
Abstract
Introduction
Laparoscopic cholecystectomy (LC), one of the most common surgical procedures performed in the U.S., offers a window into the effects of the COVID-19 pandemic on routine surgical care. The purpose of our study was to analyze the effects of the COVID-19 pandemic at a Level-1 trauma center on the performance rate of non-elective LC over time.
Methods
A retrospective chart review from July 2019 to December 2020 identified all non-elective LC cases performed at a level-1 trauma center. Patients were categorized into 4 temporal phases along the course of the pandemic based on statewide incidence data on COVID-19: pre-pandemic, peak 1, recovery, and peak 2. We compared the phases based on demographic information and outcomes.
Results
In total, 176 patients were reviewed. The performance rate in cases/day varied as follows: pre-pandemic .61, 1st peak .34, recovery .44, and 2nd peak .53. The complication rate was highest in the 2nd peak (16%) (P < .05). Compared to the pre-pandemic period, the intra-pandemic period had a higher incidence of complicated gallbladder disease (P < .05). In the non-elderly subgroup, complicated gallbladder disease was significantly more prevalent in the intra-pandemic period compared to the pre-pandemic period (25% vs 10%, P < .05).
Conclusions
Our data suggests a learning curve throughout the course of the pandemic, reflecting a stepwise increase in the performance rate of LC. The higher incidence of complicated gallbladder disease in the intra-pandemic period may imply patient hesitancy to seek routine surgical care, especially among younger patients.
Introduction
The current coronavirus pandemic has brought widespread disruption to health care systems globally. Urgent and elective surgeries have been particularly impacted.1,2 Laparoscopic cholecystectomy (LC), one of the most common surgical interventions in the United States, is no exception. In a retrospective analysis of 559 US hospitals, urgent cholecystectomies were reduced by over 40% during the pandemic. 2 The effects internationally have been similar. 3
Multiple studies, including case reports4,5 and retrospective reviews,6-8 have quantified decreased rates of LC’s between defined pre-pandemic and post-pandemic periods. Likewise, they have reported on operative complications and post-operative outcomes between these periods. Delays in the performance of LC’s have shown to have a negative impact on patient outcomes, quality of life, severity of disease, and hospital cost.6-8
The pandemic is still ongoing and has been an evolving challenge for hospitals and their surgery departments. Hospital policies, public health mandates, and patient engagement in the health care system continuously change according to evolving stages of the pandemic. Few studies have temporally stratified data on LC rates through multiple phases of the pandemic.
The purpose of this study was to analyze the effects of the coronavirus pandemic on the performance of non-elective LC’s at our Level 1 trauma center during four separate phases of the COVID-19 pandemic: pre-pandemic, 1st peak, recovery, and 2nd peak. Separately, we examined surgical outcomes, between the pre-pandemic and intra-pandemic periods. Through our analysis we hope to better understand the effects of a global pandemic on the presentation and optimal management of acute cholecystitis. More importantly, we suggest efforts that may be taken to prevent complications and improve outcomes for future global catastrophes.
Methods
This is a retrospective chart review from a database of patients who underwent non-elective laparoscopic cholecystectomy from July 2019 to December 2020 at a level-1 trauma center in Pennsylvania. Internal Review Board approval was obtained. Patients who presented to the emergency department and were diagnosed with acute cholecystitis on ultrasound and/or CT imaging, were included. Patients who presented with intractable pain and biliary colic or chronic cholecystitis were also included. Patients who underwent elective laparoscopic cholecystectomy were excluded.
The decision for operative intervention was decided by the attending surgeon on call. There were no hospital-wide policies that dictated surgical decision-making. COVID+ patients required use of HEPA filters intra-op, as well as pre-operative and post-operative triage to dedicated COVID floors. Otherwise, there was no mandated difference in the management of COVID+ patients. Most LC cases were performed by one of five attending surgeons. Although surgical technique varied slightly depending on the operating surgeon, there was no significant deviation from standard LC technique.
Patients were categorized into 4 temporal phases along the course of the pandemic based on statewide incidence data on COVID-19: pre-pandemic (7/1/2019-12/31/2019), peak 1 (3/17/2020-6/12/2020), recovery (6/13/2020-9/30/2020), and peak 2 (10/1/2020-12/31/2020). The 1st peak, recovery, and 2nd peak were categorized as the intra-pandemic group. The pre-pandemic period was chosen as an interval several months prior to the first reported COVID-19 case reported in the United States (January 2020). This ensured no COVID-19 specific preparatory actions had been initiated. The start date for the first peak (3/17/2020) was the first day a COVID-19 case was reported in the state of Pennsylvania. The subsequent recovery and peak 2 periods were assigned by analyzing peak and trough data from the statewide incidence reports. We assigned the beginning of peak 2 once the incidence of new cases surpassed 1000 new cases per day in Pennsylvania. 9 We compared the phases based on demographic information and outcomes.
We made the determination of complicated gallbladder disease by reviewing operative notes and pathology findings. Histopathology, which was performed in all cases, confirmed the diagnosis with a description reflecting the extent of gallbladder inflammation. Descriptors including “perforation,” “gangrene,” “suppuration,” and “fibrinous adhesions” reflected a relatively high degree of inflammation and were therefore used to categorize complicated gallbladder disease.
In a separate analysis, we divided the patients into pre-pandemic and intra-pandemic (1st peak, recovery, and 2nd peak) groups. We compared the groups based on demographic information and outcomes. We then performed subgroup analyses on elderly and non-elderly patients. Elderly patients were defined as patients >65.
T-testing and Chi-square were used to compare continuous and categorical variables, between each study group. Statistical analyses were 2-sided and P < .05 was considered statistically significant. All statistical analysis was conducted using SPSS (Version 22).
Results
In total, 176 patients met inclusion criteria. The pre-pandemic, 1st peak, recovery, and 2nd peak phases included 83, 24, 31, and 38 patients, respectively. Figure 1 shows a graphical representation of the LC performance rate throughout each phase of the pandemic. The performance rate in cases/day varied as follows: pre-pandemic .61, 1st peak .34, recovery .44, and 2nd peak .53. Laparoscopic cholecystectomy average case rate per day through each phase of the COVID-19 pandemic.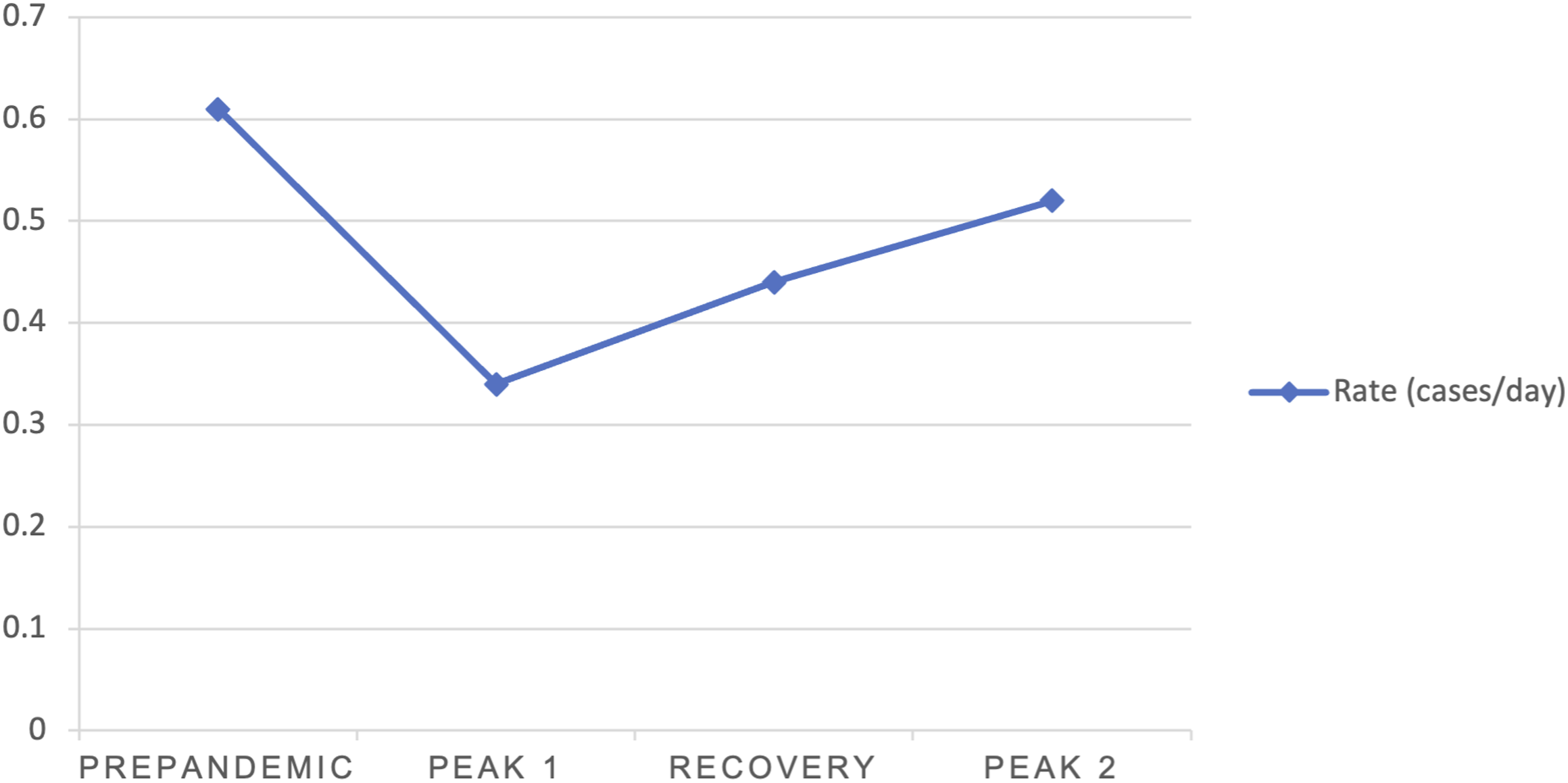
Evolution of Clinical Parameters Through Each Phase of the COVID-19 Pandemic.
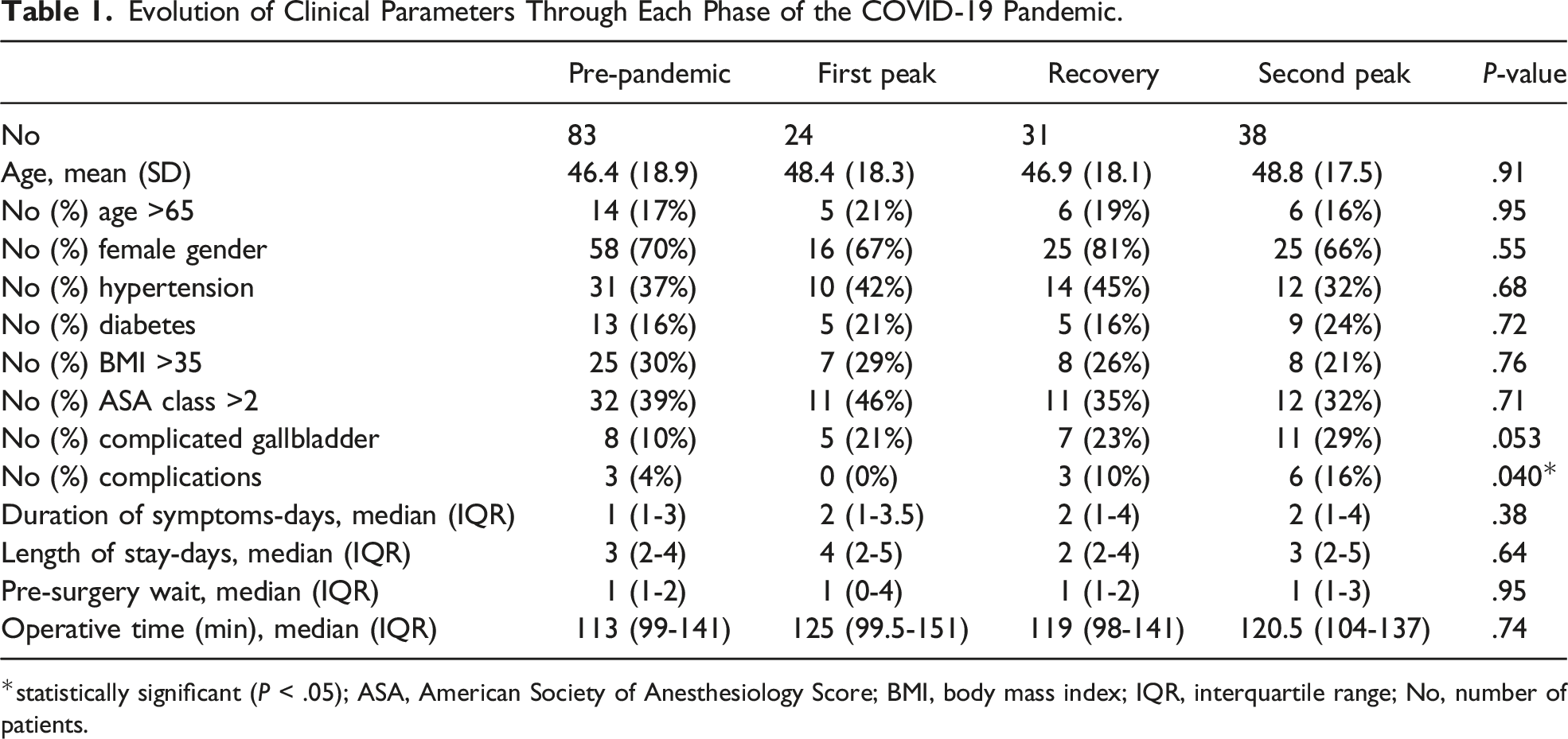
*statistically significant (P < .05); ASA, American Society of Anesthesiology Score; BMI, body mass index; IQR, interquartile range; No, number of patients.
Pre-Pandemic and Intra-Pandemic Comparison of Laparoscopic Cholecystectomy in All Patients.
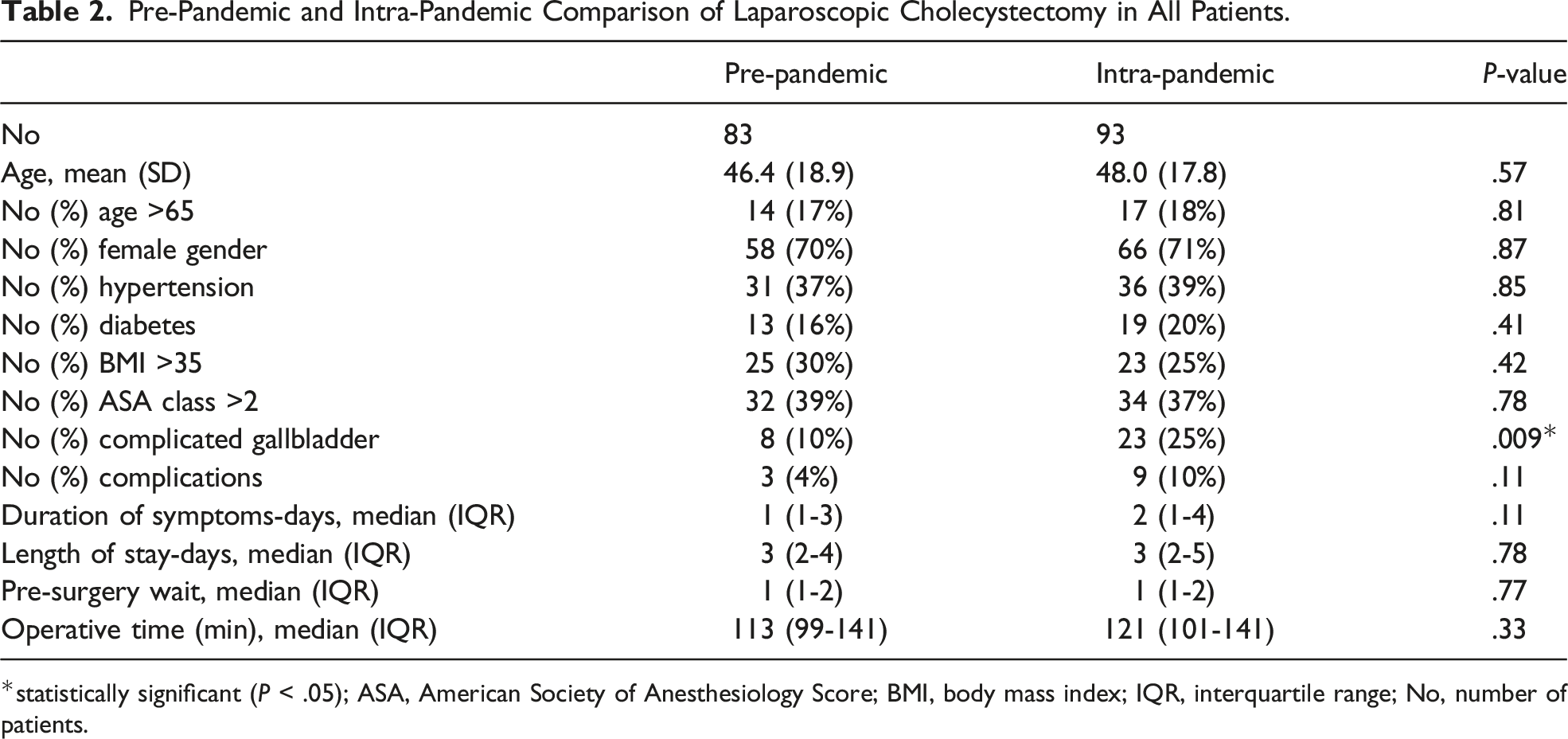
*statistically significant (P < .05); ASA, American Society of Anesthesiology Score; BMI, body mass index; IQR, interquartile range; No, number of patients.
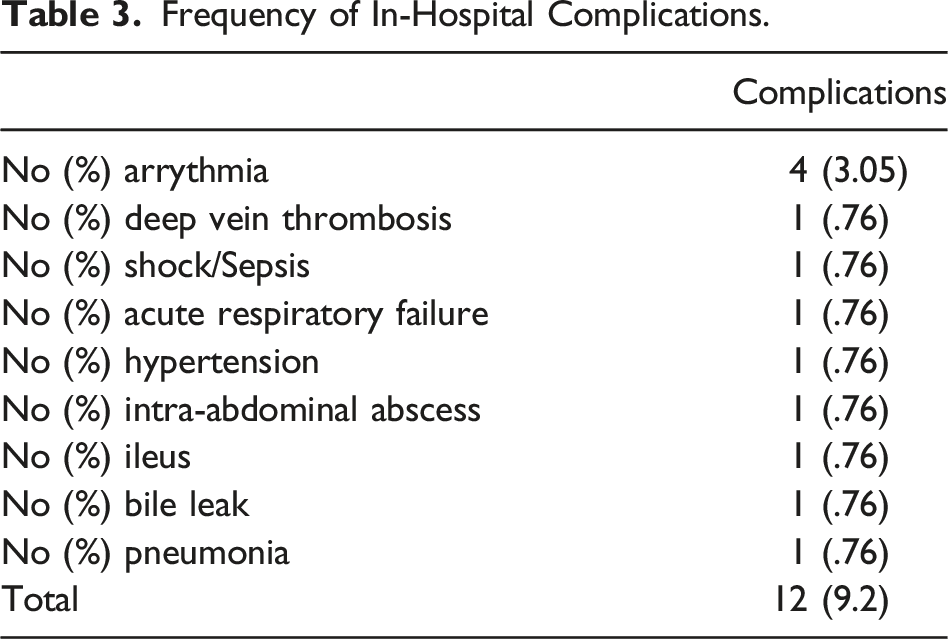
Frequency of In-Hospital Complications.
Pre-Pandemic and Intra-Pandemic Comparison of Laparoscopic Cholecystectomy in Non-Elderly Patients.
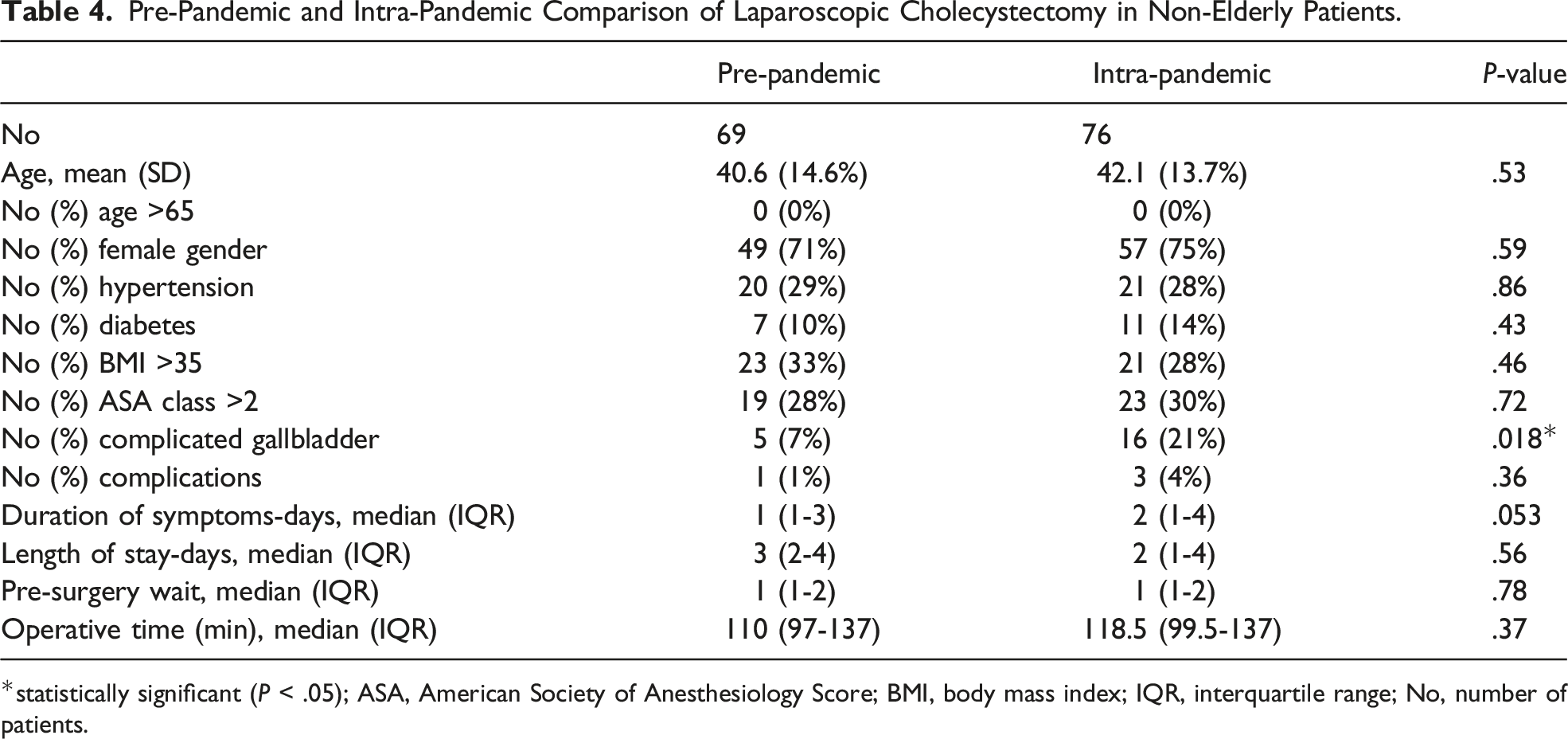
*statistically significant (P < .05); ASA, American Society of Anesthesiology Score; BMI, body mass index; IQR, interquartile range; No, number of patients.
Pre-Pandemic and Intra-Pandemic Comparison of Laparoscopic Cholecystectomy in Elderly Patients.
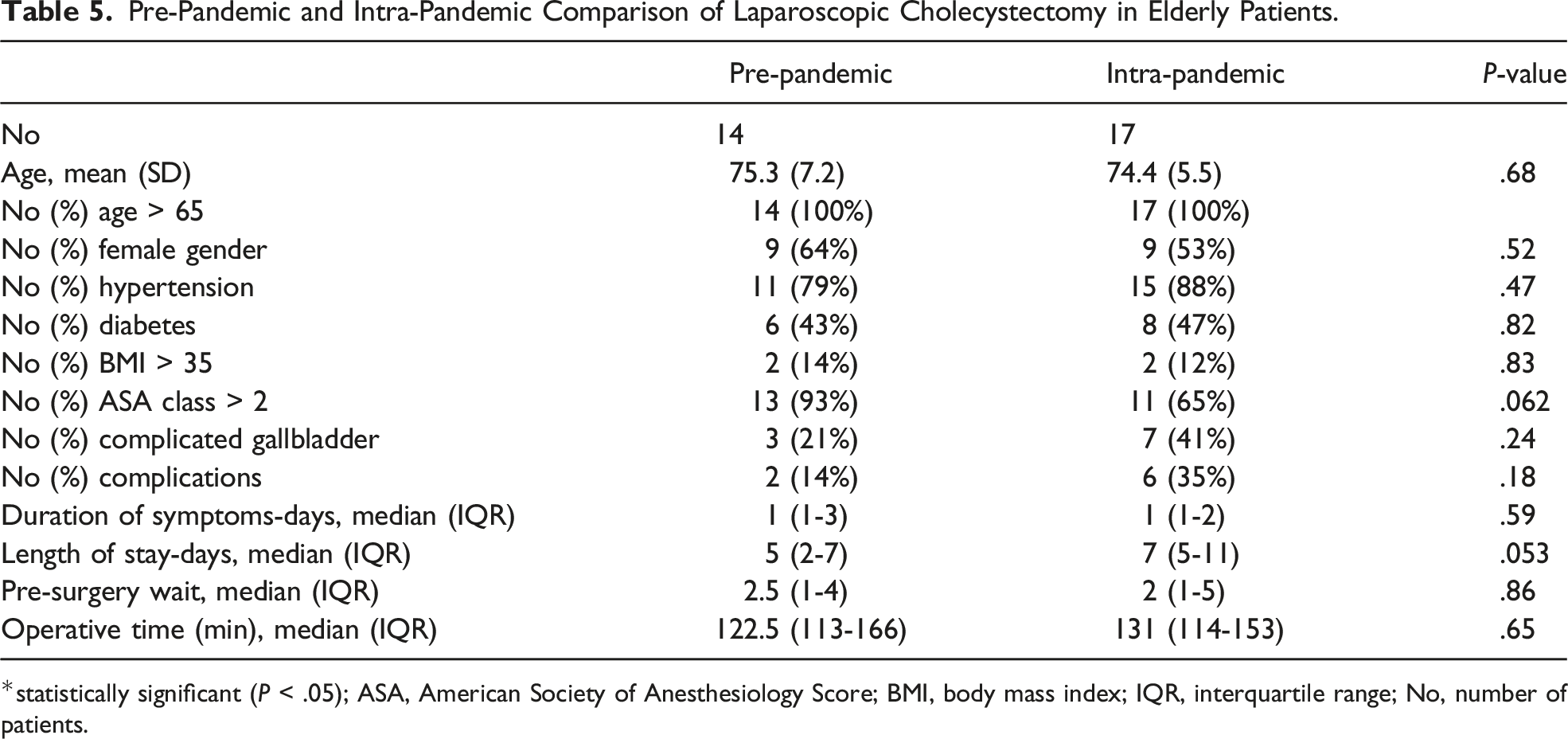
*statistically significant (P < .05); ASA, American Society of Anesthesiology Score; BMI, body mass index; IQR, interquartile range; No, number of patients.
Discussion
The purpose of our review was to analyze the effects of the coronavirus pandemic on the performance of non-elective LC’s at a level 1 trauma center. We know of no other study charting the effects of the pandemic on performance of LC’s through multiple peaks of the pandemic. Our retrospective chart review found that the coronavirus pandemic resulted in a marked decline in the performance rate of LC’s followed by a stepwise recovery. Patients undergoing non-elective LC were significantly more likely to present with complicated gallbladder disease during the recovery and 2nd peak. Complications were most prevalent during the 2nd peak of the pandemic and trended higher as the pandemic progressed. On age-stratified analysis, younger patients were significantly more likely to present with complicated gallbladders in the intra-pandemic period.
Between the pre-pandemic period and the 1st peak, there was a 44.3% reduction in the performance rate of LCs. This decline mirrors a similar trend throughout the country and internationally.2,3 In a retrospective analysis of 559 US hospitals from November 2019 to June 2020, urgent cholecystectomies were reduced by 42% in April 2020 compared to mean monthly case volumes from November 2019 through January 2020. 2 Internationally, a survey of 153 hospitals in Spain found that elective cholecystectomies were canceled in 96.7% of centers and conservative management was selected for acute cholecystitis in 90% of centers. 3 Echoing this trend, national guidelines at the time suggested postponing routine surgical cases when feasible.10,11
After this initial decline, the performance rate of LC’s made a stepwise recovery from a nadir of .34 cases/day during the 1st peak, .44 during the recovery phase, and .54 during the 2nd peak. We suggest that this steady rate of increase may be attributed to a hospital-system learning curve, which became more adept at tiding the challenges of routine surgery as the pandemic progressed. Nnaji et al reviewed measures taken at a single center in their prospective review of 104 patients who underwent LC during the peak of the pandemic including routine COVID-19 testing and the utilization of universal PPE precautions. 12 Other hospital systems have proposed more unique measures such as weekend focused surgeries to aid in long waiting lists for operative care. 13 Specific measures taken by our hospital included pre-operative COVID testing for all patients, universal operative PPE requirements, use of high-efficiency particulate air filters, pre-operative and post-operative triage to dedicated COVID floors, required post-op recovery in the OR, and minimizing OR staff during airway procedures. We suggest that implementing these measures over time contributed to the recovery in case rate as the pandemic progressed.
Additionally, it is possible that the dangers of operative delay may have been realized as the pandemic evolved, spurring the hospital-system to encourage operative management. Reports during the pandemic period demonstrated the dangers of postponing routine surgery on patient outcomes. Farber et al reviewed 313 patients with acute cholecystitis and symptomatic cholelithiasis and demonstrated that patients presented with more severe cholecystitis during the pandemic. 6 Fouad et al found that conservative management in the setting of acute cholecystitis resulted in high readmissions while delayed cholecystectomy was associated with increased operative time and blood loss, more complicated gallbladder disease, and increased length of stay. 8 Other reviews found adverse effects on cost and quality of life. 7 We presume, with this change in the general consensus, there was heightened urgency to proceed with operative intervention. It is also likely that with the discontinuance of elective LC, cases that may have otherwise presented in the first peak, presented later as acute cholecystectomies. As a result, even under the duress of a 2nd peak, the LC rate continued to increase at a steady pace.
As reported, the incidence of COVID-19 in our cohort was 4.3% which mirrored the incidence of COVID-19 in the state of Pennsylvania during our review. According to contemporaneous Centers of Disease Control (CDC) data for the state during the study period, the largest COVID-19 cumulative case rate was 5066 per 100 000 patients. Less than 4% of emergency department visits were diagnosed with COVID-19. 14 Based on these findings we presume the initial reduction in case count may not largely reflect cancellation based solely on COVID+ status. Rather, it seems hospital-system policies, in response to staff redistribution and resource allocation, may have limited our case volume regardless of the individual patient’s COVID status.
The progression in performance rate may suggest more willingness among patients to seek in-patient care as the pandemic continued. Early in the pandemic, patient hesitancy may have played an outsized role in delaying surgical care. Hesitancy to seek medical care was a common thread throughout the health care system during pandemic. In a Swedish cross-sectional study of 326 patients with acute myocardial infarction, 19% of patients reported hesitancy to seek medical care due to the pandemic. This apprehension was largely related to “fear that the health care services were already overcrowded” and “a fear of becoming infected with COVID-19 in hospital.” 15 Similar findings were found in a Chinese cross-sectional study of suspected transient ischemic attacks. In this study, 63% of 143 participants avoided going to the hospital due to concerns about in-hospital infection. 16 In the United States, 41% of respondents to a web-based survey conducted by Czeisler et al reported delaying and avoiding any medical care, including emergency care (12%) and routine care (31.5%), due to concerns about COVID-19. 17
As mentioned, complicated gallbladder disease trended higher as the pandemic progressed and was significantly higher in the intra-pandemic period. Other reviews have found similar outcomes with respect to complicated gallbladder disease.6,8 Interestingly, on age-stratified analysis, this discrepancy can largely be attributed to younger patients. We suspect that an overall hesitancy among patients to seek medical care may have factored into gallbladder disease progression, culminating in more severe illness at presentation to our institution. While this applied to elderly patients as well, it may have uniquely burdened younger patients. In our review, along with having a significantly higher rate of complicated gallbladder disease, younger patients demonstrated a trend in longer pre-operative duration of stay in the intra-pandemic period by about 1 day. This trend did not hold for elderly patients who had an identical duration of symptoms in the pre-pandemic and intra-pandemic periods (1 day). In addition to older adults generally being more susceptible to severe gallbladder disease, older patients are more likely than younger adults to utilize the emergency department, to be admitted to the hospital, and to have repeat visits to the ED. 18 A review article by Kennedy et al showed that younger adults, particularly males, are more likely to leave the emergency department without being seen. 19 This is compounded by the fact that younger adults are less perceptive of pain compared to older counterparts and consequently, may be less likely to seek out care.20-22
Other factors that contributed to complicated gallbladder disease and delayed presentations may have included limited or loss of access to health insurance compounded by financial burdens of the COVID-19 pandemic. A September 2020 report by the Harvard T. H. Chan School of Public Health which included 2992 respondents, found that one in five households in the US could not afford medical care when needed during the COVID outbreak. 46% of US households reported serious financial problems during the pandemic, with higher rates among minority groups. Moreover, 9% of households with anyone who has had COVID-19 reported losing their health insurance during the pandemic. 23 Considering the unique system of employment-dependent health insurance in the United States, job loss also presented challenges to health care delivery. The uninsured rate of those who lost or left their jobs in the early weeks of the pandemic was 26.3% compared to 10.7% of those who retained their jobs. 24 These financial burdens may have targeted the young and minority groups, who are less likely to have adequate savings. 25 Studies on adolescent health have shown that the COVID-19 pandemic generated economic stressors that uniquely affected college student’s wellbeing. 26 Our institution primarily treats historically underserved populations who are more likely to be financially disadvantaged. We suspect that combined with hesitancy to seek medical care due to the pandemic, financial strain incurred from pandemic-related hardship was a barrier for our patient population to seek care for gallbladder disease.
Finally, we suspect the trend in complication rate is largely a reflection of complicated gallbladder disease. The complication rate was highest at the 2nd peak of the pandemic (16%). This period also corresponded to the highest rate of complicated gallbladder disease (29%). Baseline factors such as age and comorbidities were not significantly different as the pandemic progressed. Of the 12 total complications that occurred in our cohort, half of them (6 complications) occurred in complicated gallbladder cases. Considering that a disproportionate number of complications occurred in the setting of complicated gallbladder disease, we presume the complication rate reflected complicated disease rather than a selection bias towards unfavorable baseline characteristics. We did not find a relationship between the COVID-19 status and complicated gallbladder disease. Only 1 patient with complicated gallbladder disease and 1 patient with complications was COVID+. We suspect the pathophysiology of COVID-19 does not directly contribute to complicated gallbladder disease however further studies are needed to substantiate this point.
There were several limitations to our study. There are inherent limitations to performing any retrospective analysis. There was no standardized approach to deciding on operative management. Rather, this was left at the discretion of the operating surgeon on call. There may have been differences in operative technique in surgeons performing LCs which may have biased our outcome measures. We relied on histopathologic reports to assess the severity of gallbladder inflammation and define complicated disease. There is no universally validated pathologic determination of cholecystitis severity. We did not include long-term follow-up outcomes in our results. Our conclusions, which are based on a retrospective data from a single-center analysis, cannot prove causal relationships between the incidence of COVID-19 and LC rates.
As health care continues to adapt to COVID-19, we must advocate for patients who are especially vulnerable to the pandemic’s effects. We believe that results from our institution are a reflection that COVID has had far reaching impacts on patient behavior and the ability to seek routine surgical care for gallbladder disease. Consequently, continued efforts must be made to decrease hesitancy in seeking appropriate treatment and a return to pre-pandemic operative rates. Policies must also be implemented to address the continued financial hardship of patients. Delayed care will only result in more severe disease with higher associated costs, and more importantly, poorer outcomes for at-risk patients. Lastly, special considerations must be made for younger patients who may be particularly vulnerable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.