
Abstract
Background
Bleeding complications are a risk associated with hemorrhoid procedures. Despite the prevalence of anticoagulant and antiplatelet therapies, including newer direct oral anticoagulants (DOACs) in the aging patient population there is a paucity of data regarding the impact of the use of antithrombotic therapy (AT) especially DOACs, on bleeding complications of hemorrhoid procedures.
Methods
We retrospectively reviewed charts of patients who had undergone a total of 1152 procedures, including hemorrhoid excision and ligation, at a single institution in the years 2016-2018. We noted whether they were prescribed AT, the indication for therapy, perioperative medication management, whether a PBE occurred, and how the PBE was managed.
Results
PBE’s were noted in 5.92% of patients on ATs, as opposed to 2.66% of patients not on ATs (P = .014.) The odds ratio of having a PBE when on ATs vs not on ATs is 2.3 (95% CI 1.21 to 4.38, P = .011). Seven out of 40 (17.5%) total PBE’s required hospital admission or repeat procedure, and this was not associated with AT use. Surprisingly, although males represented most of the patients on ATs, females were statistically more likely to have a PBE following a hemorrhoidectomy if on ATs.
Discussion
Patients on AT have an elevated risk of PBE compared to patients not on AT. No significant difference was found between the two groups when considering only those PBE’s severe enough to require hospital admission or repeat procedure. Further research is required to establish clear guidelines regarding the perioperative management of AT for hemorrhoid procedures.
Introduction
One of the most dreaded complications of hemorrhoid procedures is a postoperative bleeding event (PBE.) Occurrence rates are between 0 and 5% following hemorrhoidectomy.1-5 The risk factors which predispose patients to a PBE have been studied elsewhere, and the effects of sex, number of piles, and lifestyle have been discussed. 3 The use of antithrombotic therapy (AT) is generally considered to increase the risk of PBE after surgical procedures. Furthermore, the use of AT is sometimes considered to be prohibitive for certain elective procedures, such as hemorrhoidectomy. The safety of withholding AT during the perioperative period has been well described, but the thoughtful provider must be concerned about the risk of thromboembolic disease while it is held.1-3 There are multiple factors to consider when determining the best perioperative management of AT, including specific patient, drug, and procedure factors.
Over the past decade, the use of AT has increased with the advent of direct oral anticoagulants (DOACs.) These medications are considered to have a better safety profile than their predecessors.6,7,8 This in combination with their ease of use has led to a dramatic increase in prescriptions for DOACs.9,10 The American College of Chest Physicians has sought to create thoughtful guidelines for the management of AT during the operative period.11,12 These trials do not include hemorrhoidectomy in their review and create a gap for providers to extrapolate this data to their practice. The purpose of this study was to examine the impact of AT and its current perioperative management on the incidence of PBE’s following hemorrhoid procedures, including excision and ligation.
Materials and Methods
The study protocol was approved by the Prisma Health Institutional Review Board as a retrospective chart review. Current Procedural Terminology (CPT) codes were selected in order to identify charts within the electronic medical record of patients who had undergone hemorrhoidectomy in the years 2016-2018 at Prisma Health-Upstate, 1 of the largest not-for-profit hospital systems in South Carolina. All procedures were performed by a group of 6 colorectal surgeons within the health system, with similar frequency of procedures among all providers.
Current procedural terminology codes included in our study encompassed hemorrhoidal ligation, including rubber band and suture techniques, and excisional hemorrhoidectomies. All excisional hemorrhoidectomies were performed using a closed Ferguson technique with only subtle differences between providers. Chart review was performed within the electronic medical record (EMR) by undergraduate students who were trained and supervised by surgeons, and a secondary chart review of all charts with PBE’s was performed by a surgical resident training in colorectal surgery.
PBE’s were noted during chart review generally in 1 of 3 forms: a historical report of significant postoperative rectal bleeding at the follow up office visit, postoperative rectal bleeding prompting a phone call to the office, and/or a documented visit to the emergency room or urgent visit to another physician due to rectal bleeding postoperatively.
Perioperative management of AT.
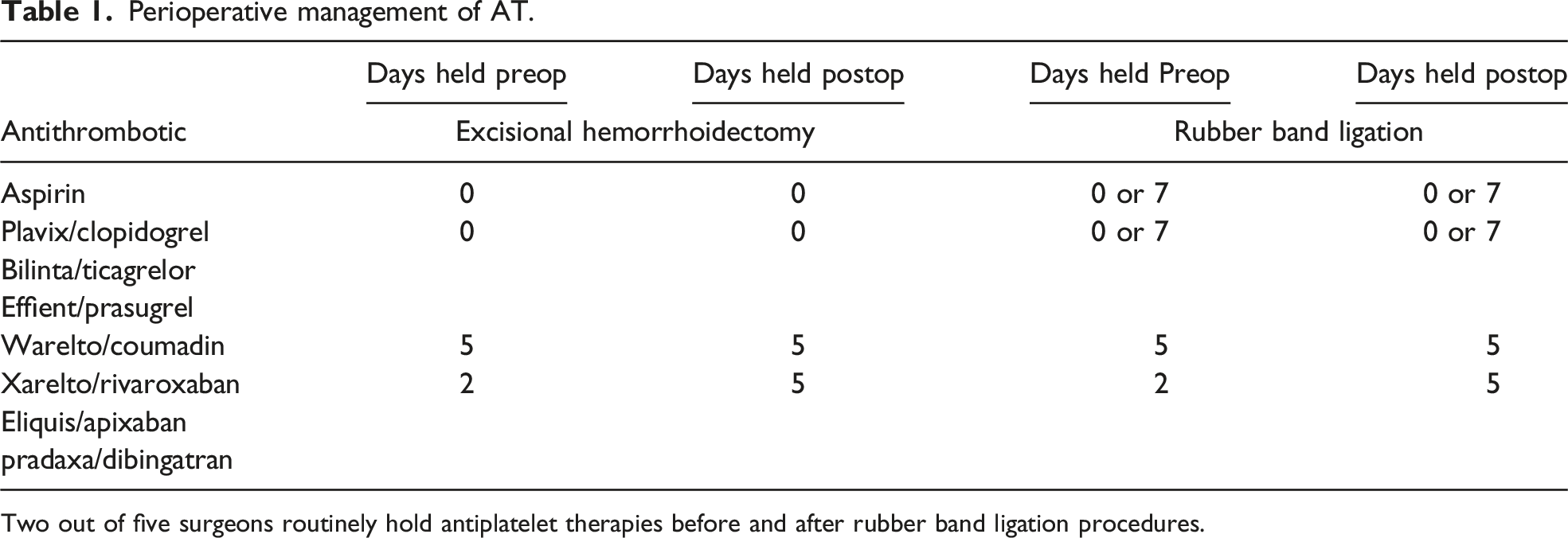
Two out of five surgeons routinely hold antiplatelet therapies before and after rubber band ligation procedures.
Standard deviation, interquartile ranges, and P values from students t test are all indicated in exhibits and were calculated using Microsoft Excel.
Results
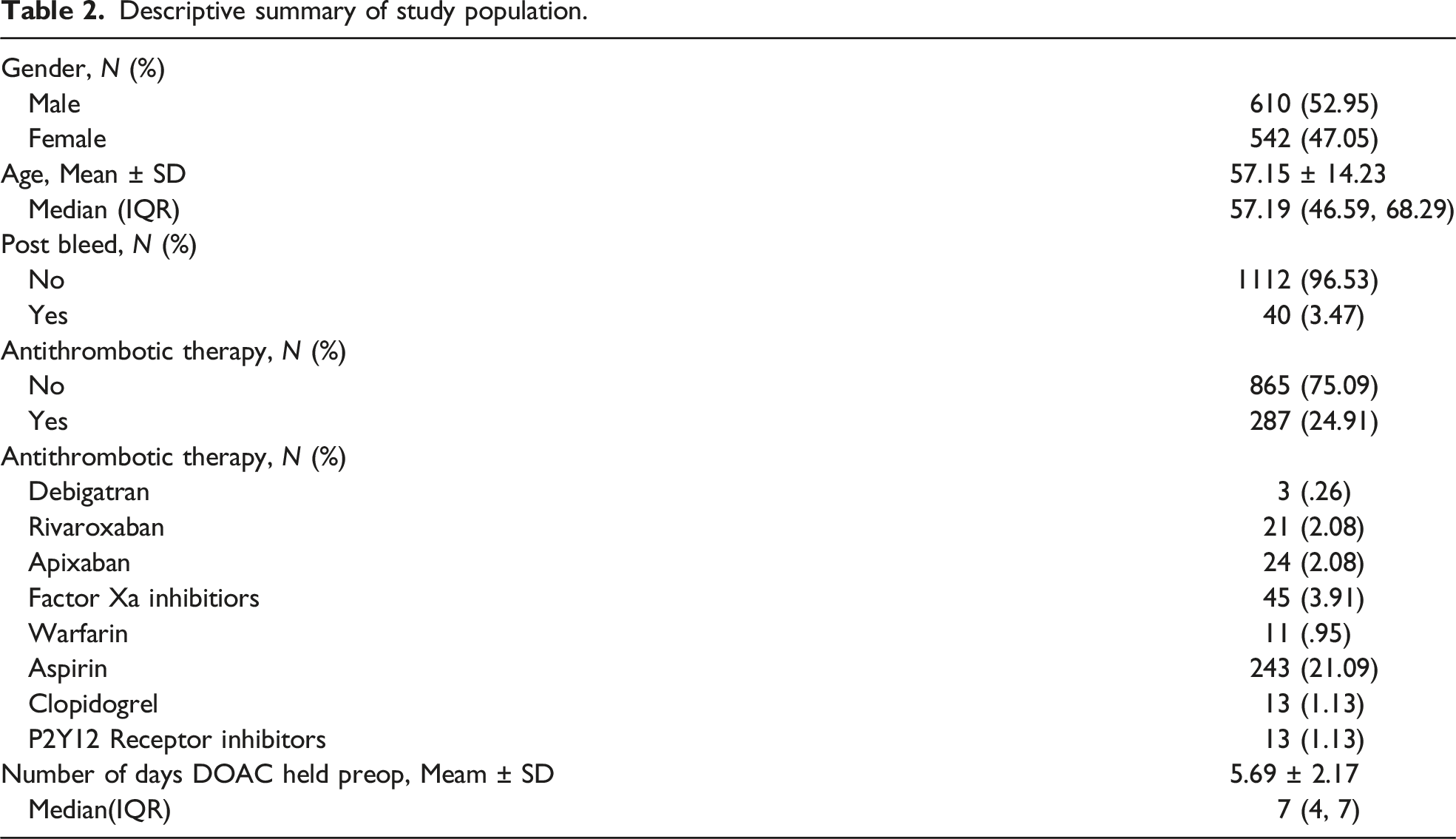
Descriptive summary of study population.
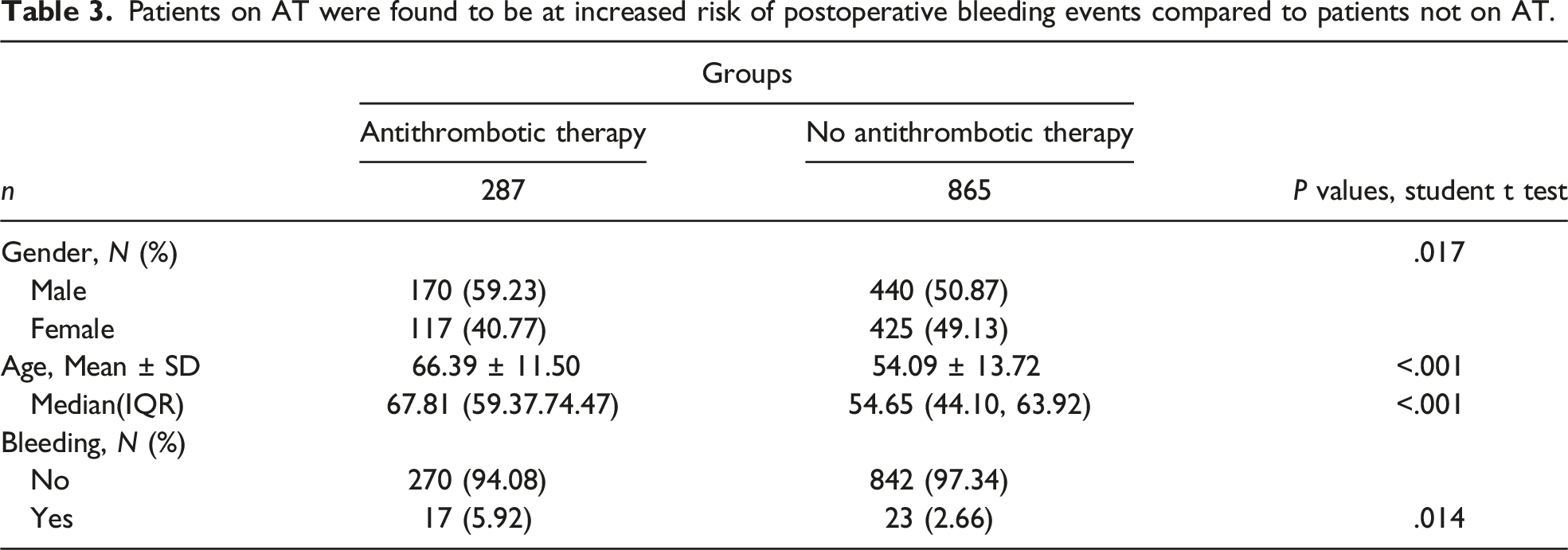
Patients on AT were found to be at increased risk of postoperative bleeding events compared to patients not on AT.
Patients on AT who underwent an excisional hemorrhoidectomy were significantly more likely to have a PBE than patients on AT who underwent a rubber band ligation (P = .04).
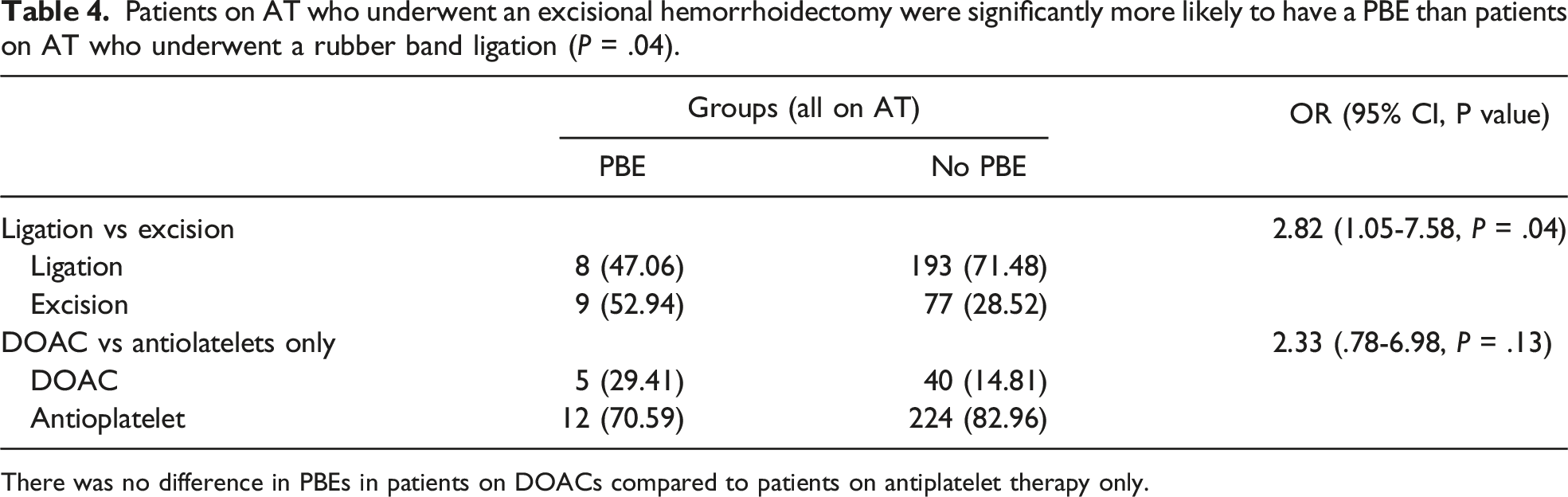
There was no difference in PBEs in patients on DOACs compared to patients on antiplatelet therapy only.
Of the 40 postoperative bleeding complications that occurred, 2 required inpatient admission, 2 required anoscopy with bedside hemostasis, and 3 required return to the OR. There was no statistical significance when evaluating for an association between the management/severity of the postoperative bleeding event and the presence or absence of AT: the odds ratio of having a PBE related complication while on AT vs not is 2.05 (95%CI .39-10.70, P = .39). This is likely in part due to the small numbers of PBE’s that required intervention, such as hospital admission or repeat procedure.
An unexpected finding with regard to gender was noted to be statistically significant. 59.2% of the patients taking AT were male, however this same percentage was not reflected in the number of patients who experienced PBE’s. 35% of the patients on AT who experienced a PBE were male (Figure 1). This may be due to the low numbers of patients in these subgroups, however, it was statistically significant and deserves some consideration. We noted a statistically significant gender discrepancy suggesting that females on AT are more likely to have a PBE than their male counterparts.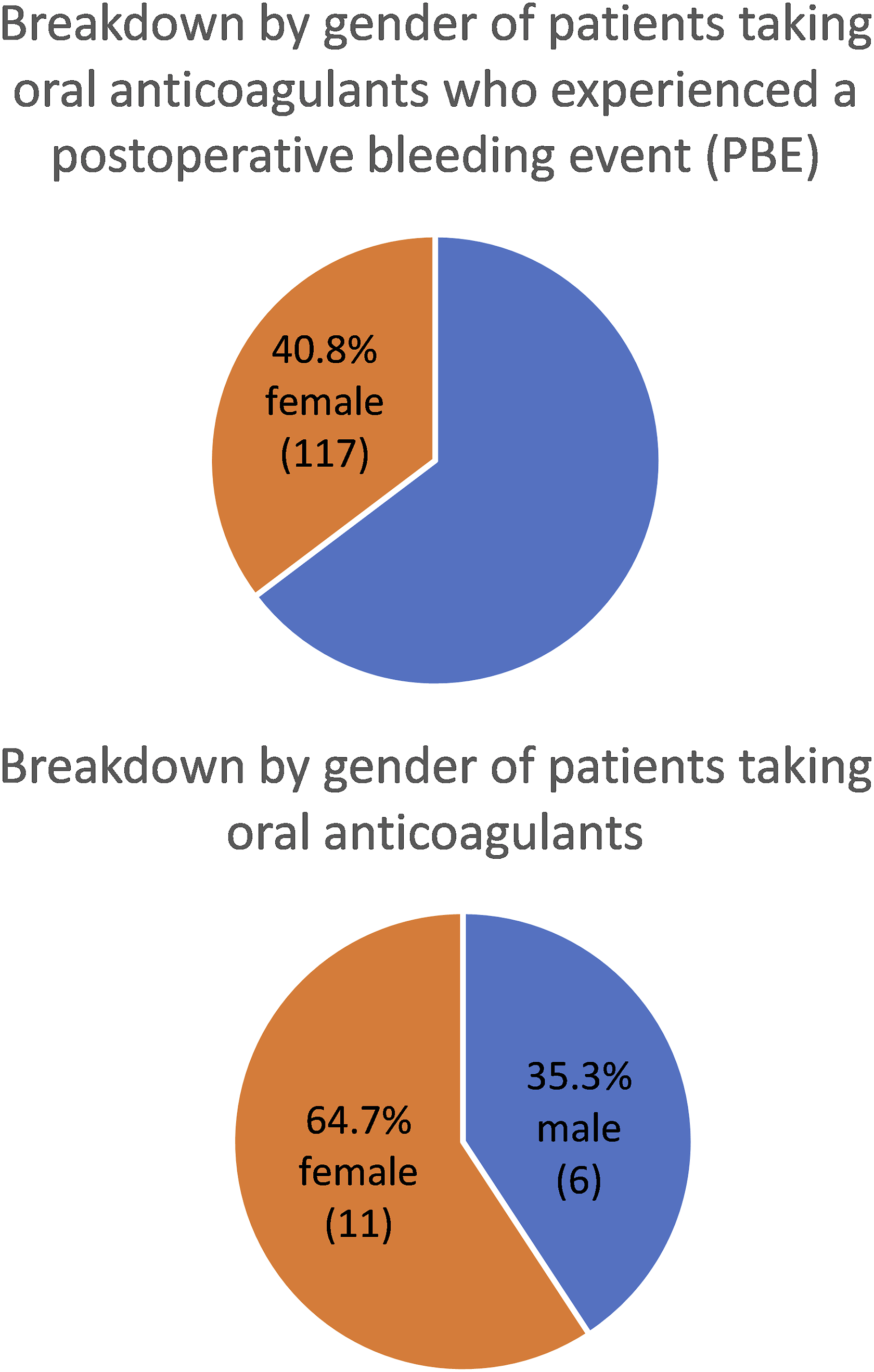
Discussion and Conclusion
We retrospectively reviewed 1152 total hemorrhoid procedures, including ligations and excisions, at a single institution and found that PBE’s were significantly more likely to occur in patients on chronic AT. PBE’s were noted in 5.92% of patients on AT, as opposed to 2.66% of patients not on AT (P = .014.) The odds ratio of postop bleeding complications for patients on AT compared to those not on AT is 2.3 (95% CI 1.21-4.38, P = .0108).
There were 40 total PBE’s noted in our study, with only 7 of the 40 requiring hospital admission and/or a repeat procedure for hemostasis. AT status did not significantly impact the risk of having 1 of these more severe PBE’s. We found no significant difference in the rate of PBE’s with regard to which particular type of AT patients were prescribed. A larger study is needed to determine the impact of particular antithrombotic medications compared to others.
We included both rubber band ligations and excisional hemorrhoidectomies. When we compared PBE outcomes in these groups, we found that for patients on AT, those undergoing excisional hemorrhoidectomy were more likely to have a PBE than those undergoing rubber band ligation. There was no significant difference in number of PBEs between patients on DOACs vs antiplatelet therapy only (Table 4). It was surprising to us that patients were more likely to have a PBE following an excisional hemorrhoidectomy vs a rubber band ligation, because as noted in the methods section some patients were told to hold their antiplatelet therapy for rubber band ligations only. Future studies could explore the question of whether antiplatelet therapy should be held before excisional hemorrhoidectomies, rubber band ligations, or both.
Interestingly, we found that while the majority of patients in our study prescribed AT were males, the majority of patients with PBE’s on AT were females. While these results were statistically significant, it is yet unknown whether this should have any clinical significance. One could assume that a biological gender difference is attributable to the findings, such as hormonal differences, body weight or pharmacologic metabolism, but these explanations are nothing more than theoretical. There are known differences in response to anticoagulant treatment, 3 and perhaps this plays some role in our results. The PAUSE study showed that females were more likely to have higher levels of residual DOAC post interruption than males, perhaps explaining some of the differences in response. 13 Further investigation with a larger study is needed to further investigate this finding.
The retrospective nature of this study is an inherent weakness. Chart review revealed a nearly complete lack of record of patient-specific perioperative management of antithrombotic medications. Fortunately, our study involved only 6 colorectal surgeons, who all practice standard perioperative management of AT, although there are slight variations amongst the group. However, there are undoubtedly certain patient characteristics (ie, renal function, thromboembolic risk, history of bleeding complications, etc.) that occasionally impact perioperative AT medication decision making. Another data point we attempted to collect on chart review was the indication for AT, but that data was also unavailable in 43.9% of cases.
This single institution study examined cases performed by only 6 colorectal surgeons, and this is a weakness when attempting to apply the data to the surgical community at large. All 6 surgeons perform similar ligation techniques and consistently performed closed excisional hemorrhoidectomies. Interestingly, 4 out of 6 of the surgeons in this study do not routinely hold antiplatelet therapies prior to or after hemorrhoid procedures, while the other 2 do typically hold antiplatelet therapies for 7 days preoperatively and postoperatively. Our data did not reveal any association between said differences in perioperative management and differences in PBE’s amongst the 6 surgeons. This may indicate that continuation of antiplatelet therapy for minor hemorrhoid procedures can be considered relatively safe, especially if the patient has a high risk of cardiac or thromboembolic event.
While this study demonstrates an increased risk of PBE’s after hemorrhoid procedures for patients on AT, most of the bleeding events were minor and did not require admission or any additional procedure for hemostasis. When considering only the more severe PBE’s, there was no significant association with AT status. A large, multicenter, prospective cohort study could be beneficial for determining what factors increase the risk for clinically significant PBE’s. Such a study may elucidate if specific antithrombotic medications are more associated with PBE’s and if any particular perioperative management regimen would be recommended to reduce postoperative bleeding risk.
Footnotes
Author Contributions
Dean, Katherine Dean, MD - Acquisition of data, analysis and interpretation of data, drafting of manuscript and critical revision for important intellectual content, final approval of manuscript for submission. Haritha Pavuluri, BS - Acquisition of data, critical revision of manuscript for important intellectual content, final approval of manuscript for submission. Sarah Fox, MD - Conception and design, acquisition and interpretation of data, critical revision of manuscript for important intellectual content, final approval of manuscript for submission. Ben Watson, MD – Drafting and critical revision of manuscript for important intellectual content, final approval of manuscript for submission. Xiyan Tan, PhD – statistical analysis, final approval of manuscript for submission. Grace Wallenborn, PhD – Drafting and critical revision of manuscript for important intellectual content, final approval of manuscript for submission. George, George Blestel, MD - Conception and design, interpretation of data, critical revision of manuscript for important intellectual content, final approval of manuscript for submission
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.