
Abstract
Background
There is a paucity of data comparing open, robotic, and laparoscopic approaches on unilateral, non-recurrent inguinal hernias. Our study presents a large, retrospective triple-arm outcome analysis between robotic, laparoscopic, and open unilateral, non-recurrent inguinal hernia repairs at a single institution.
Methods
706 patients who underwent elective, non-recurrent inguinal hernia repair performed by 8 general surgeons at a single institution from 2016 to 2019 were reviewed retrospectively. Patient baseline characteristics, operative times, resident involvement, and postoperative outcomes were analyzed for all repair types. A cost analysis of the different procedures was performed.
Results
There were 305 laparoscopic repairs, 207 robotic repairs, and 194 open repairs. Open and laparoscopic repairs were performed on patients who were older (p =< .001) and with a higher Charlson Comorbidity Index (p =< .001). Patient BMI was higher in minimally invasive repair than open repair (P = .021). There were no significant differences in complication rates on pairwise analysis. Robotic and open repairs had significantly longer operative times than laparoscopic repairs (P < .001). There was less resident involvement in robotic repair than with the other approaches (P < .001). Resident involvement was associated with shorter OR times (P = .001) and no significant difference in postoperative complications. There was a trend over the study period toward faster operative times and more robotic repair. Robotic repair is the most expensive repair, followed by laparoscopic and open repairs.
Conclusion
All 3 repair techniques can be performed without significant differences in outcomes. The technique utilized should be based on surgeon preference and patient characteristics.
Key Takeaways
• There is no significant difference between open, laparoscopic, and robotic inguinal hernia repairs with respect to complications. • Open and robotic inguinal hernia repairs took significantly longer than laparoscopic inguinal hernia repair. • Resident involvement was associated with shorter operative time. • Resident involvement did not have significant impact on complication frequencies. • Robotic repair is most expensive, followed by laparoscopic and open repairs.
Introduction
Inguinal hernia repair is one of the most common general surgery procedures with an estimated 20 million cases performed annually worldwide. 1 Currently, there are four common approaches: open repair, transabdominal preperitoneal repair (TAPP), total extraperitoneal repair (TEP), and robotic transabdominal preperitoneal repair. 2 Laparoscopic inguinal hernia repair has increased substantially over the last decade with current studies showing similar recurrence rate, less postoperative pain, and faster recovery relative to open repair. 3 Despite these favorable outcomes, laparoscopic approach is associated with a steep learning curve with studies noting higher recurrence rates and complications during the learning curve. 4 Within the laparoscopic approach, a meta-analysis comparing TAPP and TEP showed no significant differences in recurrence rates and chronic pain. 5 The robotic approach has been theorized to improve outcomes given its additional degree of dexterity, improved visualization and ergonomics. Previous studies and the latest randomized controlled trial comparing robotic and laparoscopic TAPP approaches showed no significant difference in wound events, readmissions, pain, and quality of life but showed an increased operative time and cost in the robotic group. 6 One of the other potential benefits of robotic approach is the quicker learning curve compared to the laparoscopic approach. 7 Although there are several studies comparing one approach vs another, there is a paucity of data comparing all three approaches of inguinal hernia repair in a single study in a unilateral, non-recurrent setting. Our study presents a large, retrospective triple-arm outcome analysis between robotic, laparoscopic, and open repair of unilateral, non-recurrent inguinal hernia at a single institution. Our main goal is to examine any differences in patient characteristics, outcomes, and operative times. Our secondary goal is to examine the influence of resident involvement on operative time in the three approaches.
Methods
All patients aged 18-80 years old who underwent elective, unilateral, non-recurrent inguinal hernia repair were captured using based on Current Procedural Terminology codes (49 505, 49 507, and 49 650) from 2016 to 2019 following approval from Spectrum Health’s Institutional Review Board. Patients who had a recurrent hernia of the ipsilateral side, combined procedures, or emergent surgery were excluded. Patient baseline characteristics (age, sex, BMI, ASA, Charlson Comorbidity Index (CCI), smoking status, previous abdominal surgery, previous contralateral repairs) were recorded. Primary outcomes included operative time, intraoperative complications (conversions, immediate complications), and postoperative complications (recurrence, unplanned admissions, surgical site infections, seromas, hematomas, inguinodynia). Secondary outcomes included resident involvement during the case as well as their postgraduate year of training. The open and laparoscopic approaches were performed by eight surgeons at a single institution, with four of the eight also performing the robotic approach. The surgical approach was based on surgeon preference. Recurrences and complications were identified via individual chart reviews noting assessments from postoperative follow up visits, emergency room visits, additional primary care visits related to the repair, and any abnormal radiographic findings on subsequent imaging performed. The follow up period spanned the entirety of our study period until data collection in 2020–2021. Inguinodynia was defined as postoperative pain persisting more than 3 months after surgery from chart review with postoperative follow up visits. Early postoperative pain was defined as ipsilateral groin pain within 30 days of procedure.
Data was collected securely with REDCap. Patient baseline characteristics and postoperative outcomes were examined by Kruskal Wallis or Simple Chi Square (χ2) tests and Fisher’s Exact tests when appropriate. Benjamini-Hochberg method was used for pairwise comparison between procedure types. Resident involvement in the case was assessed and sub-group analysis performed to examine significant differences in operative time and postoperative outcomes. Linear regression was used to examine the relationship of operative time and operative volume over the study period. A cost analysis of open, robotic, TAPP, and TEP repairs was performed by taking a subsample of 10 patients to obtain an average total hospital cost for each of the four procedures.
Results
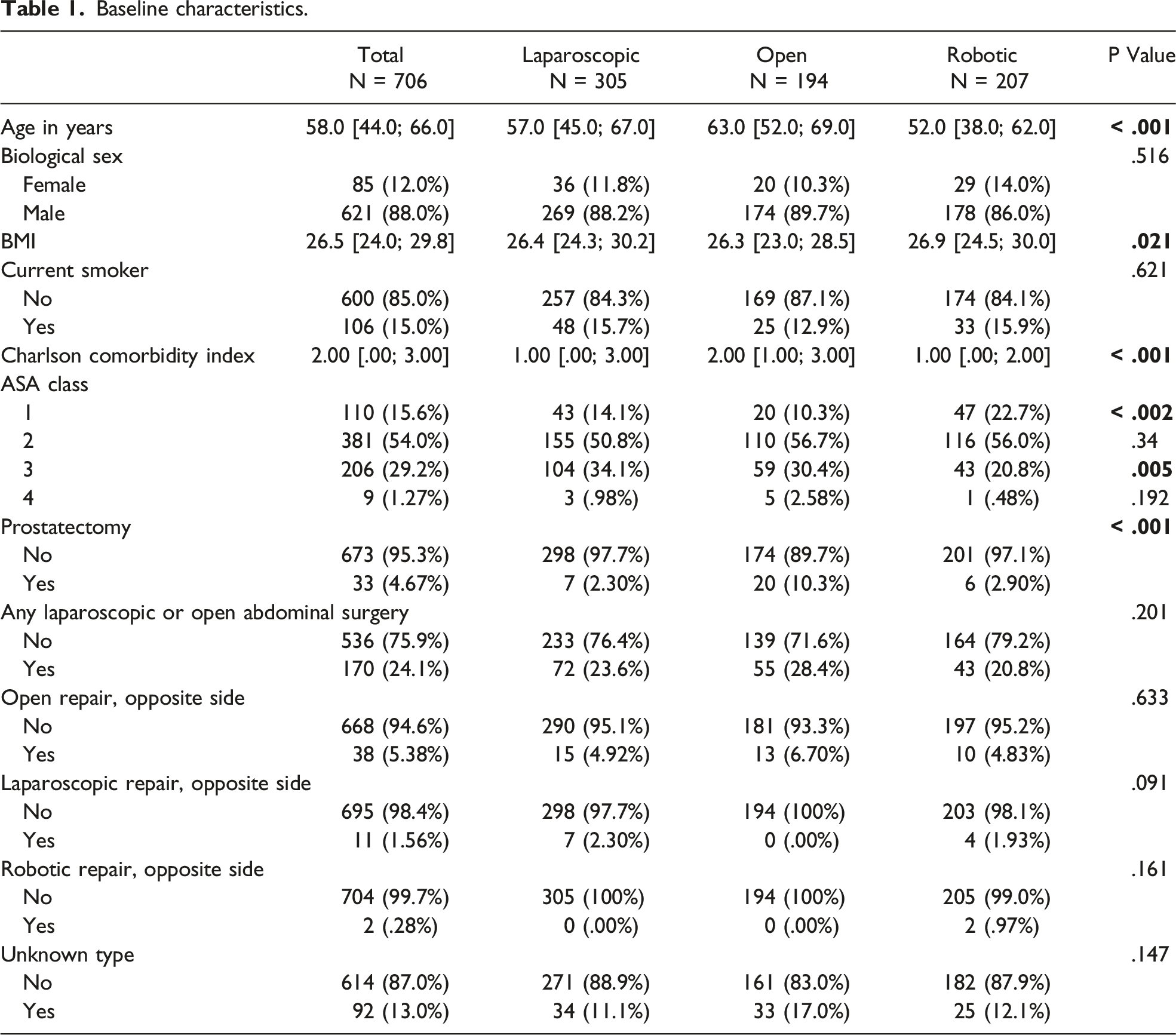
Baseline characteristics.
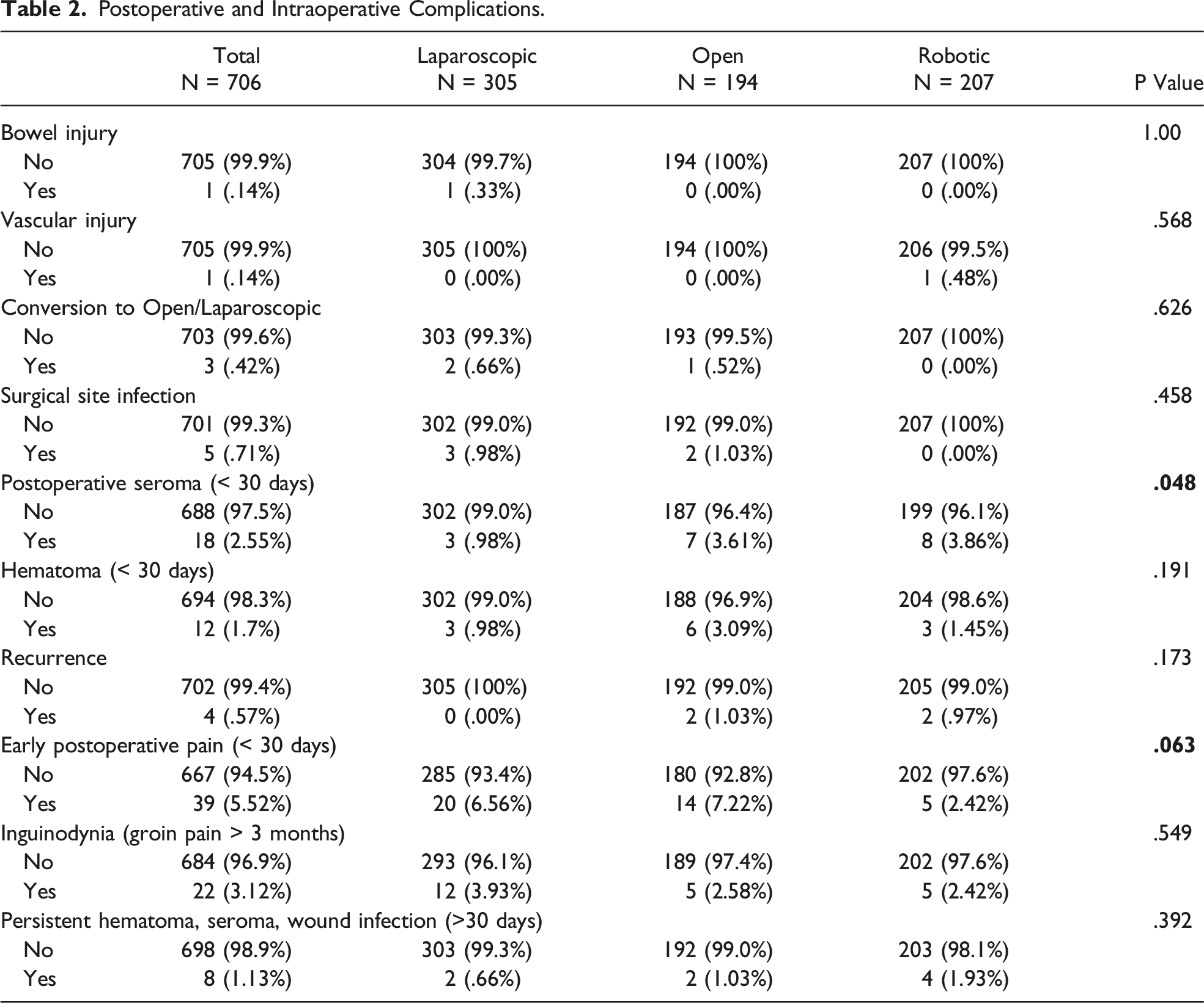
Postoperative and Intraoperative Complications.
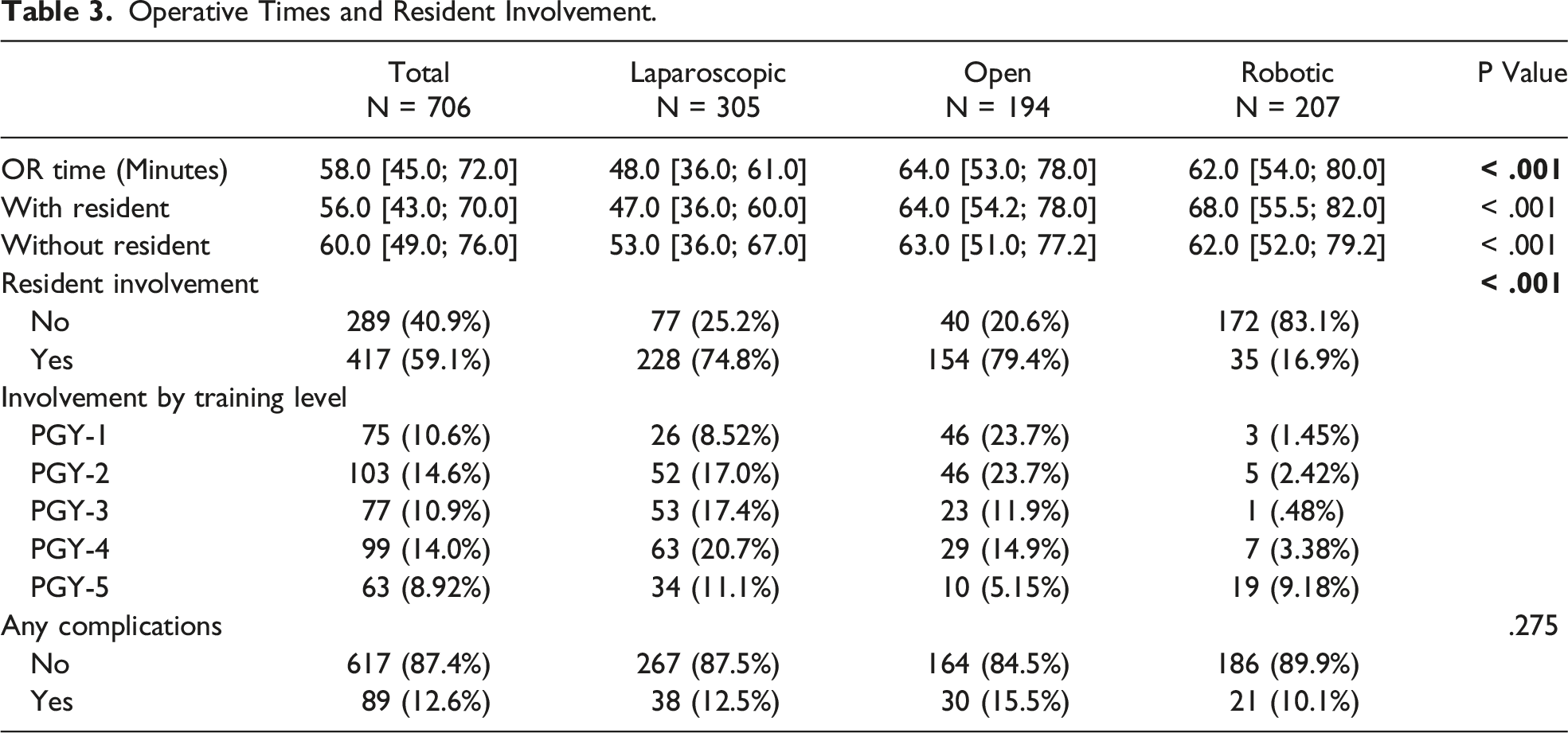
Operative Times and Resident Involvement.
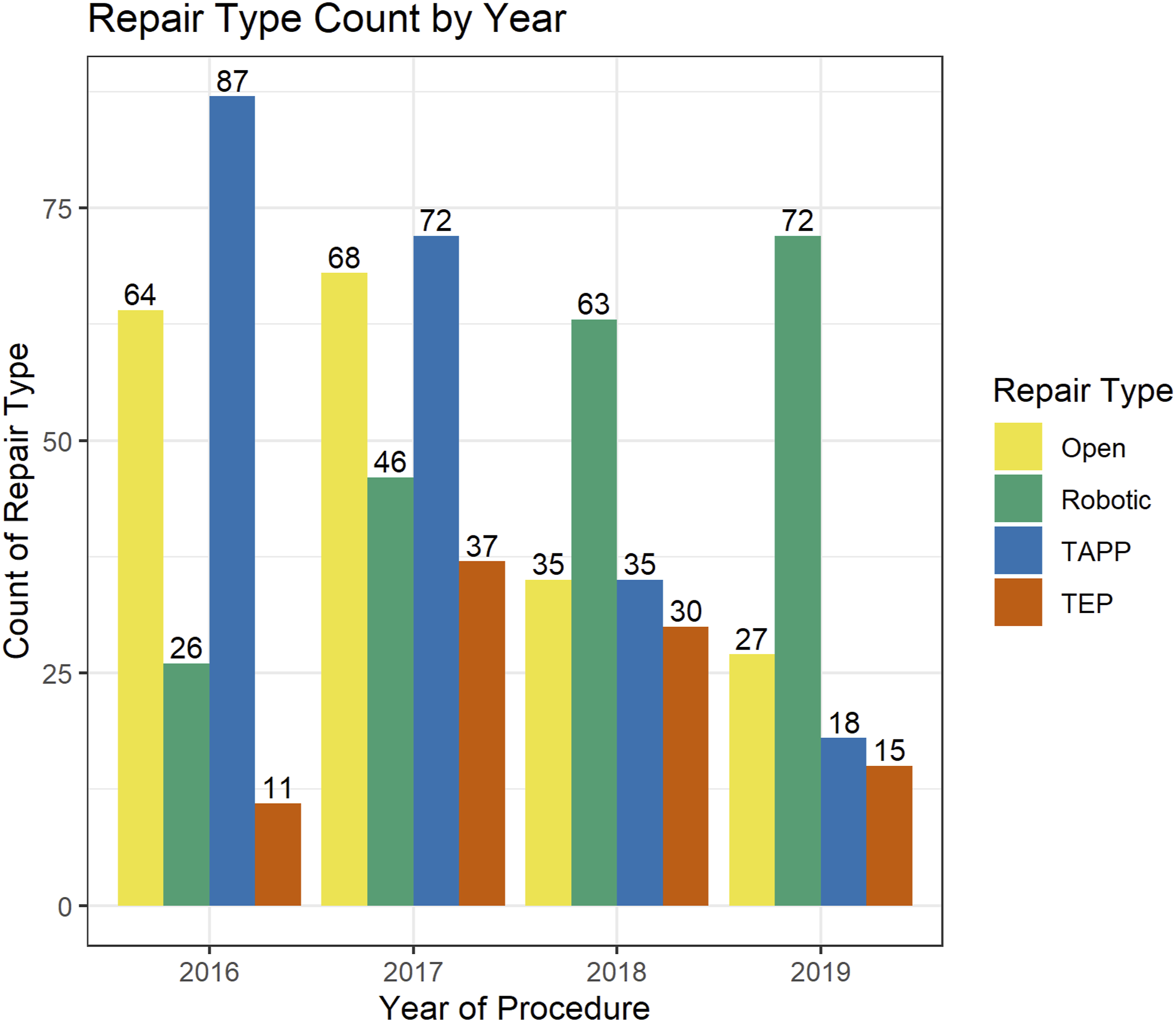
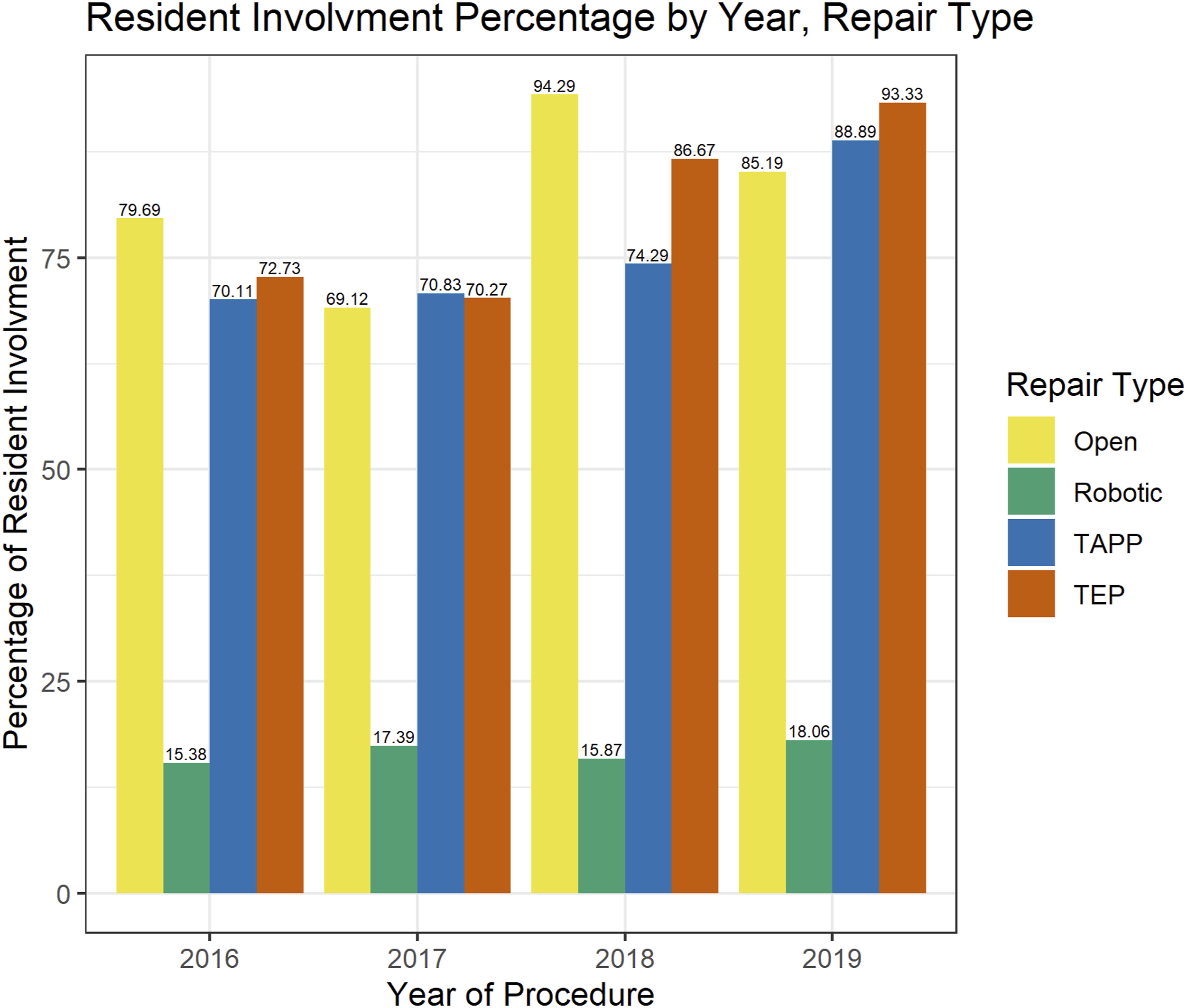
Over the course of the study period, there was a trend towards faster operating times in TAPP and robotic approaches represented in Figure 1 (4.1 minutes and 8.7 minutes on average per year based off of linear regression from 2016 respectively, P = .0017 and P < .0001). The number of repairs per approach performed each year also showed an increase in robotic repairs and open repairs (P < .001 and P < .001, respectively), a decrease in TAPP repairs (P < .001), and no statistically significant trend in TEP repairs (P = .067) on χ2 trend test (Figure 2). Resident involvement in different approaches over the study period was shown in Figure 3. There was a trend toward more involvement in TEP approaches (P = .0449, χ2 trend test) but not in the other approaches. OR time by year per approach. Operative time for open, robotic, TAPP, TEP repairs by year. Repair type count by year. Open, robotic, TAPP, or TEP repair type count performed by year. Resident involvement by year. Resident involvement percentage of overall number of unilateral, non-recurrent inguinal hernias performed by year.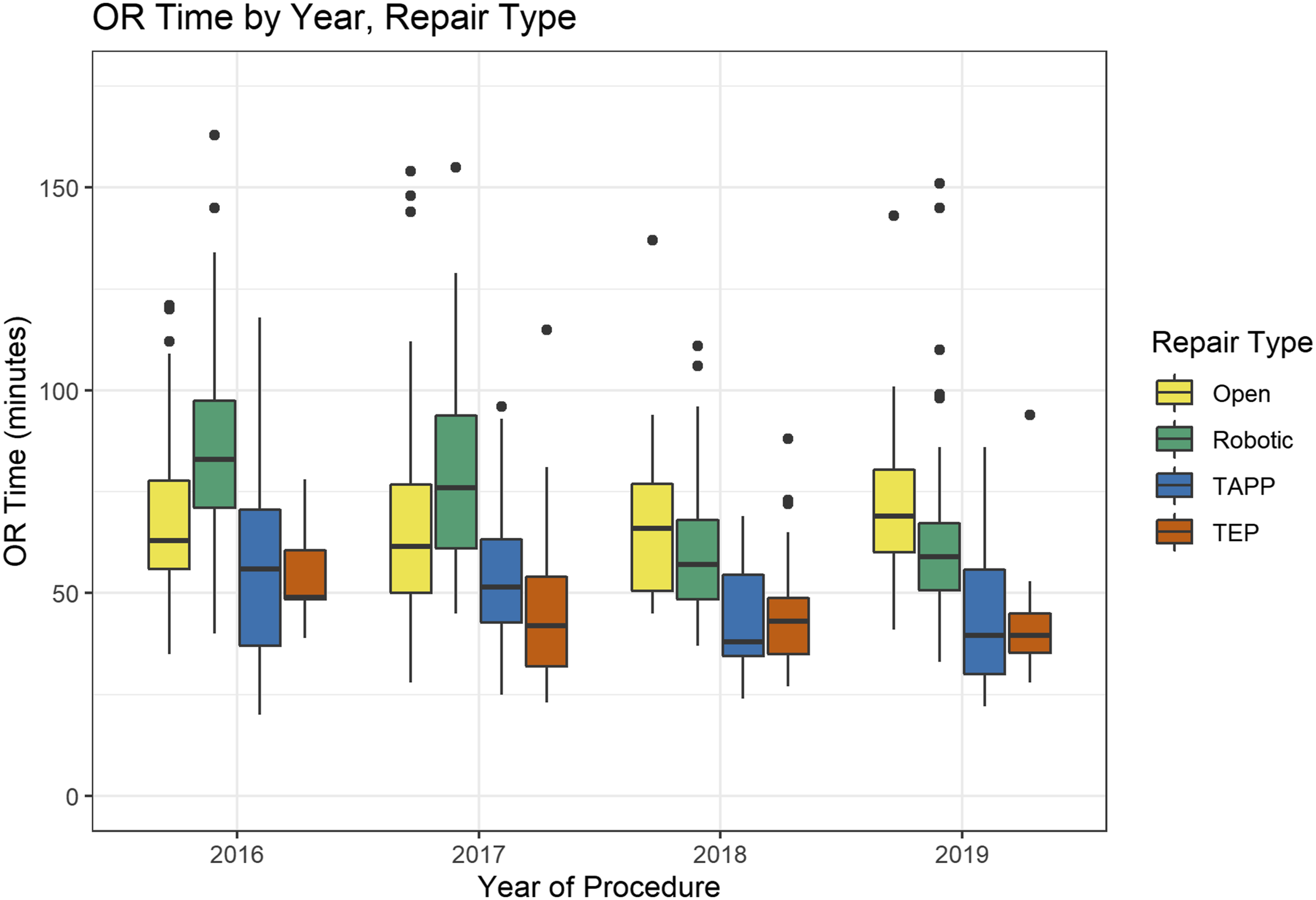
Cost analysis of the four repair types demonstrated that robotic repair is most expensive with an average cost of $19,614. TEP and TAPP repairs are next with average costs of $13,374 and $12,931, respectively. The average cost of an open repair is $12,615, making it the least expensive repair.
Discussion
Our study is in concordance with current guidelines and literature as there was no significant difference between the three arms in terms of patient outcomes.1,3,6 However, there were significant differences within patient characteristics with regard to the approach offered despite excluding bilateral and recurrent hernias. Open repair tended to be performed on patients of older age, lower BMI, and a higher CCI, whereas the minimally invasive approach tended to be performed on younger, healthier patients or patients with higher BMIs. An open approach may be preferred for older patients or patients with higher CCI to avoid general anesthesia with abdominal insufflation despite studies showing no increased risks of laparoscopic approach in octogenarians.8,9 Open approach also may be preferred for patients with large or complex inguinal scrotal hernias. There may also be surgeon preference towards selecting robotic approach for younger and thinner patients for the presumed benefits of avoiding surgical tack usage, although current literature does not show an association between tack usage and inguinodynia. 10 Our study, however, showed that our group of surgeons had a preference toward using the minimally invasive approach for higher BMI patients. Younger patients may also preferentially request a minimally invasive approach when offered. One study observed that younger age was a predictive factor toward laparoscopic approach, along with gender, race, insurance type, as well as surgeon annual volume, hospital size, and hospital region. 11
There were two interesting observations in our study regarding postoperative seromas and early postoperative pain. There was a significant difference during triple-arm analysis of postoperative seromas between all three groups that was not statistically significant on further pairwise analysis. This could be due to surgeon preference in tackling complex inguinal scrotal hernias with a robotic or open approach as opposed to laparoscopic approach. Due to the retrospective nature of this study, seroma occurrence could also be missed or not mentioned within documentation or subsequent imaging. Seromas can be quite variable in clinical manifestation and might not be clinically significant. 12 The other observation was postoperative pain between the three arms. There appeared to be a trend toward statistical significance with lower rate of early postoperative pain in the robotic approach compared to either laparoscopic or open approach. This may be due to the use of suture in the robotic approach as opposed to tacks for mesh fixation and peritoneal flap closure. However, despite limitations with follow up and lack of quantification for severity of postoperative pain, these occurrences were collected in the same method for all three arms. On our review of the literature, there has not been a randomized study focusing on early postoperative pain or inguinodynia for robotic approach but many studies have been done regarding the effects of tack usage and mesh fixation with comparable long-term outcomes.10,13,14 The first randomized controlled trial comparing robotic vs laparoscopic transabdominal approach showed no significant difference in surgeon ergonomic benefits, postoperative pain and other patient outcomes. 6 The trial however did reinforce the known issues of higher cost and longer operative times with robotic approach and questioned its justifications especially for surgeons who already performed repairs laparoscopically. 6 Our cost analysis confirms that robotic approach is significantly more expensive than laparoscopic approach, which is more expensive than open approach. Despite the purported benefits of robotic and laparoscopic approaches, international experts agreed that there is no standard repair technique for groin hernias and that surgical techniques should be tailored to the surgeon’s expertise and patient factors. 1
The operative times observed in this study showed a significantly longer operative time with robotic approach when compared to laparoscopic approach, which was similar to current published literature.2,6 Interestingly, open approach was also found to take significantly longer when compared to laparoscopic approach. Even though this study included only unilateral, non-recurrent inguinal hernias, the longer times for open approach may be attributed to selection bias, with larger and more complex hernias being preferentially performed via an open approach. However, there have been no studies on whether hernia size or degree of incarceration is a predictor for choosing a particular approach outside of bilateral or recurrent inguinal hernias. Sub-group analysis revealed a reduction in operative time in robotic and laparoscopic approaches over the years, which supported findings from previous studies looking at their respective learning curves.7,15
Comparing outcomes among the minimally invasive approaches can be challenging as it is dependent on where a surgeon is along their learning curve.7,16 Our study showed as robotic repairs increased there was a concomitant reduction in TAPP repairs. This could potentially make it more difficult for trainees to learn the TAPP technique especially with its well-documented, long learning curve. 1 Resident involvement was noted to decrease overall operative time in our study; however, only 16.9% of robotic repairs included a resident. This may be attributable to attending surgeons recently adopting the robotic platform or the lack of teaching consoles in the outpatient surgical center. The absence of a standardized resident robotic curriculum could have contributed to low involvement as well.
This study was limited by the retrospective design, use of subjective data from postoperative visits, and lack of long term follow up. The assessment of recurrence and pain were based predominantly on subjective data from postoperative notes and subsequent imaging, which all potentially could be under-reported if patients were lost to follow up. Some of the surgeons within the study were still within their learning curve for robotic inguinal hernia repair and thus may add a confounder to the study. This study was also limited by lack of objective data on hernia size or complexity that may have created selection bias. Once surgeons have surpassed their learning curves an additional focus of research includes hernia size analysis, pain assessment, and long-term follow up. Further studies should consider a prospective comparison of the four different repair types to allow for standardization in pre-operative and postoperative assessment, with implementation of patient satisfaction surveys. Given the relatively low complication rate for each repair, the large number of patients that would need to be enrolled to allow for a significant difference would likely not be met, and thus future studies could consider analyzing outcomes with a cumulative complication variable or performing propensity-matching to minimize any confounding effects or biases.
Conclusion
Our study showed no significant differences in outcomes between the three approaches, however, there was a trend toward significance with reduced early postoperative pain in robotic repairs. However, this trend was not present when analyzing for inguinodynia. While one approach was not better than another based on outcomes, laparoscopic approach was significantly quicker than robotic or open approaches at our institution and was not nearly as expensive as robotic approach. Regardless, our large, triple-arm study supported the conclusion made by prior studies that the best approach should be based on the surgeon’s experience and comfort with that approach as well as patient factors and preference.
Footnotes
We would like to thank Dr Carlos Rodriguez, Dr Jeffrey Gawel, Dr Lora Silverman, Dr Thomas Martin, Dr Ryan Conway, Dr Gabriel Gallardo, and Dr Kenneth Minks for allowing us to review their cases and include them in our study. We would like to thank Matthew Lypka for assistance with statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.