
Abstract

Intestinal malrotation is a congenital condition caused by failure of normal bowel rotation during embryological development leading to abnormal anatomic positioning and fixation of the fetal bowel. Its incidence has been reported in 1 in 200 to 1 in 500 live births. 1 Symptomatic malrotation develops in approximately 1 in 6000 live births, with over half of cases presenting before 1 year of age. 1 Very few cases present in adolescence and adulthood. Ladd’s procedure is the standard of care for children presenting with intestinal malrotation and/or midgut volvulus. The procedure is generally considered to be curative, but there have been rare reports of recurrent volvulus in patients who had previously undergone repair. The risk of recurrence is estimated to be 2-7%. 2 We present a case of a 13-year-old boy who had undergone an emergent Ladd’s procedure for midgut volvulus and re-presented in less than 72 hours with acute small bowel obstruction due to re-volvulus requiring a repeat Ladd’s operation. Not only is volvulus rare at this age, but most cases of recurrence have been reported to present months to years following repair, however this case presented in a matter of days. Furthermore, we conduct a brief review of the literature on various modifications to Ladd’s procedure and alternate techniques that may reduce the risk of recurrence.
A 13-year-old boy presented to our emergency department with a 1-hour history of acute onset periumbilical and suprapubic abdominal pain. He had associated nausea, bilious emesis, and decreased bowel movement. The patient had never experienced similar symptoms and had no previous medical or surgical history. Physical examination revealed decreased bowel sounds in all four quadrants and diffusely tender abdomen. Patient’s computer topography (CT) of abdomen and pelvis showed no definite evidence of obstructive bowel and the presence of fecal mass in large bowel. The patient was presumed to have constipation and sent home with suppository, pain meds and anti-emetics.
He returned to the emergency department 2 days later with worsening abdominal pain. A repeat CT showed dilated loops of small bowel, a collapsed large bowel, and the characteristic whirlpool pattern pathognomonic for midgut volvulus secondary to intestinal malrotation (Figure 1). Routine admission labs showed elevated white cells count of 12.8 × 103 mg/L and a normal lactic acid of 1.7 mmol/L. His abdominal exam was consistent with peritonitis. He was prepared for emergent exploratory laparotomy. Patient’s contrast-enhanced CT of abdomen and pelvis showing whirlpool pattern pathognomonic of malrotation with midgut volvulus.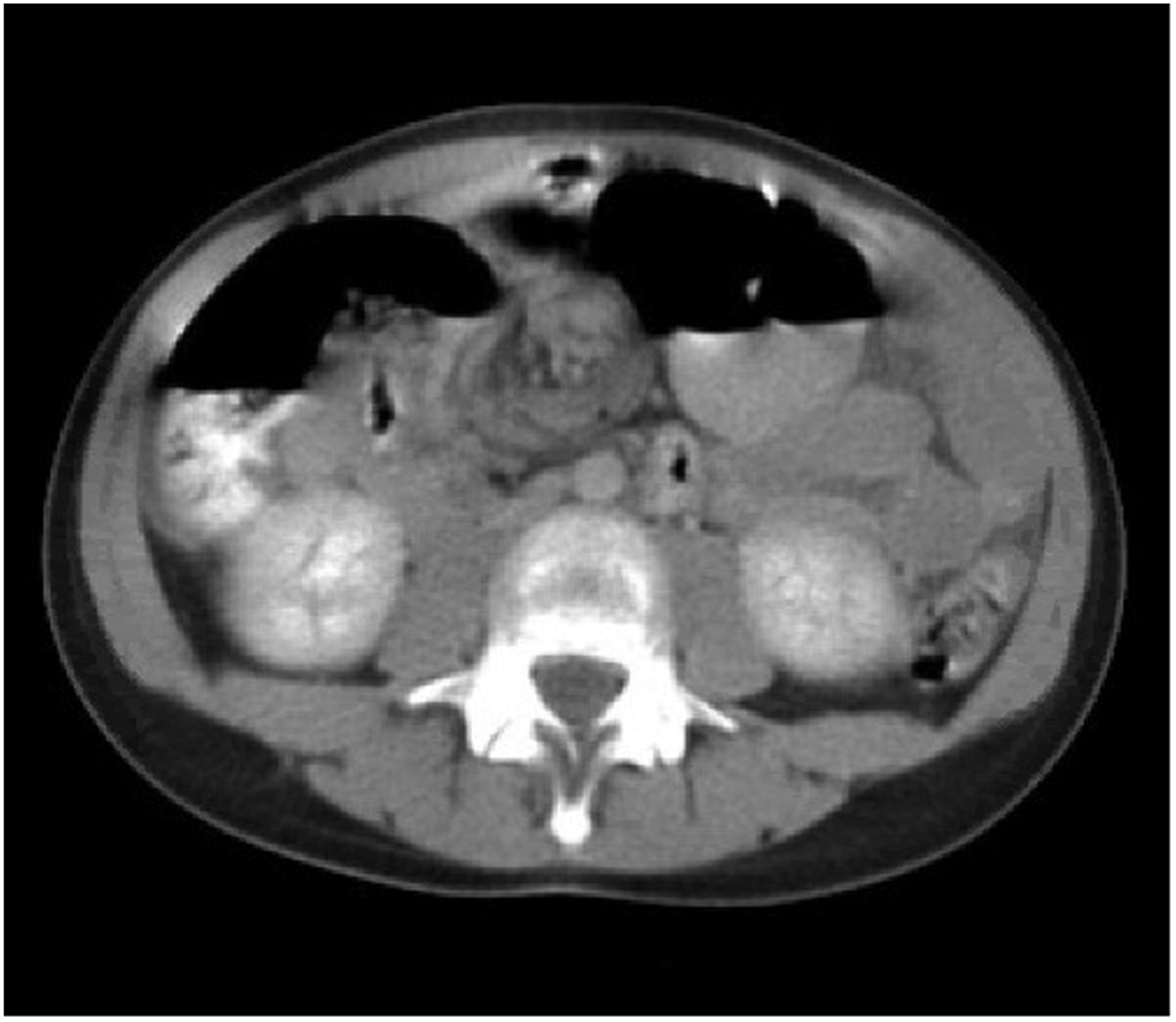
The operative findings were consistent with intestinal malrotation and midgut volvulus, the duodenal-jejunal flexure was localized on the right side of the upper abdomen, and the cecum and proximal ascending colon on the upper right side of the abdomen. A fibrous band was seen extending from the distal ascending colon on the left across the duodenum to the right lateral abdominal wall. The mesentery of the vovlulized segment was narrowed and torsed at the base. Fortunately, the patient’s small bowel was still viable. An open Ladd’s procedure for malrotation was performed by lysing Ladd’s bands, evisceration and counterclockwise detorsion of the bowel, broadening of the base of the mesentery, and prophylactic appendectomy. The cecum was then repositioned in the left lower quadrant of the abdomen and the small bowel was placed on the right upper quadrant of the abdomen to reduce the risk of re-volvulus. The mesentery was broadened and laid flat to avoid retwisting upon closure.
The patient’s recovery was unremarkable until post-op day 3, when he began complaining of increasing abdominal pain started having issues with his pain. On physical exam, he was normotensive, tachycardic, tachypneic, and afebrile with no leukocytosis. The patient’s abdomen was firm, distended, diffusely tender, with rebound tenderness and guarding. He was taken emergently for another exploratory laparotomy given concern for bowel ischemia/necrosis. On entrance into the abdominal cavity, his mesentery was noted to have re-volvulized less than 72 hours after the initial procedure. The bowel was noted to be healthy and viable upon detorsion. The mesentery was judiciously dissected and broadened to prevent another recurrence.
Midgut volvulus is the most feared complication of intestinal malrotation because it carries a substantial risk of bowel wall ischemia, necrosis, and possible perforation. 1 These potentially catastrophic consequences necessitate an immediate diagnosis and prompt intervention. Early signs of volvulus formation may be difficult to diagnosis and diagnosis is greatly facilitated by imaging via upper gastrointestinal contrast series (UGI), CT, or both.
Though Ladd’s procedure is curative in most cases, there have been rare reports of recurrent volvulus following the operation. Consequently, when a child with a history of Ladd’s procedure presents with persistent gastrointestinal symptoms, they are often evaluated for postoperative adhesion-related obstruction, but the diagnosis of recurrent volvulus is rarely entertained. 3
The exact etiology for the development of recurrent midgut volvulus in this case is unclear, however it is possible that even though the cecum was relocated to the left lower quadrant and the mesentery sufficiently broadened, the mesenteric dissection might have not been sufficiently aggressive, and thus allowing for return of bowel to its original orientation and compromised state. Care is warranted when broadening the mesentery to ensure the bowel and its mesentery remains unrestricted, free from tension and with adequate laxity, if it is to remain in an uncompromised state.
Over the years, various modifications to Ladd’s procedure have been suggested to ensure proper positioning of the bowel and avoid recurrence of volvulus. A maneuver proposed by 1 of Professor Ladd’s students, Alexander Bill, involved proactively suturing the duodenum to the fascia overlying the right kidney (duodenopexy), and suturing the cecum to the left inner abdominal wall (cecopexy). 2 While some surgeons have embraced these techniques, there have been conflicting reports in literature on the success of these maneuvers as to the prevention of recurrent volvulus. Some authors have advised against intestinal fixation maneuvers postulating that it constitutes an unnecessary procedure that may carry a risk of recurrence or hernia from further manipulation of the peritoneum and its contents. 2 The benefit of intestinal fixation/pexy maneuvers remain controversial.
In 2021, a new operation for malrotation termed “Kareem’s procedure” was proposed as a safe and effective alternative to Ladd’s procedure that significantly reduces the risk of recurrenct volvulus. 4 The procedure involves reconstructing the native gut configuration by completing the 270° embryonic counterclockwise-midgut rotation, reversal of vascular-inversion and establishment of mesenteric-attachments. 4 The study has had no reports of recurrent/de novo volvulus in the mean follow-up period of 36 ± 23 months. 4 While Kareem’s procedure appears promising, the novelty of the procedure offers data limitation on the long-term outcomes of this operation. In addition, it is significantly more complicated than the Ladd’s procedure.
An important teaching point in this case is that volvulus may recur at any time following the Ladd’s procedure, even as little as 3 days as seen in this case. It is therefore critical to maintain a high index of suspicion for recurrent volvulus in any patient with a history of malrotation, regardless of whether or not they have been treated with Ladd’s procedure, lest a recurrent midgut volvulus be missed with catastrophic consequences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.