
Abstract
Objectives
Pan scanning in trauma patients has become routine, resulting in increased identification of incidental findings (IF), findings unrelated to the reason for the scan. This has posed a conundrum of ensuring patients have appropriate follow-up for these findings. We sought to evaluate our compliance and follow-up for patients after implementation of an IF protocol at our level-I trauma center.
Methods
We performed a retrospective review from 9/2020 to 4/2021, to encompass before and after protocol implementation. Patients were separated into PRE and POST groups. Charts were reviewed evaluating several factors including three- and six-month follow-ups on IF. Data were analyzed comparing PRE and POST groups.
Results
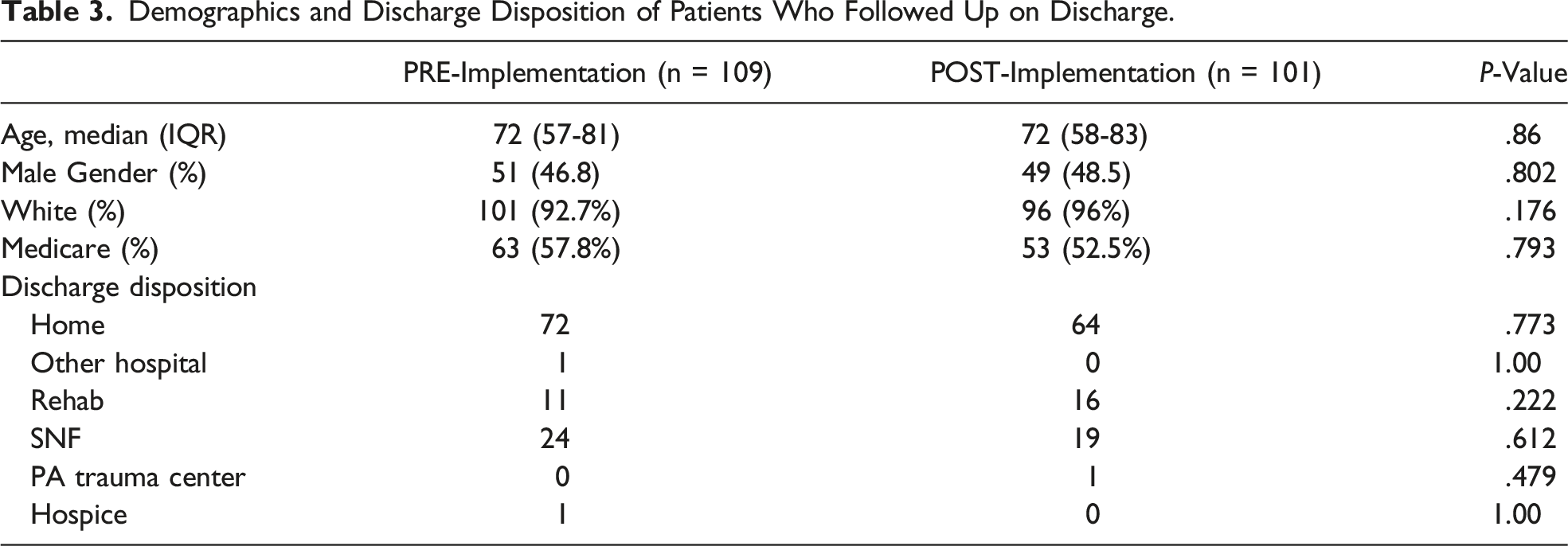
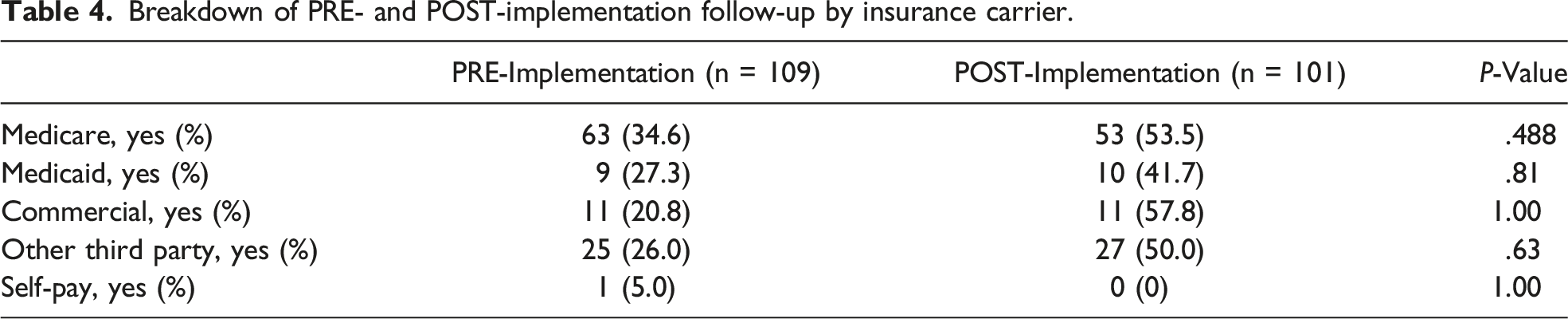
A total of 1989 patients were identified, 31.22% (n = 621) with an IF. 612 patients were included in our study. Compared to PRE, POST showed a significant increase in PCP notification (35% vs 22%, P < .001) and patient notification (82% vs 65%, P < .001). As a result, patient follow-up regarding IF at six months was significantly higher in POST (44%) v. PRE (29%), (P < .001). There was no difference in follow-up based on insurance carrier. There was no difference in patient age for PRE (63 y) and POST (66 y) overall, (P = .089); nor in age of patients who followed up; 68.8 PRE vs 68.2 years POST (P = .819).
Conclusion
Implementation of an IF protocol with patient and PCP notification was significantly improved in overall patient follow-up for category one and two IF. Utilizing the results of this study, the protocol will be further revised to improve patient follow-up.
Key Takeaways
Implementation of an Incidental Findings protocol improves patient follow-up for critical incidental findings. Patient follow-up for incidental findings is unaffected by insurance carrier or discharge disposition. Patient and PCP notification are effective ways of improving patient follow-up.
Introduction
CT scanning has become the standard of care for evaluation of hemodynamically stable trauma patients. Several studies have shown a survival benefit with routine whole body CT scanning in trauma.1-5 Recent increases in the use of routine CT scan in trauma patients have resulted not only in improved identification of traumatic injuries but also a higher frequency of incidental findings. Incidental findings are discoveries from CT scans unrelated to the initial injury or reason for scan.2,3 These incidental findings vary in significance from trivial to life threatening. Unfortunately, incidental findings are often overlooked as trauma teams focus on acute injuries. Several methods have been suggested to improve overall recognition of and follow-up for incidental findings. Electronic medical records and improved communication with patients and primary care providers (PCPs) have been proposed as means of improving incidental finding management. The REACT-2 Trial found that more clinically significant incidental findings are identified on routine total body CT scan as than selective CT scanning in trauma patients. 6
Some studies have reported incidental findings on trauma CT scans as low as 3%, but a larger study analyzing 2000 patients reported 39% of patients had category one or two incidental findings.2-5 Other studies have identified category one or two incidental findings in over 73% of patients. 7 With the percentage of incidental findings upward of more than half of all trauma patients, there is a need to better identify and communicate pertinent findings to patients and providers.
Incidental findings are divided into four categories depending on significance. Category one findings require urgent treatment or further evaluation. Category two findings necessitate further evaluation and follow-up in 3-6 months. Category three findings have no immediate projected consequences without treatment but may be potentially relevant in the future, and category four findings are considered harmless. Historically, focus on reporting incidental findings has largely centered around category one and two findings given the more imminent clinically significant nature.
The increasing number of incidental findings on trauma CT scans has led to a novel focus on ensuring patients are aware of these findings and have appropriate follow-up. While several studies over the last decade have evaluated the percentage of patients who will have an incidental finding on CT scan, few studies have specifically evaluated patient follow-up for category one and two findings. Divine et al reported 242 of 392 patients with incidental findings did not have follow-up, or that their particular findings were not adequately communicated to them. 8 Grattan et al expanded on this finding by recognizing that few patients are even given documentation for follow-up regarding their incidental findings. 9 Another study identified 43% of included trauma patients as having had an incidental finding on a CT abdomen/pelvis, yet only 27% of those patients had any documentation of the finding. 10
With increasing numbers of CT scans being performed on trauma patients and recent reports of clinically significant incidental findings found in up to 39% of trauma patients, development of a protocol to ensure appropriate follow-up is imperative.1-4 Documentation of incidental findings had been inconsistent at our busy level-I trauma center. With the goal of improving our overall patient follow-up for these critical incidental findings, we implemented an incidental finding protocol. This protocol included patient (or proxy) notification of the finding, documentation of the findings, and notification being sent to patients’ PCP via a letter. This study aims to analyze whether implementation of this protocol resulted in improved patient notification and follow-up regarding both category one and two incidental findings at a level- I trauma center in rural Pennsylvania. We hypothesized that this protocol would lead to improved patient notification and follow-up.
Materials and Methods
Following Institutional Review Board approval, we performed a retrospective review utilizing our trauma registry and the medical record from September 2020 through April 2021. The incidental findings protocol was implemented beginning in January of 2021. This protocol implementation stemmed from poor patient follow-up for incidental findings. The protocol involved identifying patients or their proxies with an incidental finding, both in person and in writing. Additionally, a letter was sent to the patient’s PCP with the overall goal of improving patient follow-up.
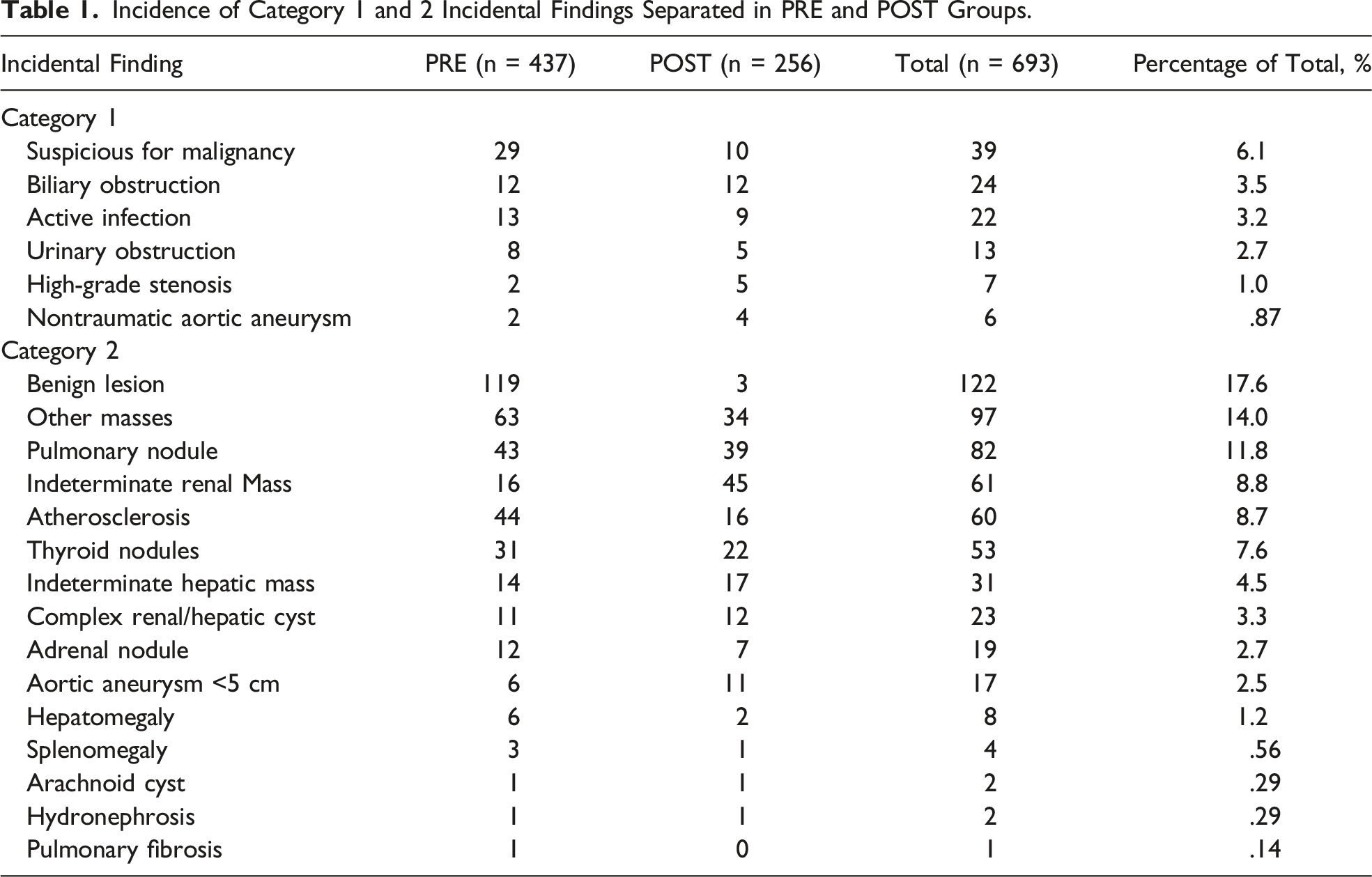
The pre-protocol implementation group was from September 2020 to January 2021. The post-protocol implementation group was from January 2021 to April 2021. All patients presenting with a traumatic injury during the query period were included in the study. Charts were reviewed to obtain information on relevant variables. These variables included age, sex, race, ethnicity, insurance type, hospital length of stay (LOS), mechanism of injury, discharge destination, presence of an incidental finding, patient follow-up regarding incidental finding, and patient’s PCP information. Information regarding only category one and two incidental findings was collected. Category one incidental findings include suspicious for malignancy, non-traumatic aortic aneurysm > 5 cm, high-grade stenosis (>80%), active infection, biliary obstruction, and urinary obstruction. Category two incidental findings included aortic aneurysms <5 cm, pulmonary fibrosis, pulmonary nodule, atherosclerosis, arachnoid cyst, hepatomegaly, indeterminate renal mass, indeterminate hepatic mass, splenomegaly, hydronephrosis, benign lesions, and other masses. Additional information collected included patient follow-up at three-month and six-month intervals. Univariate statistical analysis was conducted using one-way ANOVA, T tests, and Chi-square tests to determine associations between the two groups.
Results
A total of 1989 patients were identified, 31.22% (n = 621) of whom had incidental findings. Nine patients were excluded for missing data, leaving 612 patients included in the study. In the pre-implementation (PRE) group, 35.4% of patients had an incidental finding compared to 26.0% of patients in the post-implementation (POST) group. No statistically significant difference was observed in any demographic-related patient factors between the PRE and POST group, including sex, age, or ethnicity.
Incidence of Category 1 and 2 Incidental Findings Separated in PRE and POST Groups.
Breakdown of PRE and POST Implementation Groups.

Demographics and Discharge Disposition of Patients Who Followed Up on Discharge.
Breakdown of PRE- and POST-implementation follow-up by insurance carrier.
Discussion
Our study hypothesized that the implementation of an incidental finding protocol would improve follow-up for critical incidental findings. We demonstrated that the implementation of the protocol at our level-I trauma center in Pennsylvania led to improvements in patient notification, PCP notification, and patient follow-up. Our study shows that the implementation of a protocol that is largely led by advanced practice providers and surgical residents can improve overall patient knowledge and follow-up rates for incidental findings. Given the urgent nature of some incidental findings, increasing patient and provider awareness of these findings can help to extend patient lives and improve overall outcomes. Our current protocol for recognition and notification of incidental findings has changed since initial inception. This protocol now includes notifying the patient in person and in the discharge summary of these findings, sending a letter to the PCP, and adding these incidental findings to the patient’s active problem list in the electronic medical record.
It is important to recognize that some incidental findings are critical and time sensitive; however, most incidental findings are of little to no clinical relevance. 11 The goal of our study was not to force follow-up for these incidental findings but rather to notify patients and PCPs in case additional workup or monitoring was warranted. The rate of incidental findings in our study, 31%, was comparable to many other studies.1-3,5,9 Studies have cumulatively reported 7-70% of patients with IFs, with the majority of studies falling in the range of 15-40%.1-5,9,11
Our study shows a significantly higher percentage of patient notification when compared to similar studies. Overall, 71.8% of our patients were notified of their incidental finding. Ekeh et al documented only 21% of patients with incidental findings were notified. 10 Munk et al noted that only 27% of patients with incidental findings were notified. 3 Despite an improvement in PCP notification from our PRE to POST group, compliance can certainly be improved upon, as it remained low/suboptimal in the POST group. This is likely due to rotating surgical residents and difficulty confirming every member of the team comprehensively understood the protocol. Our team is actively working to rectify this by increasing compliance with patient and PCP notification.
Several other institutions have implemented an incidental finding protocol.12-14 Collins et al demonstrated an 80% improvement in patient notification of an incidental finding following the implementation of a protocol. 13 The protocol implemented by Collins et al was like our protocol with patient and PCP written notification. Sperry et al implemented a protocol for incidental findings notification through the addition of a dedicated incidental findings coordinator. 12 Sperry demonstrated a 95% patient notification and initiation of patient follow-up after the implementation of this dedicated coordinator. 12 Oliverio Fihleo et al implemented a unique protocol where a code was attached to each radiology report for each incidental finding; this was then reviewed by a dedicated medical team who notified the patient and aided the patient in initiating follow-up. 14 Huhyn et al demonstrated the implementation of an incidental findings protocol that was performed in conjunction with the tertiary survey. 15 Yeh et al demonstrated a 91% patient follow-up for incidental findings for those patients that had post-injury PCP appointments. 16 Overall, our study shows that the implementation of an incidental finding protocol at a level-I trauma center resulted in significantly higher rates of patient and PCP notification, as well as overall six-month patient follow-up for these critical findings.
There are several limitations to our study. First, it was performed at a single institution, so our data and corresponding conclusions may not be applicable to all hospitals. Regarding our methodology, it is conceivable that some patients’ incidental findings were communicated to them, but communication was not documented in the patients’ charts. This could explain why the percentage of patient notification is lower than expected. There is no national or standardized system for categorizing incidental findings, which is a complicating factor as it is difficult to compare our study to other studies as there is no standardization of incidental findings reporting. Additionally, several of our patients had PCPs that were not in our health system. This made it very difficult to determine if these patients followed up for their findings. Several of our patients were uninsured, which could complicate the follow up rates due to inability to pay out-of-pocket for future visits. Furthermore, our study was conducted during the fall and winter, when trauma services generally tend to see fewer patients. In practice, our protocol can be time consuming if a patient’s PCP is not in our health system, which may render it difficult to ensure compliance in the busier summer months.
In conclusion, our study shows that the implementation of an incidental finding protocol involving patient and PCP notification resulted in significantly higher rates of patient follow-up for critical incidental findings. Additional research is warranted to evaluate the cost on the healthcare system of implementing an incidental finding protocol akin to the one in our study. While our protocol improved overall patient follow-up, additional studies are needed to determine if the improved follow-up resulted in improved patient outcomes. Further studies evaluating any additional workups performed after patient follow-up would help to better evaluate the efficacy of this protocol in changing overall patient outcomes for various disease processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.