
Abstract
Background
Studies of robotic lobectomy (Robot-L) have been performed using data from high-volume, specialty centers which may not be generalizable. The purpose of this study was to compare mortality, length of stay (LOS), and cost between Robot-L and thoracoscopic lobectomy (VATS-L) using a nationally representative database hypothesizing they would be similar.
Methods
The Premier Healthcare Database was used to identify patients receiving elective lobectomy for lung cancer from 2009 to 2019. Patients were categorized as receiving Robot-L or VATS-L using ICD-9/10 codes. Survey methodology and patient level weighting were used to correct for sampling error and estimation of a nationally representative sample. A propensity match analysis was performed to reduce bias between the groups. Primary outcome of interest was in-hospital mortality. Secondary outcomes were LOS and patient charges.
Results
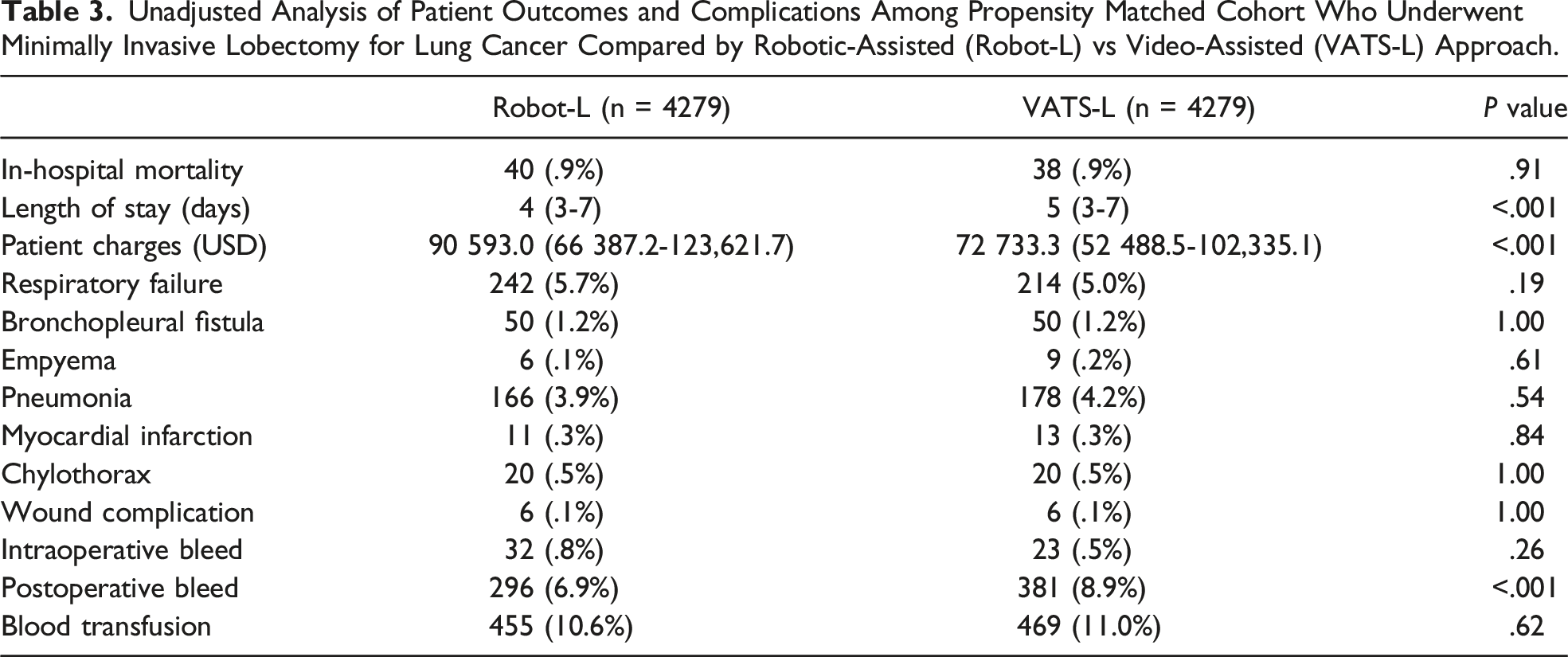
Among 62 698 patients, 19 506 (31.1%) underwent Robot-L and 43 192 (68.9%) underwent VATS-L. Differences between the groups included age, race, comorbidities, and insurance type. A propensity matched cohort demonstrated similar in-hospital mortality for Robot-L and VATS-L (.9% vs .9%, respectively, P = .91). Patients who underwent Robot-L had a shorter LOS (4 vs 5d, respectively, P < .001) but higher patient charges (90 593.0 vs 72 733.3 USD, respectively, P < .001).
Conclusions
In a nationally representative database, Robot-L and VATS-L had similar mortality. Although Robot-L was associated with shorter hospitalization, it was also associated with excess charges of almost $20,000. As Robot-L is now the most common approach for lobectomy in the U.S., further study into the cost and benefit of robotic surgery is warranted.
Introduction
Although surgery remains the gold standard for treatment of patients with lung cancer, controversy exists regarding the optimal surgical approach for lobectomy. Since the introduction of minimally invasive surgery, thoracoscopic lobectomy (VATS-L) has been widely adopted as a safe approach for the treatment of lung cancer. 1 Multiple studies have demonstrated that VATS-L has fewer complications and improved outcomes compared to the traditional open approach.2-5
In more recent years, robotic lobectomy (Robot-L) has become increasingly popular as an alternative minimally invasive approach to VATS-L. Studies comparing Robot-L and VATS-L have shown similar or improved postoperative outcomes regarding mortality and complication rates for patients undergoing segmentectomy or lobectomy for lung cancer.5-13 Although these findings suggest that Robot-L is a safe alternative to VATS-L, most of these studies include data from high-volume thoracic surgeons performed at large, academic centers, which may not be representative of the entire population. Particularly there is a lack of data from patients receiving care at community hospitals which represent an important proportion of lung cancer patients within our country.
The purpose of this study was to compare in-hospital mortality, length of stay (LOS), and total patient charges between Robot-L and VATS-L using a nationally representative database. We hypothesized that patients undergoing Robot-L for lung cancer would have similar outcomes compared to VATS-L.
Patients and Methods
Data Source
The Premier Healthcare Database (PHD) was used to analyze patient outcomes of minimally invasive lobectomy for lung cancer based on robotic or thoracoscopic approach. The PHD is a nationally representative database that contains de-identified clinical data from more than a thousand participating hospitals capturing patient billing records, costs, and coding histories. It is comprised of data from more than 1 billion patient encounters, which equates to approximately twenty-five percent of all inpatient admissions in the United States. The database is maintained by Premier, Inc. (Washington, D.C.) and contains hospital admissions, hospital characteristics, surgeon characteristics, payer information, Diagnosis Related Groups, primary and secondary International Classification of Diseases (ICD) diagnosis and procedure codes, current procedural terminology codes, and resource utilization (hospital length of stay and in-hospital mortality).
Patient Selection
The PHD was queried for all adult patients with lung cancer who underwent minimally invasive lobectomy from 2009 to 2019. Minimally invasive lobectomy was defined as robotic (Robotic-L) or video-assisted thoracoscopic (VATS-L) approach. Patients less than 18 years old and those with a clinical diagnosis of metastatic cancer were excluded. Patients were categorized as receiving Robot-L or VATS-L based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) or ICD-10-CM procedure codes.
Outcome Measure
The primary outcome of interest was in-hospital mortality based on minimally invasive approach. Secondary outcomes included total patient charges, LOS, and postoperative complications. Total patient charges reflect the charge of the patient’s entire hospitalization after surgery.
Statistical Analysis
Survey methodology was used to correct for sampling error. Patient level weighting derived from the PHD was used to estimate a nationally representative sample. Categorical variables were compared using survey weight-adjusted Pearson’s
To address potential improvement in the quality of surgery with the newer da Vinci Xi robot system, a subgroup analysis comparing more recent robotic procedures was performed. Patients who underwent Robot-L were categorized as Xi Robot-L using ICD-10-CM procedures codes under assumptions that the platform used was based on the time that the procedure was performed. The Xi system became available in April 2015 and ICD-10-CM coding began in October 2015. Therefore, patients who had their robotic lobectomy coded with ICD-10-CM procedure codes were used as a surrogate for Xi robot use.
Statistical analysis was performed using STATA MP (Version 16.0, College Station, TX). Statistical significance was set at a P value ≤ .05. Since all patient-related data in the PHD is aggregated, de-identified, and HIPAA-compliant, this study was determined to be exempt from Institution Review Board review.
Results
In total, there were 14 155 patients who met inclusion criteria representing an estimated population size of 62 698 patients: 43 192/62 698 (68.9%) underwent VATS-L and 19 506/62 698 (31.1%) underwent Robot-L. Figure 1 represents the annual proportion of each minimally invasive approach for lung cancer lobectomy during the study period. From 2009 to 2019, the proportion of lung cancer lobectomies performed by robotic approach increased from 4.1% to 60.9%. The proportion of all adult patients who underwent minimally invasive lobectomy for lung cancer compared by robotic-assisted (Robot-L) vs thoracoscopic-assisted (VATS-L) approach from 2009 to 2019.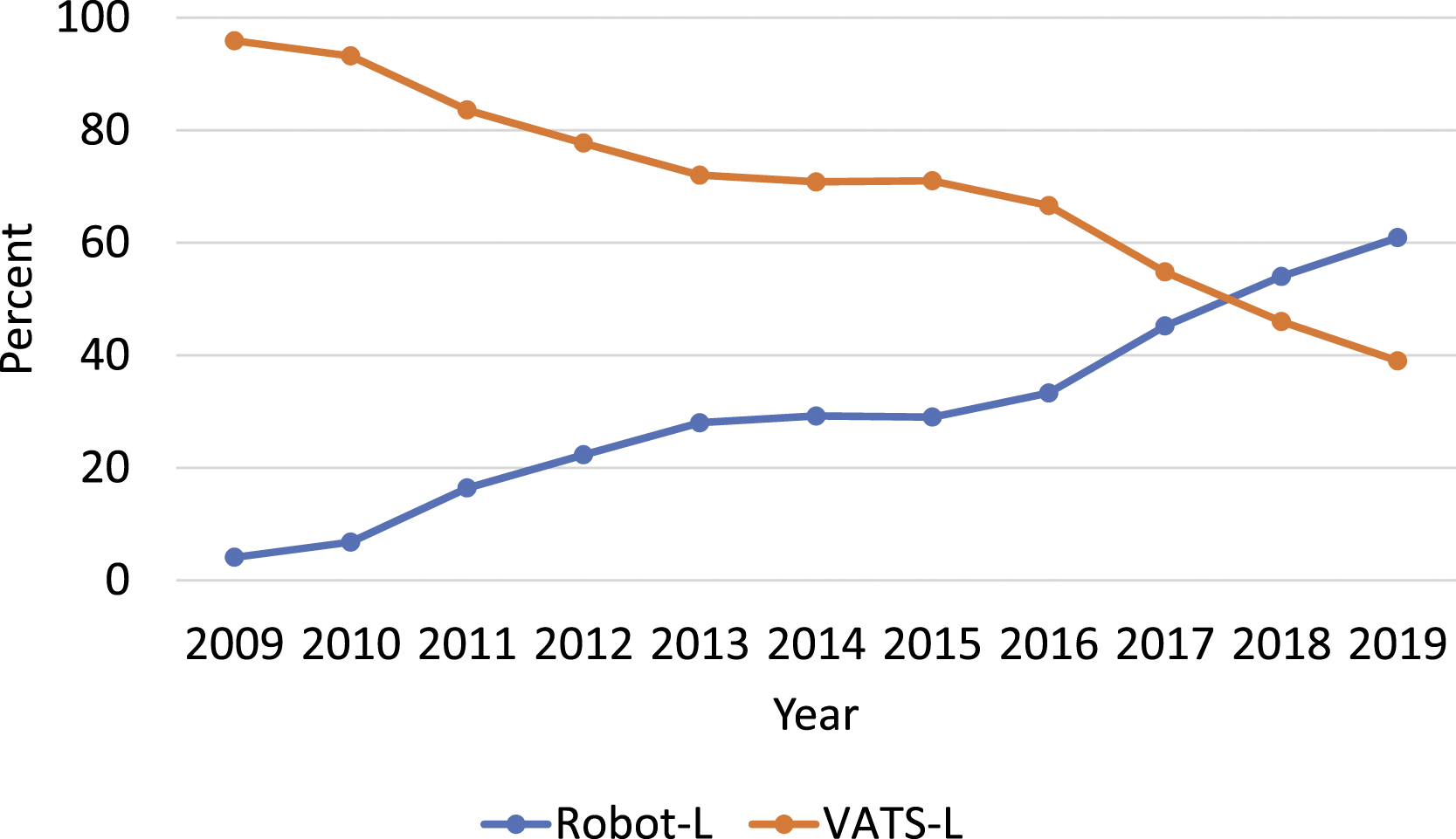
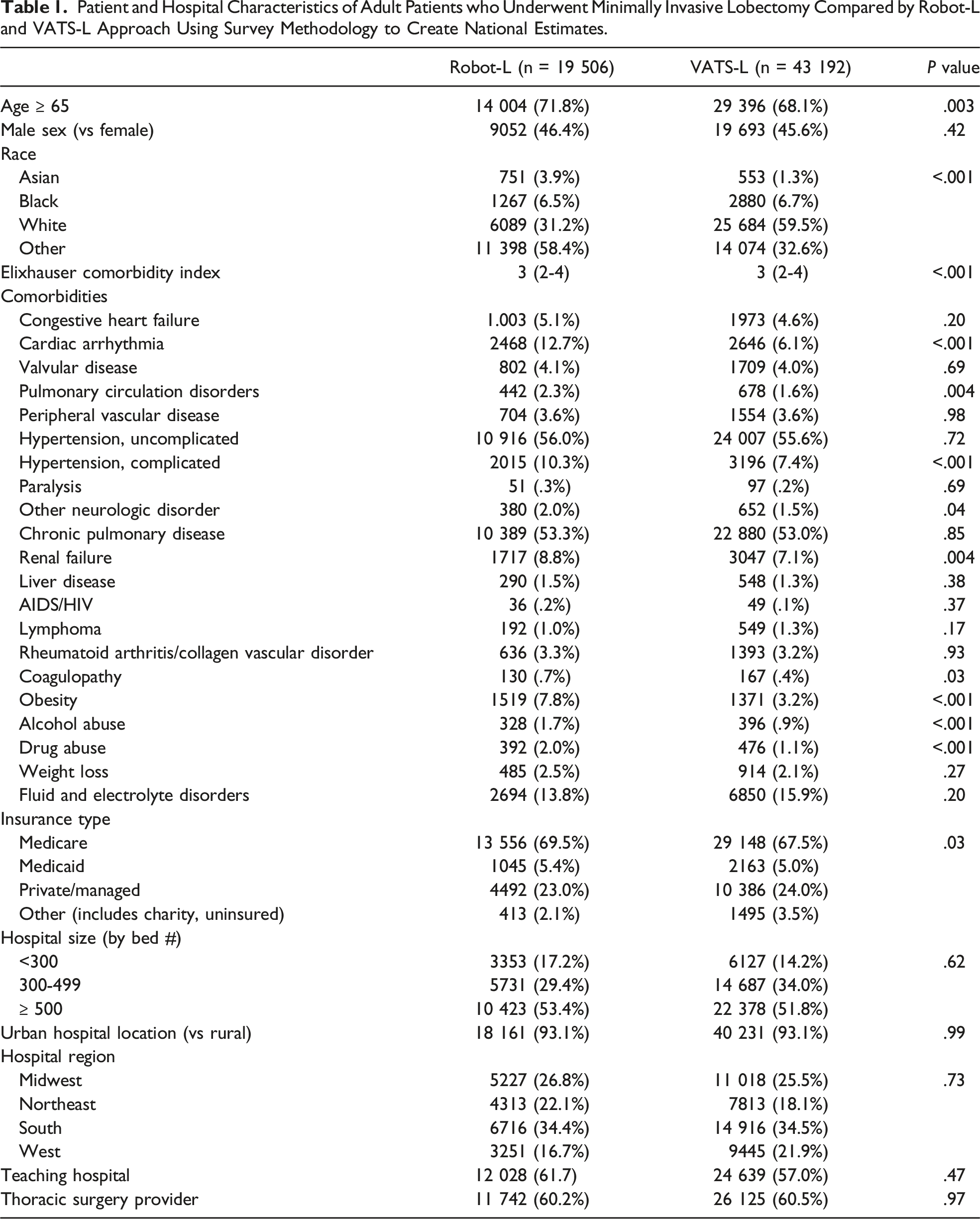
Patient and Hospital Characteristics of Adult Patients who Underwent Minimally Invasive Lobectomy Compared by Robot-L and VATS-L Approach Using Survey Methodology to Create National Estimates.
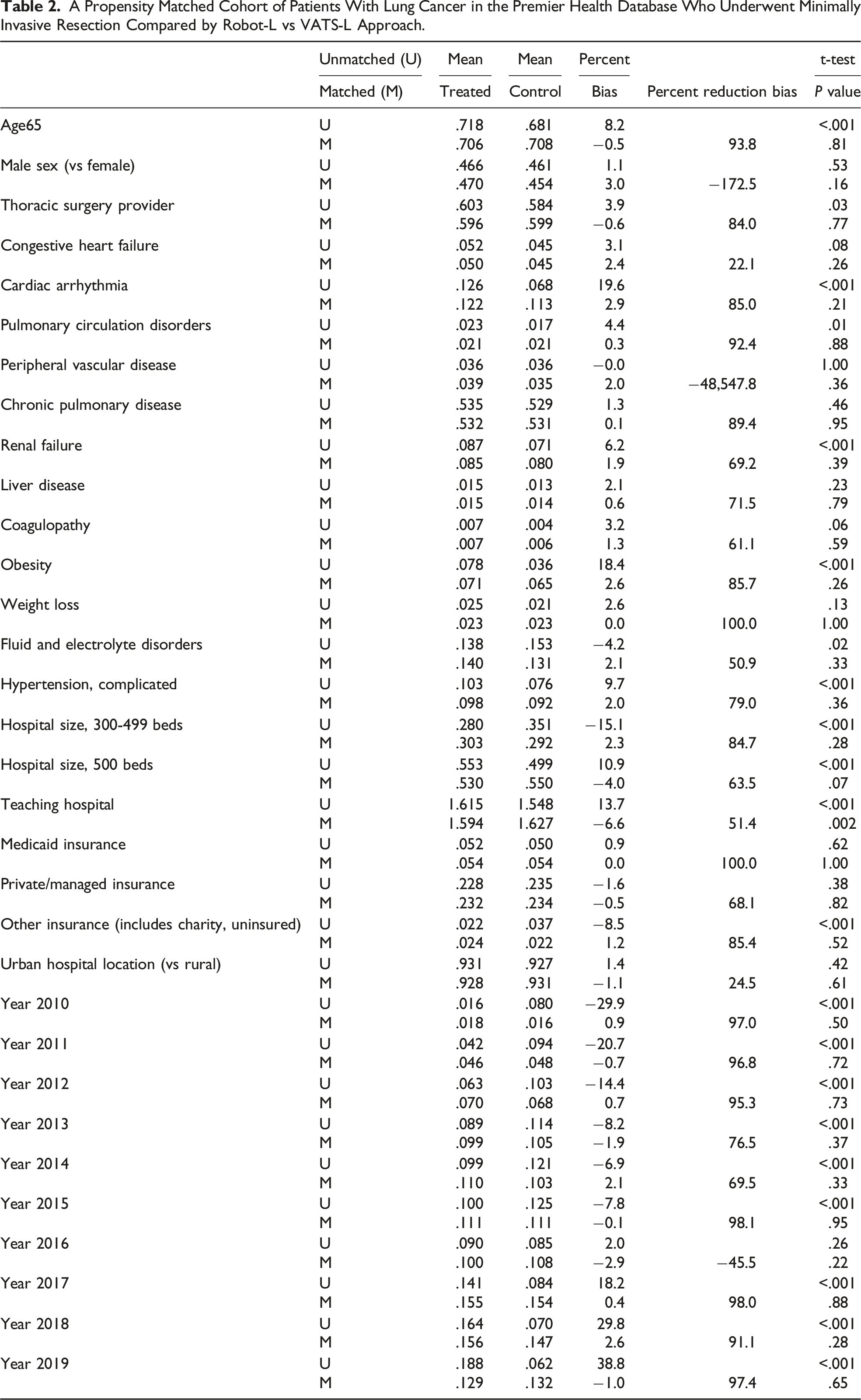
A Propensity Matched Cohort of Patients With Lung Cancer in the Premier Health Database Who Underwent Minimally Invasive Resection Compared by Robot-L vs VATS-L Approach.
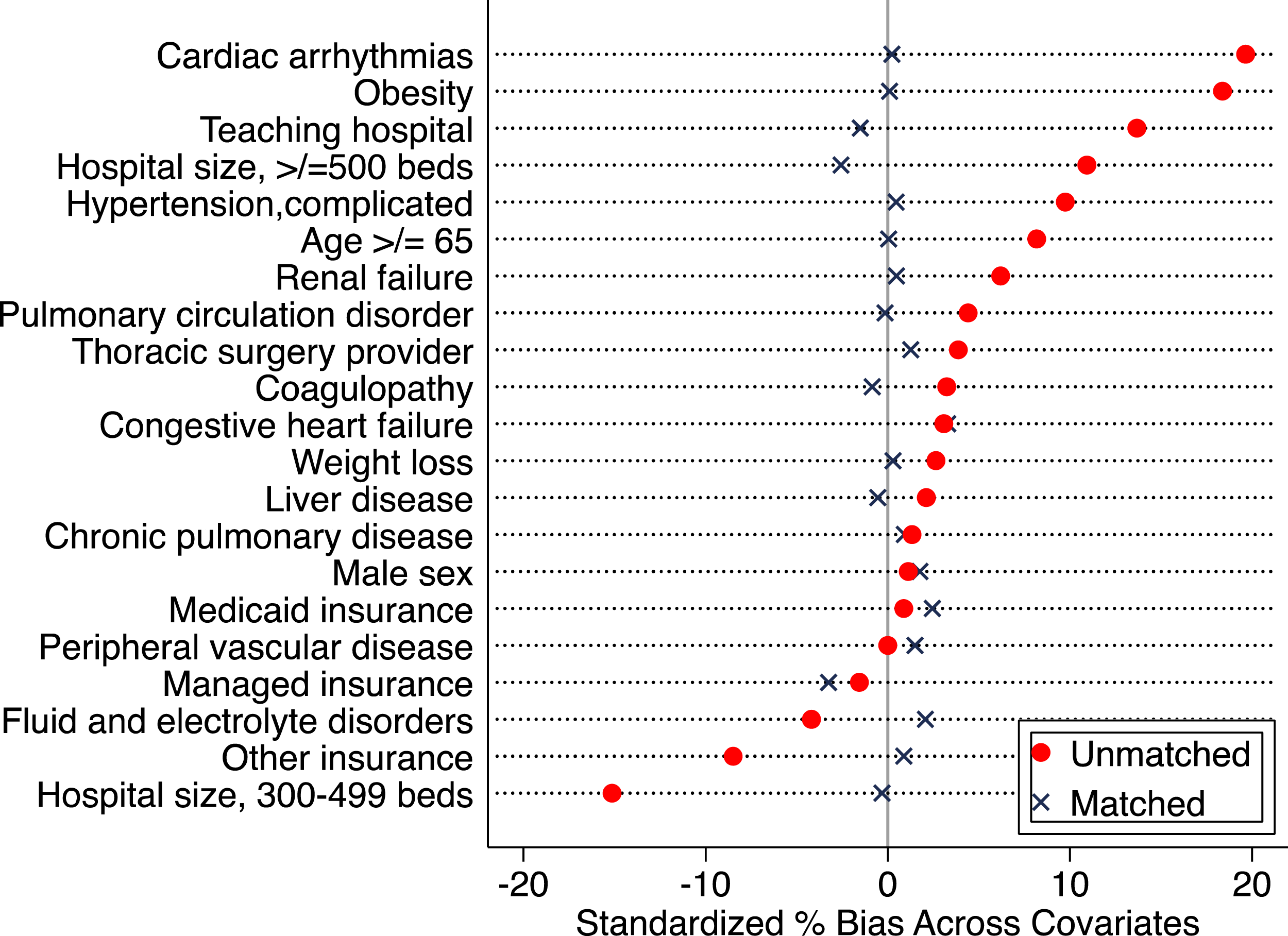
The standardized difference before (blue circle) and after (red circle) propensity score match.
Unadjusted Analysis of Patient Outcomes and Complications Among Propensity Matched Cohort Who Underwent Minimally Invasive Lobectomy for Lung Cancer Compared by Robotic-Assisted (Robot-L) vs Video-Assisted (VATS-L) Approach.
To assess the potential improvement in quality of surgery associated with the newer da Vinci Xi robot system, a propensity matched subgroup analysis was performed comparing Xi Robot-L and VATS-L using ICD-10-CM procedure coding as a surrogate for Xi robot use (Supplemental Table 2, Supplemental Figure 1). Patient outcomes are represented in Supplemental Table 3. Like the larger cohort, in-hospital mortality was similar between the 2 groups; however, Xi Robot-L was associated with a shorter LOS but increased patient charge. Multivariable Cox analysis showed equivalent in-hospital mortality for both groups (HR 1.00, P = 1.00, data not shown).
Comment
In this study, there was a substantial increase in the use of robotic approach for lung cancer lobectomy over a 10-year span. From 2009 to 2019, the annual rate of minimally invasive lobectomies performed by robotic approach increased by almost 15-fold. Robotic approach is now the most common minimally invasive technique used for cancer lobectomy in the United States. The robust sample size and recent timeframe of our study provides an accurate comparison of outcomes and charges between robotic and thoracoscopic cancer lobectomy while comprehensively representing the patient population of the country.
Prior to this study, the most recent nationally representative study was published in 2017 by Oh et al. which also used the PHD to compare outcomes of robotic, thoracoscopic and open lobectomy using data from 2011 to 2015. 14 Similar to our study, when compared to thoracoscopic lobectomy, patients who underwent robotic lobectomy had a shorter hospital stay and similar postoperative mortality rates. When looking at other outcomes, robotic approach was associated with a lower conversion rate to thoracotomy, lower overall postoperative complication rate, and an increased likelihood of patients being discharged home rather than to a transitional healthcare facility. Although postoperative outcomes investigated in both studies were similar, one of the main differences in our study was that a charge analysis was performed for robotic vs thoracoscopic approach. Another study published in 2014 by Swanson and colleagues used PHD data from 2009 to 2011 to show that robotic lung resection had higher hospital costs and longer operating times without any differences in adverse events compared to thoracoscopic lobectomy. 15
A key difference between our study and prior studies is that our more recent timeframe allowed the inclusion of patients who underwent robotic surgery using the da Vinci Xi robot system. The Xi robot was first introduced in April 2015 and since that time there have been no studies looking at the effect of the Xi system on lung cancer lobectomy outcomes. With advancement in technology, the Xi system is thought to offer technical improvements which may lead to improved surgical outcomes. One study looking at patients who underwent radical prostatectomy suggested better outcomes with the Xi robot compared to the Si robot. 16 Our study is the first to include national data as well as data from the Xi platform. In our subgroup analysis comparing Xi Robot-L to VATS-L, we found similar outcomes as the larger cohort. Compared to VATS-L, Xi Robot-L had equivalent in-hospital mortality, similar complication rates, shorter LOS, and higher patient charges. Although the Xi robot is thought to offer technical advantages compared to the Si system, the lack of differences observed in patient outcomes may be due to evolution in techniques within the Xi system itself such as staplers, which could not be accounted for in this study.
Other studies comparing Robot-L and VATS-L have shown similar outcomes between these two approaches.5-7,10-12 These studies include systemic reviews, meta-analyses, and single institution retrospective reviews which use data mainly collected from high-volume, specialty centers. This differs from our study which used a nationally representative database and may be more generalizable to the current patient population. Furthermore, national data regarding this topic has not been published in more than 5 years. Adoption of robotic technique for any operation requires surgeon frequency and volume to become proficient, making it important to reanalyze this data in a more recent timeframe to determine if outcomes have changed over time.
In addition to safety and efficacy, other important considerations include resource allocation and total cost to the patient. This is especially relevant when outcomes have been shown to be equivalent between approaches. Like our study, literature has shown that the cost of robotic lobectomy greatly exceeds that of thoracoscopic lobectomy.17-19 Although some believe that robotic surgery may prove to be cost effective over time, this was not appreciated over our 10-year study period. In a recent study published by Heiden et al, the authors suggest that factors such as lower conversion rates, shorter operating times, and higher hospital volumes may lead to robotic lobectomy being the most cost-effective approach in the future. 18 Now that robotic approach has been widely accepted and is the most common approach for lung cancer lobectomy, we expected the charge difference to have resolved in our study period, but instead it remained persistent. One hypothesis for the excess charges associated with robotic lobectomy includes increased intraoperative resource utilization of consumables and other equipment such as instruments. 20 This lends itself to further discussion surrounding the benefits and cost of robotic lobectomy.
In contrast, other studies have shown similar cost for robotic surgery compared to more traditional approaches such as VATS and open thoracotomy.21,22 Nguyen et al. used the PHD to evaluate the cost of robotic, thoracoscopic, and open malignant lobectomy from 2008 to 2015 and found that when annual hospital volume was >25 cases, there was no significant cost difference between the 3 approaches. 21 Another study by Kneuertz et al. demonstrated that Robot-L and VATS-L had improved patient outcomes compared to open thoracotomy approach and similar cost. 22 This study, performed at a single tertiary referral center, suggests that robotic surgery may be more likely to be cost effective when performed by specialty trained surgeons at high adoption centers. This is consistent with data demonstrating that a learning curve exists before being able to achieve robotic thoracic surgery competency.23,24
Limitations of this study include that this is a retrospective analysis of a national database. The PHD does not contain data regarding neoadjuvant treatment or clinical stage which may have affected decisions regarding surgical approach and may have impacted outcomes such as in-hospital mortality and length of stay. The PHD also lacks data regarding patient characteristics such as comorbidities and pulmonary function status. However, we do not believe that there is a significant bias between which patients are offered a robotic vs thoracoscopic approach to lung lobectomy based on these clinical factors. Furthermore, studies have shown that patients with significant comorbidities can still safely undergo a minimally invasive approach to lung lobectomy. 25 Since billing data was used to determine surgical approach with an intention to treat model, we are unable to verify that the procedure performed is what was billed. Another important limitation of our study is that we did not have data relating to patient-centered outcomes. Lastly, although total patient charges were analyzed in our study, details of the charge analysis (including individual components of the total charge) are unknown making it difficult to draw conclusions regarding cost effectiveness of either approach.
In conclusion, this study of a nationally representative database demonstrates that robotic lobectomy is now the most common approach for lung cancer lobectomy. Although Robot-L had similar in-hospital mortality compared to VATS-L, patients who underwent robotic approach had reduced LOS but significantly increased patient charges. Further research with emphasis on patient-centered outcomes is warranted to determine the relationship between cost and benefit for patients undergoing robotic lobectomy for lung cancer.
Supplemental Material
Supplemental Material - Comparing Thoracoscopic and Robotic Lobectomy Using a Nationally Representative Database
Supplemental Material for Comparing Thoracoscopic and Robotic Lobectomy Using a Nationally Representative Database by Christine E. Alvarado, MD, Stephanie G. Worrell, MD, Anuja L. Sarode, MPH, Boxiang Jiang, MD, Sean J. Halloran, BS, Luis M. Argote-Greene, MD, Philip A. Linden, MD, and Christopher W. Towe, MD in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
Dr. Towe is a consultant and recipient of a grant for Zimmer Biomet. He is also a consultant for SigMedical, Atricure, and Medtronic. Dr. Worrell is a consultant for Intuitive and Bristol Meyer Squibbs. None of these relationships have affected this manuscript or the accuracy of the data analysis.
Supplemental Material
Supplementary material for this article is available on the Online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.