
Abstract
Background
Seminal trials have demonstrated improved survival in pancreatic adenocarcinoma with novel multiagent chemotherapy regimens. To understand the clinical ramifications of this paradigm shift, we reviewed our institutional experience.
Methods
This retrospective cohort study utilized a prospective database at a single institution to study all patients diagnosed with and treated for pancreatic adenocarcinoma between 2000 and 2020.
Results
1,572 patients were included of which 36% were diagnosed before (Era 1) and 64% after (Era 2) 2011. Survival improved in Era 2 (Median survival 10 vs 8 months, HR .79; P < .001). The survival advantage for Era 2 was primarily seen in patients with high-risk disease (12 vs10 months, HR .71; P < .001). A similar trend was noted for patients undergoing surgical resection (26 vs 21 months, HR .80; P = .081) and with imminently resectable tumors (19 vs 15 months, HR .88; P = .4); however, this was not statistically significant. There was no survival advantage for patients with stage IV disease (4 vs 4 months). Patients in Era 2 were more likely to undergo surgery (OR 2.78; CI 2.00-3.92, P < .001). This increase was driven primarily by increased surgical resection for those with high-risk disease (42 vs 20%, OR 3.74; P < .001).
Discussion/Conclusions
This single institutional study showed improved survival after the shift to novel chemotherapy regimens. This was driven by improved survival for patients with high-risk disease and may be due to more effective eradication of microscopic metastatic disease with adjuvant chemotherapy and increased resection rates.
Key Takeaways
• Pancreatic cancer survival improved following a shift to novel chemotherapy regimens in 2011. • In high-risk pancreatic cancer, patients were downstaged more often following 2011. • In high-risk pancreatic cancer, there were increased rates of surgical resection after 2011.
Introduction
Pancreatic cancer remains a deadly disease. Although pancreatic cancer is the 11th most common cancer, it is the third most common to cause cancer-related death. 1 In addition, 82% of patients have advanced to locally advanced or metastatic disease at presentation with an overall median survival of less than 6 months.
Before 2011, chemotherapeutic regimens for pancreatic cancer consisted of 5-FU or gemcitabine as single-agent therapies or as backbones for doublet regimens.2,3 These chemotherapeutic regimes were associated with only modest improvement in survival and response rates. Two prospective randomized trials published in the New England Journal of Medicine ushered in a new era of effective multiagent chemotherapy.4,5 In these two seminal trials, both FOLFIRINOX and Gemcitabine/nab-paclitaxel were associated with improved survival in the treatment of metastatic pancreatic cancer.4-6 Conroy, et al reported that FOLFIRINOX was associated with improved overall and progression-free survival as well as an improved response rate when compared to gemcitabine alone. 4 Similarly, Von Hoff et al 5 reported that gemcitabine with nab-paclitaxel was associated with improved overall survival compared to gemcitabine alone. FOLFIRINOX and gemcitabine/nab-paclitaxel are now considered the first-line treatments for unresectable and metastatic pancreatic cancer.2,7,8
Surgery is the only curative treatment for pancreatic cancer; however, because of the aggressive nature of this disease, only 10-15% of patients are candidates for upfront surgery. 9 Neoadjuvant chemotherapy with FOLFIRINOX or Gemcitabine/nab-paclitaxel has been associated with downstaging that can increase resectability. 10 Further, recent research has shown a survival advantage with adjuvant chemotherapy. The PRODIGE 24/CCTG PA.6 trial was a prospective randomized trial that showed a survival benefit of nearly 20 months for adjuvant FOLFIRINOX over gemcitabine (54 vs 35 months). 11
Given the improved survival seen with the introduction of these novel multiagent chemotherapy regimens, it is essential to continue to examine the effect this shift in treatment has had on clinical practice. This study examines the clinical ramifications of this change through a single institutional experience. This study aimed to answer the question: has multiagent chemotherapy improved the overall survival of patients presenting with pancreatic cancer?
Methods
Data Collection
This study is a retrospective cohort study utilizing a prospective database at a single institution. All index cases of pancreatic adenocarcinoma at Maine Medical Center from January 1, 2000 to December 31, 2020 were included. Local entries from the NCDB database were used. Subjects with missing data were excluded.
Patients were separated into two discrete groups based on the year of diagnosis. Era 1 included those patients treated January 1, 2000 to December 31, 2010, and Era 2 included those patients treated from January 1, 2011 to December 31, 2020. Further, the dataset was subdivided using the American Joint Commission on Cancer (AJCC) stage into clinical stage groups, including: imminently resectable (AJCC Stage 1A and 1B), high-risk (AJCC Stage 2A, 2B and 3), and stage IV disease. Localized disease refers to all patients with imminently resectable and high-risk disease. The stage was obtained from the NCDB and therefore reflects the AJCC classification system that was utilized at the time the case was original coded. The NCDB was started in 1989 as a joint program of the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society. It is the largest cancer database globally, containing approximately 34 million cancer records from more than 1500 CoC-accredited hospitals in the United States. These data encompass approximately 70% of all patients with cancer diagnoses. 12 The CoC requires that all cancer occurrences be reported to the NCDB annually. Additional data, such as chemotherapy regimen, was obtained from a prospective local tumor registry. The local institutional review board approved this study.
Outcomes
The primary outcome of this study was overall survival. Secondary outcomes included survival based on presentation and whether the patient underwent surgical resection.
Statistical Analysis
Statistical analysis was performed using R software. When assessing differences between patients in Era 1 and Era 2, univariate analysis was conducted using Pearsons Chi-squared test for categorical variables and Wilcoxon Rank Sum or 2-sample T-test for continuous variables. Further univariate and multivariate logistic regression models were used to analyze differences. Odds ratios (OR) and their 95% confidence intervals (CI) were reported. Cox proportion hazard models were used to assess survival. Results were reported as median survival in months or a hazard ratio with CI and P-values. Covariates were controlled for when appropriated including: Age, primary insurance, AJCC clinical stage group, marital status, single vs multiagent chemotherapy, and if patients received radiation or surgery as part of their treatment. Significance was defined at P < .05 for all tests.
The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, Award Number TL1TR002546. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Results
Demographics of All Patients by Era, pancreatic cancer 2000-2020.
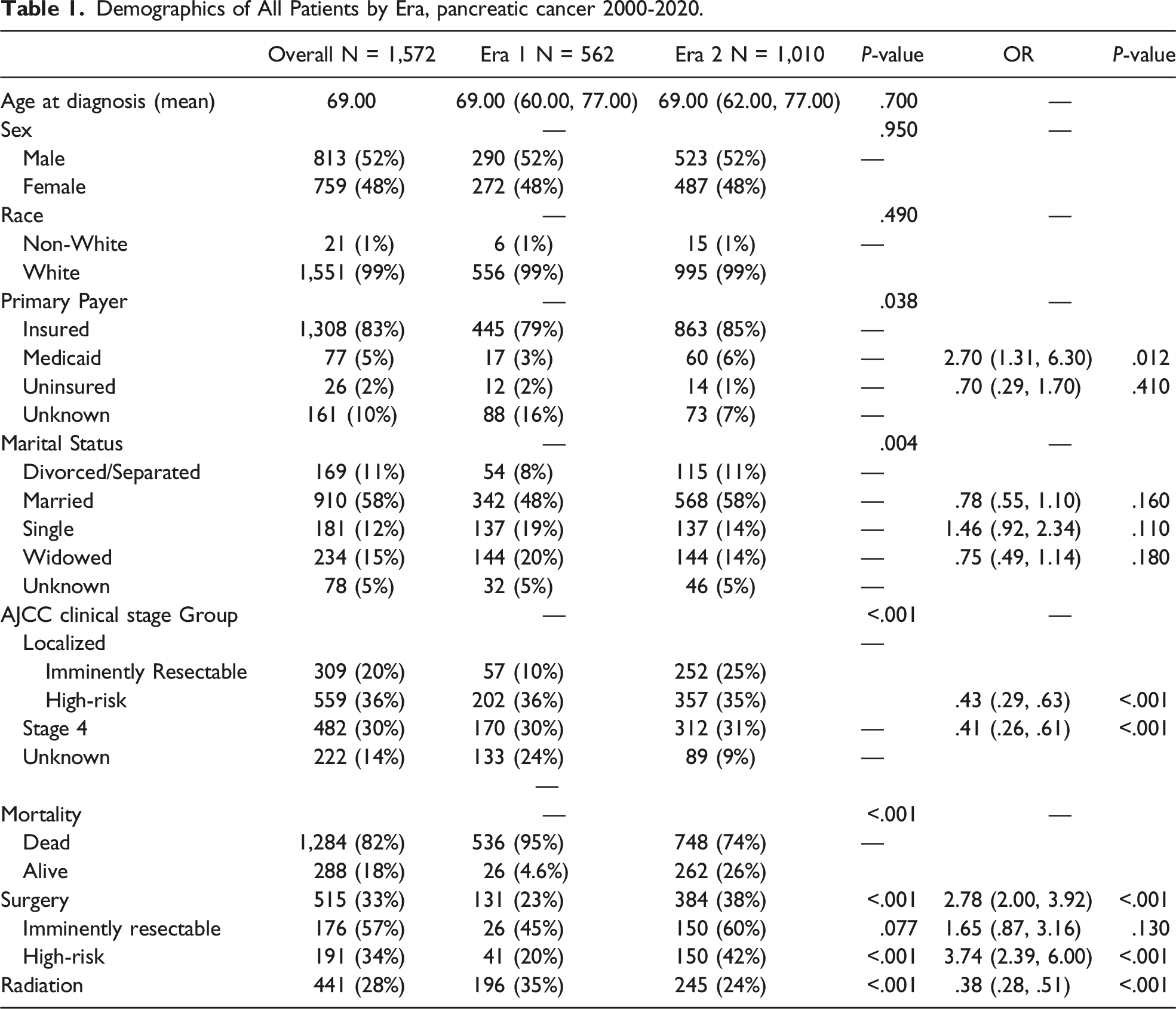
The sample population was divided into two groups. Thirty-six percent were diagnosis before (Era 1, N = 562) and 64% were diagnosed after (Era 2, N = 1,010) January 1, 2011. This date was chosen because it represents the year when the seminal trials for FOLFIRINOX and gemcitabine/nab-paclitaxel were published. Overall, Era 1 and Era 2 groups were comparable. There was no significant difference in age (P = .70), sex (P = .95) or race (P = .49). Those in Era 2 were less likely to present with advanced pancreatic cancer including: high-risk (OR .43; CI 0.29-.63, P < .001) and stage IV disease (OR .41; CI 06-.61, P < .001) (Table 1).
Five hundred fifteen total patients underwent surgical resection. Those in Era 2 were more likely to undergo surgery (OR 2.78; CI 2.00-3.92, P < .001), and this was driven primarily by an increase in surgery for those patients with high-risk disease (42 vs 20%, OR 3.74; CI 2.39-6.00, P < .001). There was no difference in surgical resection rates for those with imminently resectable disease (OR 1.65; CI 0.87-3.16, P = .130) (Table 1).
Survival
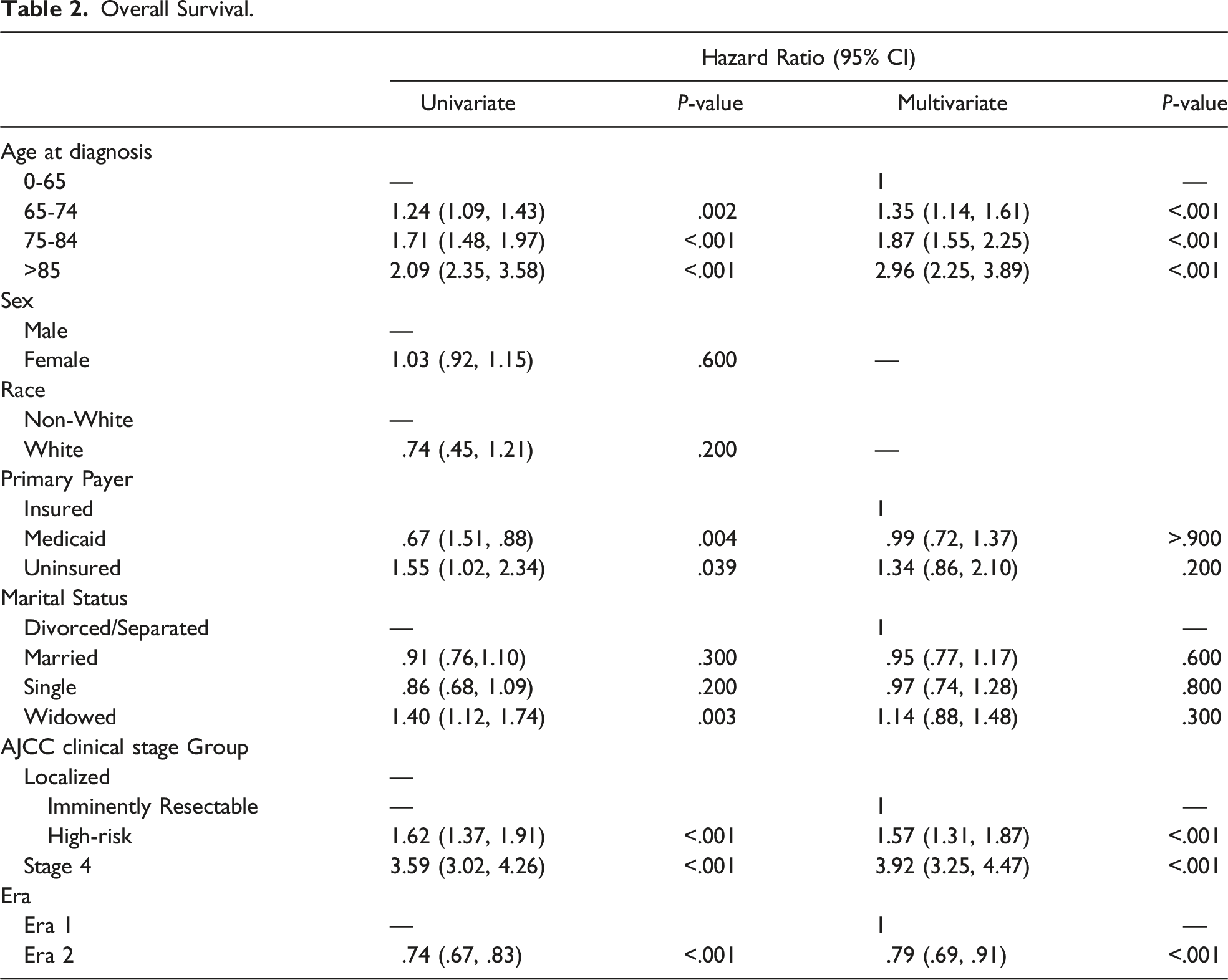
Overall Survival.
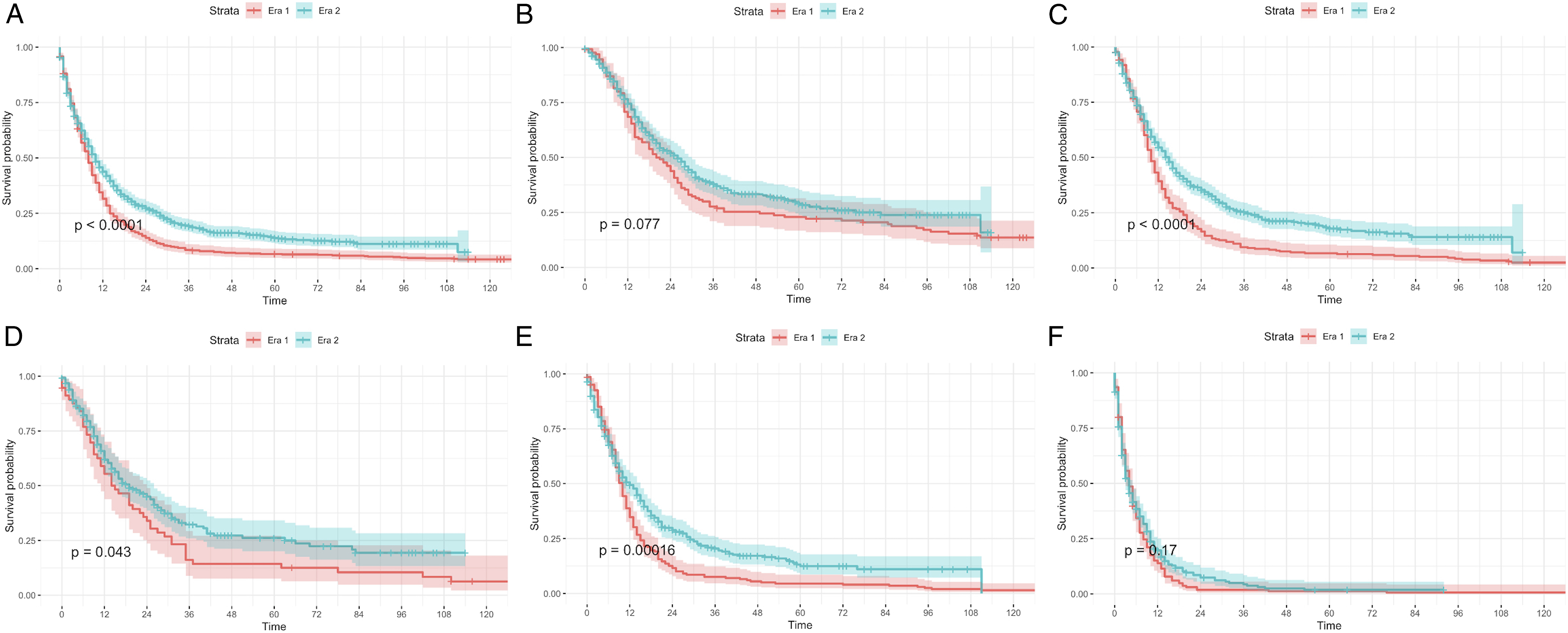
Survival by Era, pancreatic cancer 2000-2020. (A) Overall (B) Surgery patients (C) Localized disease: Imminently resectable and high-risk disease (D) Imminently resectable disease (E) High-risk disease (F) Stage IV disease.
Survival of Subgroups: Era 1 vs Era 2, pancreatic cancer 2000-2020.
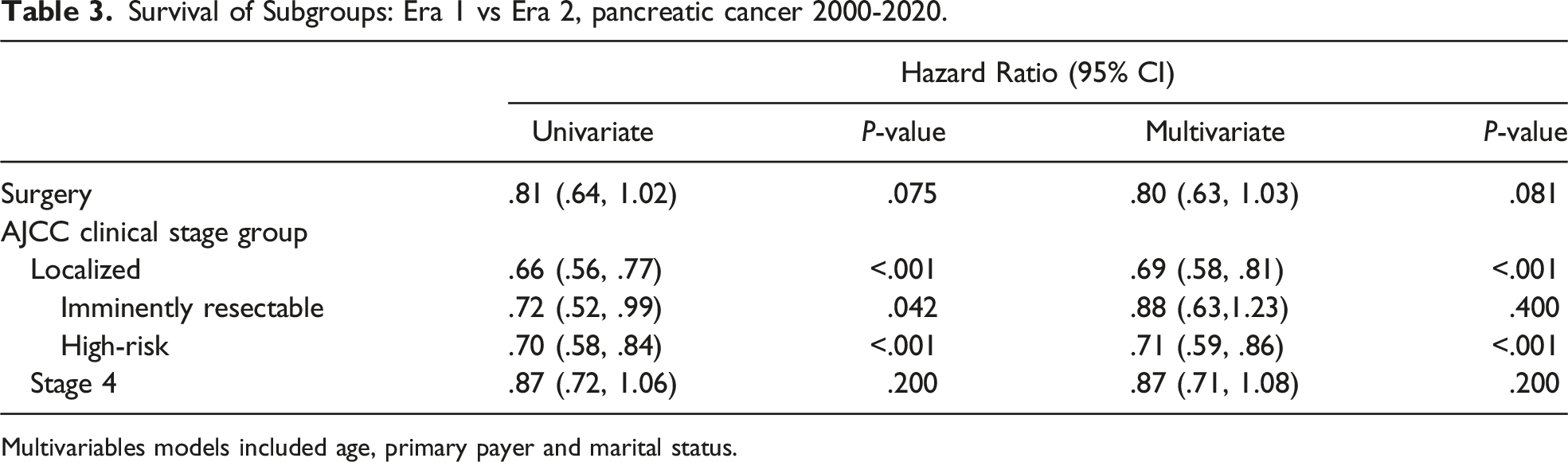
Multivariables models included age, primary payer and marital status.
Chemotherapy Regimens
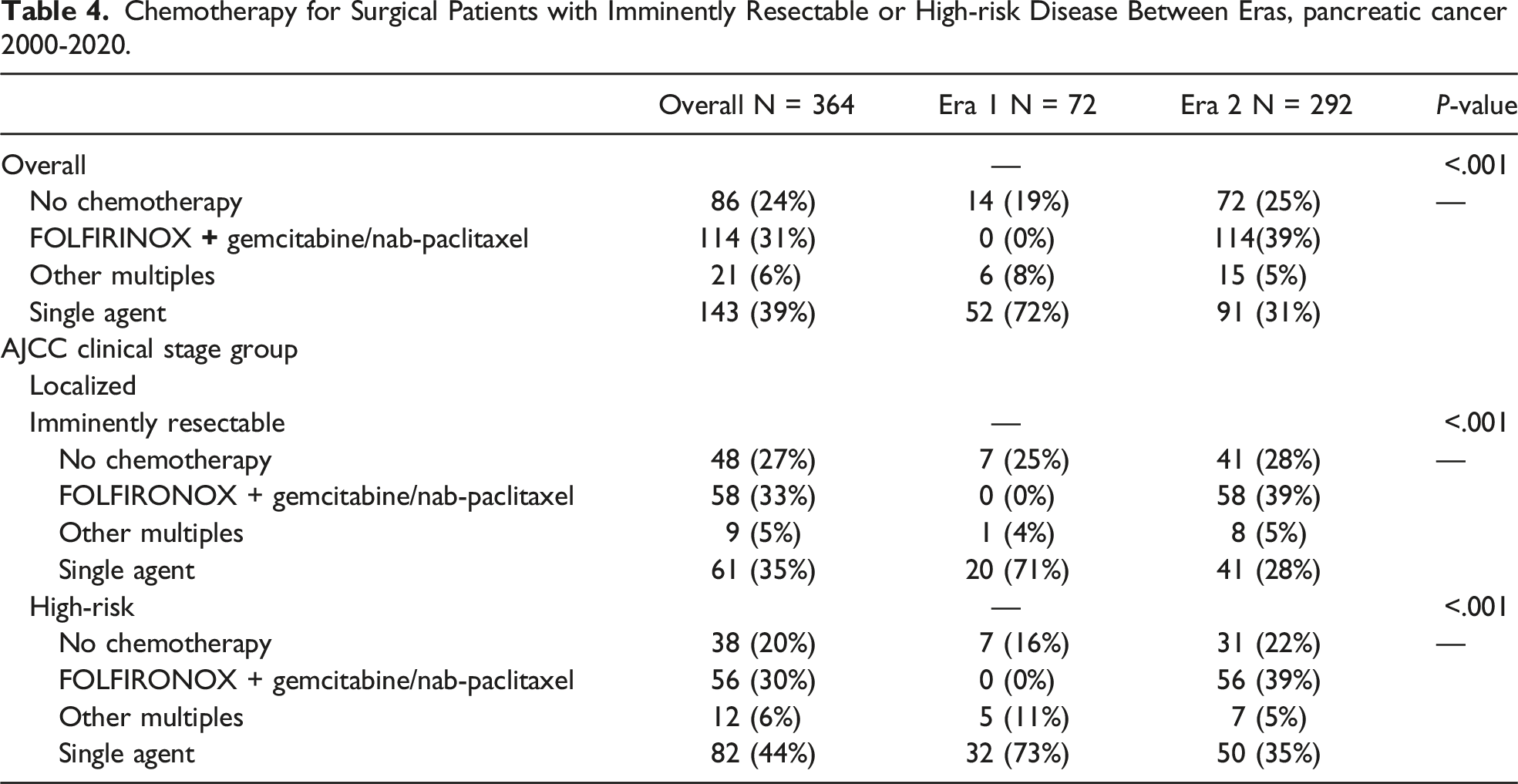
Chemotherapy for Surgical Patients with Imminently Resectable or High-risk Disease Between Eras, pancreatic cancer 2000-2020.
Discussion
Often, pancreatic cancer is diagnosed at advanced stages, and therefore chemotherapy is the first line of treatment. The introduction of increasingly more effective systemic chemotherapeutic regimens, such as FOLFIRINOX and Gemcitabine/nab-paclitaxel, has significantly impacted the treatment of pancreatic cancer. These regimens have become the first-line treatment for patients with locally advanced and metastatic pancreatic cancer. 3
This study aimed to examine the impact of this change in treatment paradigms for all stages of pancreatic cancer. Given that multiple studies have reported improved survival for patients with localized and metastatic pancreatic cancer since the shift to newer multiagent chemotherapeutic regimens, it was hypothesized that survival would improve for all patients diagnosed with pancreatic cancer. All patients at a single institution treated for pancreatic cancer were studied before and after the publication of the use of FOLFIRINOX or Gemcitabine/nab-paclitaxel in the treatment of metastatic pancreatic cancer. An approximate 2 month improvement in overall survival was seen after 2011 (Era 2) compared to those treated before this date.
It was postulated that this improved survival would be seen for all stage categories based on findings of prior publications.4,5,13-15 Surprisingly, no improvement in survival was seen for patients with stage IV disease. Median survival in those with stage IV disease was 4 months in both eras. These findings differ from what has been previously published. The two randomized control studies showed improved survival for those with stage IV disease treated with FOLFIRINOX or Gemcitabine/nab-paclitaxel when compared to gemcitabine alone.4-6 These studies reported a median overall survival of 11.1 months with FOLFIRINOX and 8.5 months with Gemcitabine/nab-paclitaxel, compared to 6.8 and 6.7 months for gemcitabine alone, respectively.4,5 The highly controlled environment of RCTs compared to this pragmatic retrospective study could explain why the small but significant difference seen in the RCT is not discernible in the Stage IV subgroup in this study. Additionally, the smaller sample size in this subgroup could also affect the ability to detect this difference.
The most significant improvements in survival was for patients with localized disease (ie, imminently resectable and high-risk disease). The subset of patients with Stage 1 disease, including 1A and 1B, was analyzed as a single group called imminently resectable because it was felt they reflect a group of patients most likely to have resectable disease and thus, a relatively good prognosis. 16 A trend towards improved survival was noted for patients with imminently resectable tumors with a median survival of 19 vs 15 months.
Unfortunately, from the data, the difference between locally advanced and borderline resectable pancreatic cancer could not be discerned, so these were combine into a single designation, high-risk. The most significant improvement in survival was seen in this group. This high-risk subgroup had a median survival increase to 12 months from 10 with a hazard ratio of .71 (P < .001). This statistically considerable improvement in survival is likely secondary to the use of multiagent chemotherapy for neoadjuvant treatment of these patients. Neoadjuvant therapy can treat microscopic metastatic disease and impact downstaging. 17 It is likely the increased use of FOLFIRONOX after 2011 and Gemcitabine/nab-paclitaxel after 2013 improved tumor response and thus increased the number of patients with resectable disease.
Multiple studies demonstrate improved rates of resection for patients treated with neoadjuvant FOLFIRINOX or Gemcitabine/nap-paclitaxel.14,15,18,19 Hackert et al 13 showed a 61% resection rate in patients with locally advanced cancer who underwent neoadjuvant treatment with FOLFIRONOX. This resection rate was higher than that seen with Gemcitabine alone (46%). Chatzizacharias et al 17 similarly found that 50% of those with locally advanced disease treated with multiagent chemotherapy, including FOLFIRINOX, Gemcitabine/nab-paclitaxel (73%), or other multiagent chemotherapies (27%), were eventually deemed operable. Further, of those who underwent resection, 80% achieved an R0 resection. The median overall survival in this study was 40 months. Finally, Truty et al examined outcomes both in patients with borderline and locally advanced disease. The authors reported significant downstaging and high rates of R0 resections (94%) after treatment with FOLFIRNOX or Gemcitabine/nab-paclitaxel. 10
Patients in the Era 2 cohort were more likely to be treated with surgical resection. Interestingly, there was little difference in surgical resection rates for those with imminently resectable disease; however, those with high-risk disease in Era 2 were 60% more likely to undergo surgical resection. The increased use of surgical therapy in this group is likely secondary to increased downstaging and aggressive surgical approach for patients with localized disease treated with neoadjuvant combination chemotherapy. This aligns well with the reported experience at other high-volume centers outlined above. These studies document downstaging and conversion to a resectable status for patients with borderline resectable and locally advanced pancreatic cancer treated with multiagent chemotherapy.10,13 It is well known that surgical resection is the only curative treatment, and research to this point supports the idea that surgical resection improves survival. 20
This study is not without limitations. First, this study was performed using a single institution’s data. Maine Medical Center serves a primarily white population (99% in this study) and an older than average population, thus bringing in concern for generalizability. Second, other changes in local practice between these two eras could not be accounted for. Although there were no major changes, such as loss of a surgeon, in 2011, the point at which the data was split, general management of this disease would have changes over time that was not able to be captured. For example, there was likely a progressive increased use of imaging over this 20 year time period. Third, as this is a retrospective study there is potential for the usual biases. Fourth, given that this is not an RCT, findings are not as clean; however, an RCT would not be possible for this study, given the design and focus on the shift in practice surrounding 2011. Fifth, there are limitations to using a large national database including the inability to standardize AJCC classifications. Unfortunately there is no standard mechanism to recode AJCC items from one edition to another. Finally, observational studies hold a risk of missing confounding factors that could affect results downstream.
In conclusion, overall survival is improved in pancreatic cancer patients treated after 2011. This data suggested this is multifactorial. First, in this era, better adjuvant therapy likely improves survival by more effective eradication of microscopic metastatic disease. Second, increased surgical resection was noted in all localized groups but was particularly distinct for patients with high-risk disease, including those with locally advanced and borderline resectable tumors. Likely, this is due to improved rates of downstaging and the resulting increased number of patients with potential for a negative margin resection. Third, there was an increased resection rate even for patients with imminently resectable tumors. This may reflect decreased negative opinions towards surgical exploration for local pancreatic cancer. This increased use of surgery, the only potentially curative treatment, is likely a primary reason for the improved overall survival rates. Finally, and most surprising, there is no increase in survival for patients with stage IV cancer. This is likely secondary to the small number of patients in this subgroup and the modest improvement in survival.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, Award Number TL1TR002546 and TL1TR002546-04 is the more specific number for Laura Nicolais grant.