkland: study design, article editing
Amy H. Kaji: data analysis, article editing
Kathryn T. Chen: study design, data analysis, article writing and editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.